
Abstract
Background:
Recently, the inverted V-shaped high tibial osteotomy (iVHTO) procedure fixed with a locking compression plate (LCP) has attracted notice as a useful surgical option for medial osteoarthritic knees with severe varus deformity. However, no studies have clarified how bone healing at the osteotomy site progresses after this surgery or when bone union is completed.
Purpose:
To clarify how bone healing at the osteotomy site progresses after the iVHTO procedure fixed with an LCP and when bone union is completed.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 109 knees in 96 patients who underwent this procedure were followed up for a minimum of 24 months after surgery. Radiographs were obtained at 5, 8, 12, 16, 20, 24, 36, 52, and 104 weeks after surgery. In addition, computed tomography (CT) imaging was performed at 5, 12, and 24 weeks. Three experienced surgeons independently observed the radiographs and CT images. The radiographic union score for tibial fractures was used to quantitatively determine the bone union time. The relationship between bone healing and clinical outcome measures was analyzed.
Results:
The progression of bone healing at the osteotomy site after this iVHTO procedure could be classified into 3 types: type 1 (direct bone healing), type 2 (indirect bone healing), and type 3 (delayed bone healing). The incidences of types 1, 2, and 3 were 75.2%, 18.3%, and 6.4%, respectively. The mean time required to complete bone union was 10.6 weeks in type 1 knees, 16.8 weeks in type 2 knees, and 22.3 weeks in type 3 knees, showing significant differences among the 3 types (P < .001). The mean overall bone union time was 12.5 weeks in 108 knees, excluding 1 knee that required additional surgery. The overall rate of major complications was 9.2%, which included only cases of delayed union. The complication rate was significantly different among the 3 types (P < .001).
Conclusion:
The fact that type 1 bone healing occurred in 75.2% of knees is a unique feature of iVHTO fixed with an LCP. Early completion of bone union with rare complications is one of the clinical advantages of this iVHTO procedure.
The inverted V-shaped (iV) high tibial osteotomy (HTO) procedure is defined as a hemi–lateral closing wedge (LCW) and hemi–medial opening wedge (MOW) HTO procedure with immediate bone grafting.1,14 In this procedure, the center of tibial alignment correction by the HTO is located approximately at the center of rotation of angulation 21 of the tibia. Therefore, the iVHTO is classified as a neutral wedge (NW) HTO, which has various theoretical advantages compared with LCWHTO and MOWHTO.15,21 The first iVHTO procedure, in which a Charnley external fixation device was used to fix the osteotomy site, was reported in 1986. 27 The minimum 10-year follow-up results of this procedure, which were reported by Aoki et al 1 in 2006, showed that the incidence of complications was significantly reduced compared with the knees that underwent LCWHTO. In this iVHTO procedure, however, it took 10 weeks or more before weightbearing on the operated limb began. To improve this disadvantage, we developed a modified iVHTO procedure fixed with a locking compression plate (LCP). 14 In 2022, Kondo et al 13 reported the midterm follow-up results of this procedure, showing that this procedure did not change the patellar height, posterior tibial slope (PTS), tibial length, or bone mass and shape of the proximal tibia, even after a large correction was made. Recently, the iVHTO procedure fixed with an LCP has attracted notice as a useful surgical option for medial osteoarthritic knees with severe varus deformity, 28 because various advantages compared with MOWHTO and LCWHTO have been demonstrated by clinical studies.9,13,33 However, no studies have clarified how bone healing at the osteotomy site progresses after the iVHTO procedure fixed with an LCP or when bone union is completed.
When evaluating the clinical usefulness of NWHTO procedures as well as LCWHTO procedures, the length of the postoperative period until bone union is complete is important. The longer the period, the more social or economic losses the patient experiences, because patients are restricted from returning to work or from participating in sports until the bone union is complete. In our preliminary study on the iVHTO fixed with an LCP, 36 complete bone union was achieved within 3 months after surgery in most knees that underwent this surgery. Therefore, this iVHTO procedure is likely to be the technique that results in early postoperative bone union. The present study was conducted to test this hypothesis. To do so, it was necessary to clarify not only the time of completion of bone union after this surgery but also the radiological healing process of the osteotomy site after surgery until the bone fusion was complete.
