
Abstract
Purpose:
To report the 5-year clinical efficacy of PRP intra articular injections in knee osteoarthritis (OA) and to investigate the risk factors predictive for treatment failure and poor clinical outcome.
Methods:
We retrospectively evaluated 118 patients treated for low to moderate knee OA demonstrated by X-Ray and magnetic resonance imaging (MRI) with autologous PRP injection from 2014 to 2018 with a mean 51.1 ± 14.8 (range 29 to 89) months follow-up. All the patients were evaluated with Lysholm and WOMAC score. The role of Kellgren Lawrence (KL) grade, patello-femoral (PF) degeneration, age, body mass index (BMI), relevant comorbilities, smoking status, gender, previous surgery or conservative measures were analyzed with univariate and multivariate analysis.
Results:
There was a significant improvement of all outcome measures at final follow-up and high satisfaction rate (79.7%). The overall failure rate was of 15.3% after a mean of 57.7 ± 15.1 (range 33 to 85) months. The BMI and the KL grade were identified as significant independent risk factor related to failure of autologous PRP injection. Patients under 60 reported significantly higher Tegner activity scale (p = 0.032) at final follow-up. Patients with KL grade 3 and patients with PF MRI-KL grade 3 had significantly lower Lysholm scores (p = 0.026 and p = 0.042 respectively) at final assessment. Younger patients with lower BMI and lower grade of radiographic OA had significantly longer therapeutic benefit (p < 0.05).
Conclusion:
Intra articular PRP injections led to a significant clinical improvement in middle-aged adults with a low to moderate knee OA. BMI and high KL grade have been identified as significant risk factors predictive for failure at mid-term follow-up.
Introduction
Knee osteoarthritis (OA) is a degenerative joint disease affecting 250 million people worldwide that leads to gradual degradation of articular cartilage, degenerative changes of subcondral bone, reduced viscosity of the articular fluid and chronic inflammation of synovial membrane. 1 The progressive aging of population inevitably causes an increasing incidence of OA and a negative impact on the quality of life of affected patients. 2
The current conservative strategies for the treatment of knee OA include physical therapy, weight loss, oral and topical NSAIDs and intra-articular injections. 3 However, there is an increasing interest in biologic therapies and regenerative medicine for the management of degenerative musculoskeletal disorders. Platelet rich plasma (PRP) is elaborated by processing and centrifugation of blood (autologous or from donor) to obtain plasma with high concentration of platelets. 4 The activity of PRP is mediate by many components as cytokines and growth factors that create a regenerative and anti-inflammatory action on musculoskeletal tissues. 5,6 PRP injections demonstrated great efficacy for degenerative cartilage disease in high level of evidence studies. 7 –9 Nonetheless, there is a lack of uniformity in indications, inclusion criteria and classifications among published researches leading to variable outcomes and contrasting findings. 7,8,10 To the best of our knowledge, the risk factors predictive for failure of PRP injections for the treatment of knee OA has not been extensively investigated.
The purpose of this retrospective study is to report the 5-year clinical efficacy of PRP intra articular injections in knee OA and to identify the risk factors predictive for failure.
Materials and methods
Selection of patients
Ethical approval for the present study was requested and obtained from the institutional review board (number 1882019). We retrospectively reviewed all patients treated consecutively with intra-articular PRP injection from January 2014 to march 2018.
The indication for PRP intra-articular injections was patients under 80 years old with symptomatic low to moderate knee OA demonstrated by clinical and imaging investigations.
The inclusion criteria were knee pain and functional impairment, presence of low to moderate knee OA demonstrated by X-Ray and 1.5 Tesla magnetic resonance imaging (MRI).
Exclusion criteria were patients with less than 24 months follow-up, previous history of knee trauma such as fracture or dislocation, ligament laxity, severe knee OA, varus or valgus mechanical axis (>5 degrees from neutral), MRI evidence of bone marrow lesions, previous conservative strategies (physical therapy, NSAIDs and injections) within the 6 months preceding the PRP treatment and incomplete medical or imaging records.
Medical records were retrieved and analyzed and data of age, sex, smoking status, previous surgeries, therapies and comorbidities were collected.