Therefore, we conducted the present study using a quantitative radiological method to clarify how bone healing at the osteotomy site progresses after the iVHTO procedure fixed with an LCP and when bone union is completed. We found the following. (1) The progression of bone healing at the osteotomy site after iVHTO fixed with an LCP could be classified into 3 types: type 1 (direct bone healing), type 2 (indirect bone healing), and type 3 (delayed bone HEALING). Types 1, 2, and 3 occurred in approximately 75%, 18%, and 6% of knees, respectively. (2) The mean time required to complete bone union was approximately 11 weeks in type 1, 17 weeks in type 2, and 22 weeks in type 3, showing significant differences among the 3 types.
Methods
Study Design
A prospective observational study was conducted using 129 knees in 114 patients who underwent iVHTO with an LCP (TriS Inverted-V Lateral HTO Plate; Olympus Terumo Biomaterials) (Figure 1) between April 2017 and March 2021 in our hospital. The following study protocol was approved by the ethics review board of our hospital, and informed consent was obtained from all individual participants.

Schema of the inverted V-shaped high tibial osteotomy (iVHTO) procedure fixed with a locking compression plate (LCP). (A) Osteotomy lines. (B) Preoperative planning for fixation with an LCP. (C) LCP developed for iVHTO. Holes 1 and 2 have a function to apply a compression force.
The indications for the iVHTO procedure included (1) a knee with persistent pain due to medial osteoarthritis that did not improve despite 3 months of nonoperative therapy, (2) a medial osteoarthritic knee that needed a valgus correction angle >10°, and (3) patients who wanted to return to active daily activities, sports, or labor. The contraindications involved (1) a loss of knee extension <10°, (2) a loss of knee flexion <120°, (3) a knee with a lateral meniscus injury requiring surgical treatment, (4) a knee with severe patellofemoral osteoarthritis, (5) a knee with cruciate and collateral ligament insufficiency, (5) a history of infection in the knee or the tibia, and (6) a history of severe trauma of the leg. There were no age restrictions.
Two senior orthopaedic surgeons (E.K. and K.Yasuda.) who were sufficiently trained concerning the procedure performed all operations using the previously reported procedure with an LCP.11,14 The same rehabilitation protocol was used for all the knees after surgery. To clarify characteristics of the patients, preoperative demographic data were precisely recorded. Anteroposterior (AP) and lateral radiographs were obtained preoperatively and at 5, 8, 12, 16, 20, 24, 36, 52, and 104 weeks after surgery. In addition, computed tomography (CT) images were also obtained at 5, 12, and 24 weeks after surgery. However, if bone union was confirmed at some point, subsequent CT imaging was not performed to eliminate radiation exposure. On the other hand, in cases with prolonged bone fusion, CT imaging was performed when needed, even after 16 weeks postoperatively. To report details of the HTO surgery performed in each patient, the pre- and postoperative lower limb alignment and patellar height were measured before and 1 year after surgery. To quantitatively assess the time required to complete bone union (the bone union time) at the osteotomy site, the radiographic union score for tibial fractures (RUST)16,35 was used. To clarify the relationship between bone healing at the osteotomy site and the clinical results, we collected baseline and follow-up outcomes, including demographic data; complications; the Japanese Orthopaedic Association (JOA) score, which is the standard knee function scale in Japan1,13,33; the Lysholm score 18 ; and the Knee injury and Osteoarthritis Outcome Score (KOOS). 25 The final follow-up evaluation was made ≥2 years after surgery.
Three experienced orthopaedic surgeons (J.O., D.S., T.K.), who were blinded to all clinical information, independently observed each set of radiographs and CT images to radiologically elucidate the progression of bone healing at the osteotomy site. To calculate intrarater consistency, 1 observer (T.K.) was asked to score the radiographs again 4 weeks after the initial assessment.
Inverted V-Shaped HTO Procedure
Details of the iVHTO procedure have been previously reported.11,14 First, the fibula was osteotomized at the center of the shaft, using the acute oblique osteotomy and ligation procedure.33,37 Then, to perform the tibial osteotomy, a 10-cm curved skin incision was made on the anterolateral aspect of the proximal tibia. The tibialis anterior muscle attachment was detached subperiosteally from the tibial cortex. A lateral wedge resection angle was determined for each knee so that the mechanical axis in the corrected limb passed through a point on the lateral tibial plateau, which was 65% lateral to the medial edge of the tibial joint surface. Under observation using a C-arm fluoroscope, a K-wire was inserted perpendicular to the anterior surface of the proximal tibia and into the apex of the V-shaped osteotomy. A Protractor-Installed Wire Insertion Guide (Olympus Terumo Biomaterials), in which the angle of the 2 sleeves could be matched to the angle of the planned bone resection, was attached to the apex K-wire. Using this guide, we inserted 2 pairs of K-wires from the lateral side of the tibia through these sleeves so that each inserted K-wire precisely reached the apex wire. The coronal ascending osteotomy parallel to the anterior surface of the tibial tubercle was made using a thin oscillating saw, leaving the proximal part of the tibial tubercle intact with a width of 10 mm. A lateral hemi-LCW bone resection was made along the 2 pairs of inserted K-wires, using a thin oscillating saw and a thin chisel. Next, the anteromedial periosteum and a part of the superficial medial collateral ligament were scraped from the tibia just along the medial osteotomy line. A Parallel Drill Guide (Olympus Terumo Biomaterials) was attached to the apex K-wire so that the guide was located on the medial osteotomy line. Multiple parallel holes were created in the tibia by inserting a 2 mm–diameter K-wire into parallel sleeves in this guide. Along these parallel holes, the hemi-MOW was carried out with a thin chisel. A valgus force was manually applied to the tibia so that the knee alignment was corrected with an incomplete fracture at the apex portion of the V-shaped osteotomy. Temporary fixation was performed using 2 other K-wires.
Fixation of the tibia was achieved using an LCP, which was installed at the lateral side, using the quantitative technique to achieve the correction angle as planned preoperatively. 11 First, a marker wire was precisely inserted into the proximal tibia at the preoperatively planned position of the most proximal locking screw. By inserting the first locking screw along this marker wire, the LCP was precisely installed on the proximal tibia at the planned position. Then, a compression screw was inserted into the distal tibia through a combination hole in the LCP (Figure 2A). This screw pulled the distal tibia toward the distal part of the LCP while applying proximal displacement and valgus rotation. Thus, the tibia was precisely fixed with the LCP at the planned correction angle. After 3 locking screws were inserted into the remaining 3 distal holes of the LCP, the inserted compression screw was pulled out and another locking screw was inserted into the same hole (Figure 2B). Into an opening space at the medial side of the tibia, morselized bone chips made from the wedged bone resected from the lateral tibia were implanted.

(A) A compression screw (CS) was inserted into the distal tibia through a combination hole in the locking compression plate (LCP). (B) After 3 locking screws (LSs) were inserted into the remaining 3 distal holes of the LCP, the inserted compression screw was pulled out and another LS was inserted into the same hole. The locking screw diameter is 5.5 mm.
The displaced ends of the osteotomized fibula were reduced to ensure as much contact as possible between the osteotomy surfaces, and they were securely ligated with a polyester thread, leaving some degree of displacement and angulation.33,37 After irrigation, the subcutaneous tissue and the skin were closed (Figure 3).

Images obtained in a representative case that underwent inverted V-shaped high tibial osteotomy fixed with a locking compression plate. (A) Preoperative images. (B1 and B2) One-week postoperative images. (C) Twelve-week postoperative images.