The hospital protocol included a baseline clinical examination conducted by a trained orthopedic fellow using the Lysholm Score, 11 Western Ontario and McMaster Universities Arthritis Index (WOMAC). 12 The Tegner Activity Scale (TAS) 13 was used to quantify the grade of sport activity, the visual analogue scale (VAS) 14 was used to assess the level of pain.
The radiographic grade of OA was classified with Kellgren-Lawrence (KL) system 15 and the patello-femoral (PF) degeneration was assessed with the MRI based Kellgren Lawrence (MRI-KL) grading tool for PF joint. 16 Low to moderate OA was considered as KL grade 1 to 3. Patients with severe knee OA (KL grade 4) or normal findings (KL grade 0) were excluded from the study.
Patients were called to be clinically reassessed with the same clinical protocol at final follow-up evaluation. Duration of symptoms relief was recorded and the satisfaction was investigated with a rating scale from 0 (no benefits) to 10 (maximum satisfaction).
Failure was defined as the need for surgery or recurrence of symptoms within the 6 months following the first PRP injection.
The primary outcome measures were considered the Lysholm and WOMAC scores.
Secondary outcome measures were considered the failure rate, the subjective satisfaction and the duration of symptoms relief.
The role of KL grade, age, BMI, comorbilities, smoking status, gender, previous surgery or conservative measures were analyzed with univariate and multivariate analysis to identify the predictive risk factors for failure.
PRP preparation
Every patient was screened with routine blood count, electrocardiogram and general consultation performed by transfusion medicine specialist before PRP preparation.
A standard blood bag sample (450 mL) was taken from each included patient and managed by the Department of Transfusion Medicine. The blood underwent a standardized preparation with three consecutive centrifugations (Hettich Zentrifugen®; Hettich Lab technology, Tuttlingen, Germany): the first at 3550 r/min for 12 min, the second at 1100 r/min for 10 min, and the third at 2600 r/min for 20 min. The final product was than filtered and frozen (–80°C) in four test tubes for cryopreservation.
The PRP platelet (PLT) concentration ranging from 250,000 to 900,000 per mL, with a mean value of 600,000 PLT/mL. Moderately elevated PLT concentration demonstrated optimal biological effects on musculoskeletal tissues. Leukocytes (WBC) were filtered during preparation with low concentration in the final product (<1,000 WBC/mL). No activating agents were added.
We injected 5 mL of PRP once a week for four consecutive weeks. No medications were prescribed, and self-medication with NSAIDs was strongly discouraged. Exercise or physical therapy was not formally prescribed, and patients were asked to gradually return to their normal working, recreational or sporting activity following the last injection.
Statistical analysis
A post-hoc power calculation was performed considering the final Lysholm score as the primary outcome measure. With the Lysholm value of 58.1 ± 25.7 points reported in the literature for patients affected by knee osteoarthritis 17 and the probability of type I error with α value of 0.05, the resulted post-hoc power of the present study on 118 patients was Φ (11.7) corresponding to 100% of power.
Categorical variables were expressed as the absolute number of cases and percentage.
The Shapiro-Wilk Test was used to identify normally distributed parameters.
Differences between means were calculated with the T-test for continuous variables or with the Mann-Whitney U test if not normally distributed. The non-parametric Wilcoxon Signed Rank test was used to compare continuous matched pre-operative and final data. Categorical variables were calculated using the Chi-square test or Fisher’s exact test.
The analysis of variance (ANOVA) was used to compare means of continuous normally distributed variables in two or more independent comparison groups. The Kruskal-Wallis test was used for not normally distributed variables.
The non-parametric Spearman’s rho coefficient was used to assess correlation between continuous or ordinal values.
Variables achieving the p value <0.1 in univariate analysis were examined using multivariate logistic regression analysis and backward selection process. Kaplan-Meier survival function curves were created using all parameters to analyze failure rate for any reason. The significance threshold for tests was set at p < .05.
Results
A total of 173 patients underwent PRP injection within the indexed period and 55 among them were excluded (20 underwent other conservative measures within the previous 6 months, 14 had incomplete medical records, 11 showed ligament laxity, 7 were untraceable and 3 had severe varus deformity).
One-hundred-eighteen patients (118 knees) with knee OA were finally included with a mean 51.1 ± 14.8 (range 29 to 89) months follow-up.
Demographic data and characteristics of patients at baseline evaluation are reported within Table 1.
Demographic data and characteristics of patients at baseline evaluation.

Data are presented as mean value or number (percentage).
APM: arthroscopic partial meniscectomy; BMI: body mass index; HA: Hyaluronic acid; KL: Kellgren Lawrence; MRI-KL: magnetic resonance imaging based Kellgren Lawrence grade; L: left side; R: right side; VAS: visual analogue scale; WOMAC: Western Ontario and McMaster Universities Arthritis Index.
* Significant p value represents not normally distributed variables (Shapiro-Wilk test).
† Classified with MRI-based Kellgren Lawrence grading tool for patellofemoral joint.
‡Maximum perceived pain during the day.
There was a significant improvement of all outcome measures at final follow-up. Results are showed within the Table 2.
Overall results of outcome measures and differences from baseline to final follow up.

Data are presented as mean value, standard deviations and ranges.
TAS: Tegner Activity Scale; VAS: visual analogue scale; WOMAC: Western Ontario and McMaster Universities Arthritis Index.
* Significant p value (Wilcoxon signed rank test)
† Maximum perceived pain during the day.
The reported main value of subjective satisfaction at the end of follow up was 7.8 ± 1.7 (range 4 to 10). Ninety-four (79.7%) patients reported a value of subjective satisfaction at latest follow-up from 7 to 10. Fifty (42.4%) patients repeated more than one PRP treatment during the follow-up (42 patients had 2 treatments, 6 patients had 3 treatments and 2 patients had 4 treatments). The PRP injections were repeated after a mean of 24 ± 8.3 (range: 12 to 34) months from the baseline.
The overall failure rate was of 15.3% (18 knees) with 18 patients underwent subsequent surgery for symptoms persistence after a mean of 57.7 ± 15.1 (range: 33 to 85) months (Figure 1).

Kaplan Maier survival function of 118 patients underwent autologous PRP injections.
There was no significant difference of failure rates within sub-groups of patients stratified for comorbilities, smoking status, gender, previous surgery and previous hyaluronic acid injections.
However, patients underwent previous steroid injections, BMI > 25, KL > 2 and age > 60 showed significantly higher failure rate. Table 3 shows the details of univariate analysis of risk factors for failure.