Postoperative Management
A previously reported rehabilitation protocol13,14 was used for all knees postoperatively. Quadriceps exercise with quadriceps setting and straight leg raising was allowed 1 day after surgery. Passive knee range of motion from 0° to 90° was allowed during the first 2 weeks, and active knee range of motion from 0° to 120° was encouraged thereafter. Partial weightbearing using a pair of crutches was allowed at 3 weeks, and full weightbearing was permitted at 5 weeks. After 5 weeks, however, bone resorption appeared on radiographs in 10 knees. Therefore, immobilization of the knee with a knee brace was performed in 2 of those knees (one of the 2 knees needed an additional surgery later), and limitation of walking distance and daily activity was indicated in the other 8 knees.
Radiological Evaluations
Radiological Observations of the Progression of Bone Healing
The radiological progression of bone healing at the osteotomy site in each knee was observed according to the guidelines suggested in our preliminary study. 36 On each radiographic image, obscuration of the osteotomy line, occurrence of a radiolucent lesion, callus formation bridging beyond the osteotomy site, and increasing radiopacity around the osteotomy line were observed. On the CT images, formation of trabecula-like bone columns penetrating the narrow bone gap between the osteotomy surfaces and callus formation bridging beyond the osteotomy site were carefully assessed.
Assessment of the Time Required to Complete Bone Union at the Osteotomy Site
To quantitatively determine the bone union time at the osteotomy site, we used the RUST, which has been commonly used to assess bone healing at the fracture site of the tibia.16,35 The scoring rules in this system are as follows:
-Bone healing of the tibial osteotomy site was assessed at each of the medial, lateral, anterior, and posterior cortices visible on AP or lateral radiographs.
-Each cortex was given a score: ➢1 point if an osteotomy line was clearly visible with no callus ➢2 points if there was callus formation but an osteotomy line was still visible ➢3 points if an osteotomy line was invisible or if the cortices were completely bridged by a maturated callus even though an osteotomy line was still visible
-The individual scores for the 4 parts of the cortex were summed (full mark, 12 points) to give a total score at each period.
In addition, the bone union between the closing wedge osteotomy surfaces inside the tibia was observed on CT images. To evaluate the bone union of these surfaces, we developed the RUST assessment system using CT images (RUST-CT). In this system, trabecula-like bone formation at the gap between the hemi-LCW osteotomy surfaces was evaluated with the following scoring rules:
-This gap was divided into 4 portions: anterocentral, posterocentral, anterolateral, and posterolateral.
-Each gap was given a score: ➢1 point if a gap was clearly visible with no trabecula-like bone formation ➢2 points if trabecula-like bone columns penetrating the gap were sparsely found on almost all CT slices ➢3 points if the trabecula-like bone columns penetrating the gap were abundantly observed on almost all CT slices
-The individual scores for the 4 portions were summed (full mark, 12 points) to give a total score at each period.
Bone healing statuses shown on radiographs and CT images obtained at the scheduled postoperative time were independently scored using the RUST and RUST-CT, respectively. Three experienced orthopaedic surgeons (T.K., D.S., and J.O.), who were blinded to all clinical information, acted as observers and independently scored each set of radiographs or CT images. In the present study, the time when the total score of either the RUST or RUST-CT reached the maximum score of 12 points was defined as the time of bone fusion at the osteotomy site of each patient. 29
Evaluation of Postoperative Knee Alignment and Patellar Height
In each patient, AP view radiographs of the knee and the whole lower limb were obtained in a standing position on the diseased limb. A lateral view radiograph was obtained at 30° of knee flexion in the nonloading condition. As for dimensional parameters of the tibia, the anatomic femorotibial angle (FTA), the anatomic medial-proximal tibial angle (MPTA), the hip-knee-ankle angle (HKA), the point at which the mechanical axis (weightbearing line) passed across the joint line (%MA), and the tibial length were measured on the AP radiographs. The tibial length was defined as the length of the line between the central point of the tibial plateau and the central point of the joint surface of the tibiotalar joint. In addition, the Caton-Deschamps index, 4 the PTS angle, and the Insall-Salvati ratio 10 were measured on the lateral radiograph of the knee, according to the following definitions.
Clinical Evaluations
Demographic data included sex, age, height, body weight, bone mass index, bone mineral density (BMD), and osteoarthritis grade. The BMD was measured with a dual-energy x-ray absorptiometry bone densitometer (Discovery A; Hologic Inc) and is presented as the rate of the young adult mean. On the AP radiograph of the knee, the radiological stage of osteoarthritis was assessed according to the Kellgren-Lawrence grading system. 12
If any complications occurred postoperatively, the details were always recorded in the electronic medical record. Nonunion was defined as an osteotomy site where bone union had not yet been completed at 9 months after surgery.17,24,26,29 In addition, an osteotomy site that required additional surgery due to the appearance of a large translucent zone was defined as nonunion, regardless of the postoperative time. No studies have quantitatively defined the status of delayed union after LCWHTO or NWHTO surgery. Therefore, in the present study, delayed union was defined as an osteotomy site where bone union had not yet been completed at 4 months after surgery in the quantitative evaluation of postoperative radiographs obtained over time. This definition was made based on the following clinical facts: (1) The general time of bone union for proximal tibial fractures depends on the type of fracture. The general union time is 3 to 4 months for stable fractures without displacement as well as for fractures in which initial displacement has been anatomically reduced and firmly fixed.2,5,34 LCWHTO and NWHTO are surgeries that artificially create a proximal tibial fracture. Therefore, LCWHTO and NWHTO procedures, which are recognized as useful in the modern era, must produce bone union as early as or earlier than those fractures. (2) Patients who undergo the NWHTO as well as the LCWHTO commonly want to return to labor or sports activities as soon as possible. The longer bone union is delayed after these surgeries, the more the patient experiences various social or economic losses. According to our clinical experience a patient is only willing to tolerate these losses due to delayed union for approximately 3 months. Therefore, for LCWHTO and NWHTO procedures to be considered useful in the modern era, bone union must be achieved within at least 4 months.
Statistical Analysis
All continuous data are presented as the mean with the standard deviation. The quadratic weighted kappa was used to assess inter- and intrarater reliabilities concerning the radiographic union score. To compare the groups, the Mann-Whitney U test and Kruskal-Wallis test were used for continuous variables, and the Pearson chi-square test was used for discrete variables. On the other hand, the effects of the HTO performed on patients were evaluated by comparing the preoperative data with the postoperative results, using the paired t test. Before the calculation, the Shapiro-Wilk test was performed to confirm that a parametric method was appropriate for this additional comparison. A commercially available software program (JMP Pro Version 10.0 for Windows; SAS Institute Japan) was used for statistical calculation. The significance level was set at a P value of .05.
Results
Preoperative Demographic Data of Patients and Knees
Among the 114 patients (129 knees) who underwent iVHTO, 18 patients (20 knees) were lost to follow-up before 2 years after surgery. Therefore, 109 knees of 96 patients were enrolled in the present study. These patients were followed up for ≥24 months after surgery. The demographic data is shown in Table 1. The mean age was 61.3 years, the mean body mass index was 25.2 kg/m2, and the mean BMD was 93.5%. Concerning osteoarthritis grade, grade 3 knees were present in 51.4% of all knees and grade 4 in 20.2% of knees. Two knees with grade 1 osteoarthritis had a painful posterior root tear of the medial meniscus and severe varus deformity, requiring meniscal suture and valgus correction of 16° with the iVHTO procedure.
Demographic Data of Patients and Knees a

Data are presented as n (%) or mean ± SD unless otherwise indicated. BMD, bone mineral density; BMI, body mass index; YAM, young adult mean.