Univariate analysis of risk factor predictive for failure of PRP treatment.
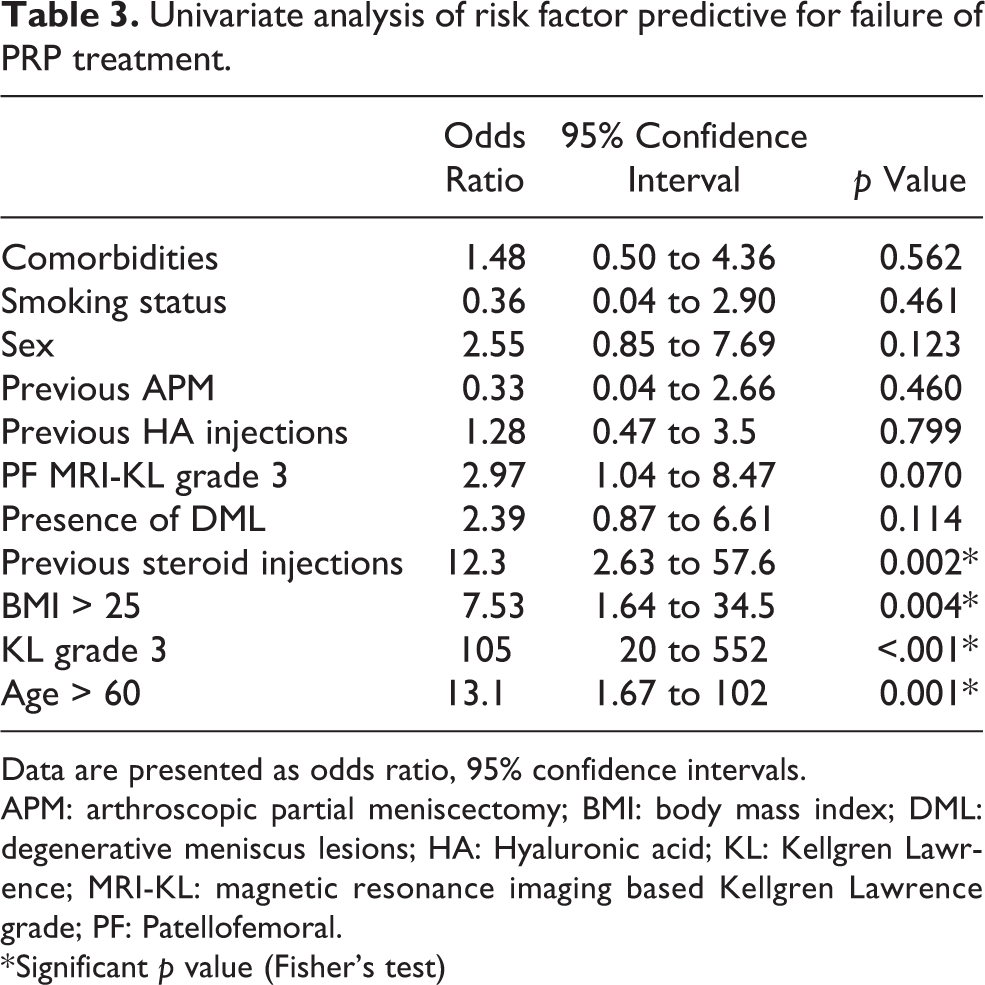
Data are presented as odds ratio, 95% confidence intervals.
APM: arthroscopic partial meniscectomy; BMI: body mass index; DML: degenerative meniscus lesions; HA: Hyaluronic acid; KL: Kellgren Lawrence; MRI-KL: magnetic resonance imaging based Kellgren Lawrence grade; PF: Patellofemoral.
* Significant p value (Fisher’s test)
The logistic regression model identified the BMI and the KL grade as significant independent risk factor related to failure of autologous PRP injection. Age, PF MRI-KL grade and previous steroid injections were not confirmed (p > 0.05) at multivariate analysis (Table 4).
Logistic regression model of failure risk factors.

BMI: body mass index; KL: Kellgren Lawrence; MRI-KL: magnetic resonance imaging based Kellgren Lawrence grade; PF: patello-femoral.
*Significant p values.
A significant correlation between BMI, age and KL grade has been found.
The analysis of outcome measures within subgroup of patients stratified for age, BMI, previous steroid injections, KL and PF MRI-KL grade grade was performed.
Patients under 60 reported significantly higher Tegner activity scale (p = 0.032) at final follow-up. Patients with KL grade 3 and patients with PF MRI-KL grade 3 had significantly lower Lysholm scores (p = 0.026 and p = 0.042 respectively) at final assessment.
No differences between other outcome measures were found.
The main duration of symptoms relieve after autologous PRP injection was 11.1 ± 6.2 (range 0 to 40) months. Younger patients with lower BMI and lower grade of radiographic OA had significantly longer therapeutic benefit (p < 0.05). Furthermore, sub-group of patients with PR MRI-KL grade 3 or patients who underwent previous steroid injections had significantly shorter benefit (p < 0.05). Details are showed within the Table 5.
The stratified results of duration of symptoms relief in patients underwent PRP injections.

BMI: body mass index; KL: Kellgren Lawrence; MRI-KL: magnetic resonance imaging based Kellgren Lawrence grade; PF: patello-femoral.
*Significant p values.
Discussion
According to the main findings of this study, intra articular PRP injections led to a significant clinical improvement in middle-aged adults with a low to moderate knee OA. Moreover, this research allowed to identify the risk factors predictive for failure at mid-term follow-up.