Changes in Tibial and Patellar Alignment due to the HTO
The preoperative FTA, HKA, %MA, and MPTA values showed that all 109 knees had severe varus deformity. The mean intraoperative correction angle of the tibia was 12.8°. Postoperatively, the mean MPTA significantly increased to 93.5°, and the FTA, HKA, and %MA were sufficiently corrected to 170.1°, 3.9°, and 65.7%, respectively. The surgery did not significantly affect the PTS, Caton-Deschamps index, or Insall-Salvati ratio (Table 2).
Radiological Comparisons of Pre- and Postoperative Alignment and Patellar Location a
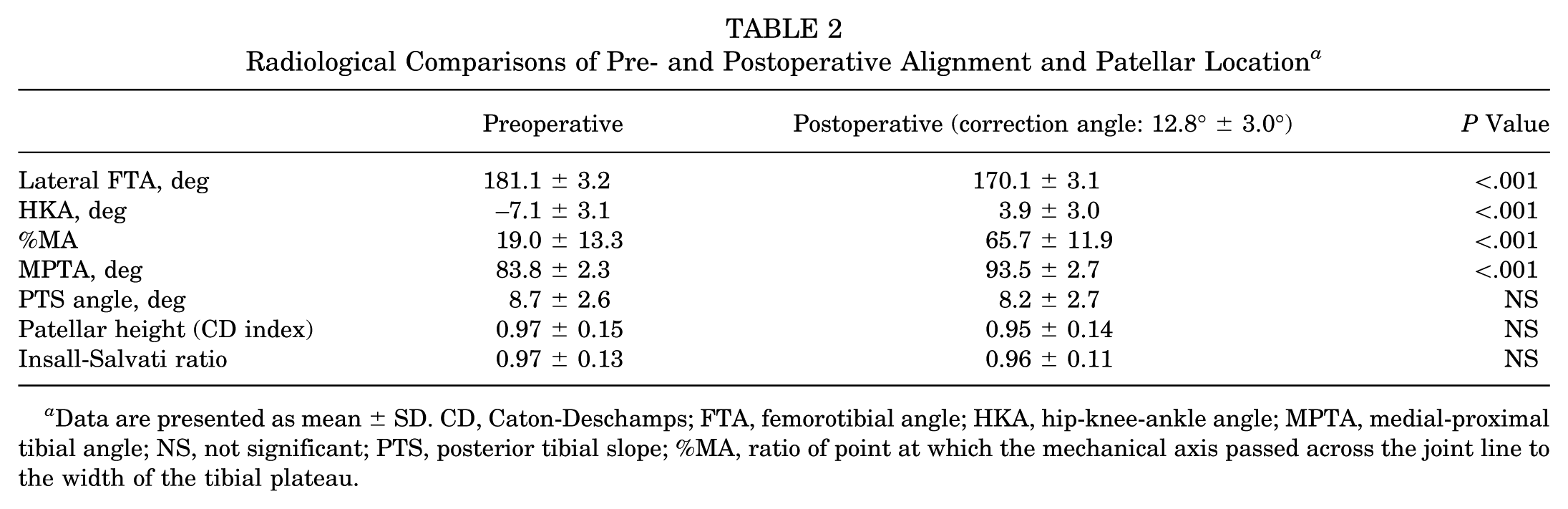
Data are presented as mean ± SD. CD, Caton-Deschamps; FTA, femorotibial angle; HKA, hip-knee-ankle angle; MPTA, medial-proximal tibial angle; NS, not significant; PTS, posterior tibial slope; %MA, ratio of point at which the mechanical axis passed across the joint line to the width of the tibial plateau.
Radiological Observations of the Progression of Bone Healing
In the AP radiograph obtained immediately after surgery, the osteotomy line in the lateral portion of the tibia was very thin or indistinct because the osteotomy surfaces were in close contact under a high compression force, while the medial hemi-MOW space was filled with grafted bone chips (Figures 3B, 4A, 5A, and 6A).