In the last few years the use of intra articular PRP injections for knee OA has been widespread, thanks to their regenerative potential and inflammatory modulation. 5,6,18
Several studies reported early benefits of PRP injection for early knee OA, 19 –22 but the mid to long-term efficacy is still unclear. 23,24
The present research showed that intra-articular autologous PRP injection provides a significant improvement of WOMAC, Lysholm, TAS and VAS score up to 5 years. The secondary aim of this study was to identify the potential risk factors predictive for failure of PRP treatment since only few studies in the literature has been selectively focused on this specific topic. 25 –28 Korpershoek et al. 25 reported inconsistent findings correlating the clinical outcome of PRP treatment and demographic factors (sex, age, BMI, KL grade, history of knee trauma, and baseline KOOS). Nonetheless, other studies identified a significant correlation between clinical outcome and age 26,27 and BMI. 28
The present research demonstrated that BMI and KL grade independently affected the risk of failure of PRP treatment. In particular, patients with lower BMI and KL grade showed better and lasting results and lower failure rate. According to our results, Filardo et al. 28 identified that BMI significantly influenced the clinical outcome with a trend to reduce the duration of beneficial effect of PRP injections although with limited follow-up and a small sample size.
Regarding age, some studies demonstrated poor clinical results in old patients who underwent PRP injections. 26,27 The present research showed that age represent a potential risk factor related to failure of PRP injections, but it was not confirmed as independent risk factor at multivariate analysis suggesting a potential confounding role of other variables. Nevertheless, we point out that patients older than 60 had a significantly shorter therapeutic benefit.
A recent consensus 29 described the low to moderate knee OA as proper indication for PRP injections. A careful patient selection is recommended because severe radiographic changes appeared to be correlated to poor clinical outcome. 30
This study investigated the presence of MRI degenerative changes in all the included patients, in particular the PF degeneration and the presence of degenerative meniscus lesions. Jang et al. 31 showed that the PF OA is associated with a poor clinical results and shorter patient’s benefit. Our results demonstrated that, although patients with PF degeneration showed a significantly shorter benefit, the PF MRI-KL grade did not influence the clinical outcome and the failure rate up to 5 years. However, we point out that patients with severe PF changes (MRI-KL grade 4) were not included in the present research as PRP injections are not a proper indication for this specific condition. Raeissadat et al. 32 measured the clinical outcome and the MRI changes of PF joint in patients underwent PRP and exercise or exercise alone and demonstrated a significant improvement of cartilage volume in patients underwent PRP injection. All these findings suggest that the presence of moderate PF OA is not a contraindication for autologous PRP injection, but patients should be informed that clinical benefits could be limited.
The presence of degenerative meniscus lesions, did not influence the clinical outcome of PRP treatment and there was a clinical improvement in all affected patients analogously to other research investigating patients without knee OA. 33 Mitev et al. 34 showed a clinical improvement in patients with articular cartilage and degenerative meniscus lesions. Raeissadat et al. 32 showed that PRP injection and exercise improve the MRI signal of degenerative meniscus and the same results had been found by Özyalvac et al. 35 but the patients underwent intra-meniscal injection with ultrasound.
The use of steroid injections showed a potential impact on treatment failure, even if the injection is delayed of more than 6 months, and all patients underwent previous steroid injections had significantly shorter benefit. This was not confirmed for hyaluronic acid injections as no differences were found. It’s well known that corticosteroids have a catabolic activity of PRP and Eymand et al. 29 recommend a delay if steroids are injected before PRP. Nevertheless, Camurcu et al. 36 demonstrated that single steroid injection followed by PRP 1 week later improve the clinical response in patients with low or moderate knee OA. Although, these contrasting results, from our opinion corticosteroids injections should be avoided as first line strategy, especially in younger patients who could benefit from PRP injections.
The heterogeneity of available PRP products (number of platelets and leukocytes, amount of growth factors and pro- or anti-inflammatory cytokines) and unstandardized protocols both leads to variable clinical results and contrasting findings. 29,37 A precise, stepwise and detailed description of the preparation protocol is mandatory to provide the reproducibility and the efficacy of this therapeutic strategy.
This study has several limitations; first of all, this is a retrospective series and, although well powered, a priori sample size was not calculated. Second, the outcome measures are based only on clinical evaluation, without systematic imaging follow-up nor arthroscopic findings. Finally, although the strict inclusion and exclusion criteria, there are potential confounding variables due to heterogeneous study population.
Conclusion
Intra articular PRP injections led to a significant clinical improvement in middle-aged adults with a low to moderate knee OA. BMI and high KL grade have been identified as significant risk factors predictive for failure at mid-term follow-up.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The article processing charge for publication of this research was covered by Department of Surgical Sciences and Integrated Diagnostics (DISC) of the University of Genova. The author (s) received no financial support for the research and authorship.