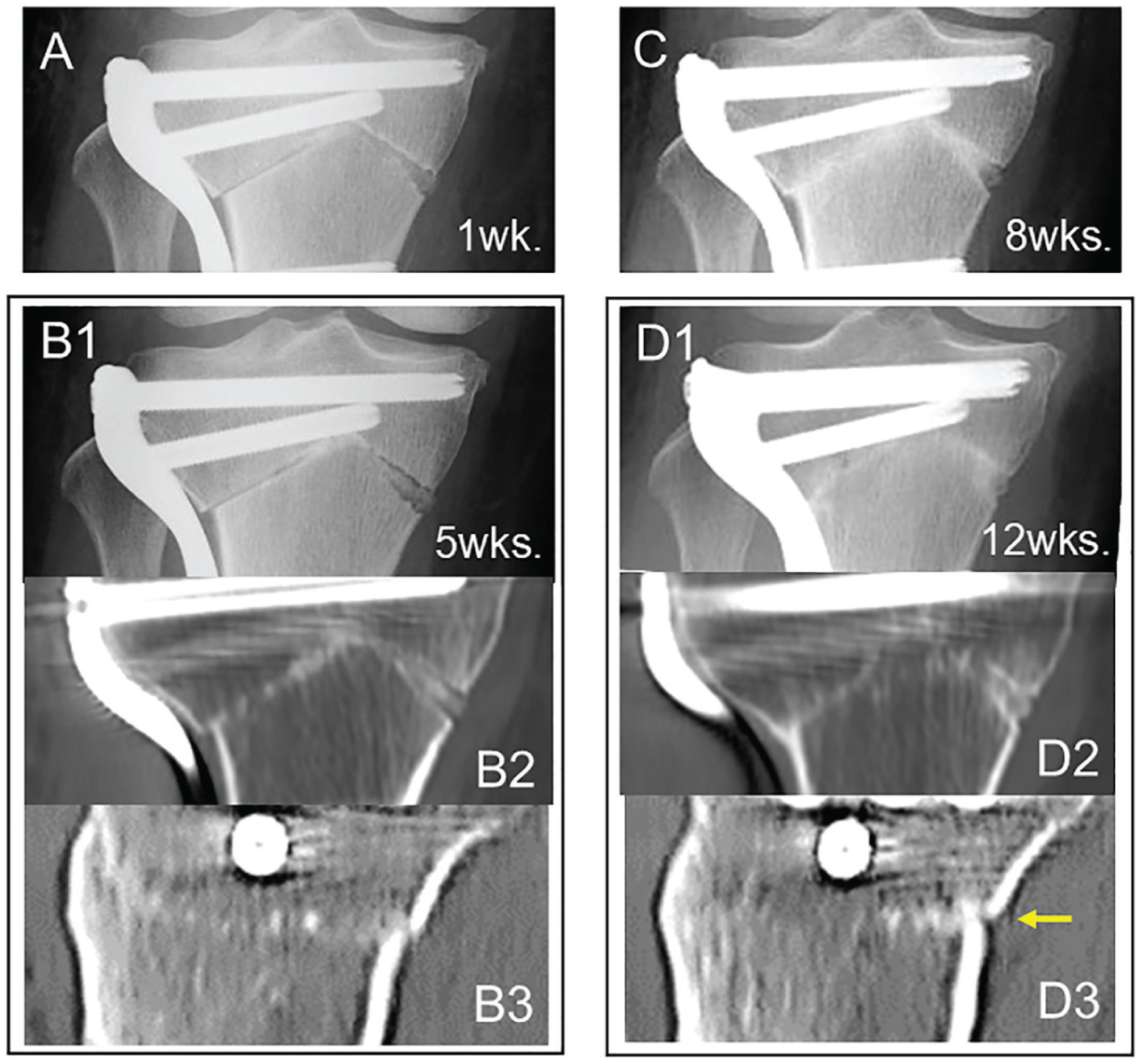
Type 1 healing. (A and B1) At 1 and 5 weeks, the lateral osteotomy line was indistinct in the radiographs. (B2 and B3) Computed tomography (CT) images obtained at 5 weeks indicated that trabecula-like bone columns penetrating the narrow bone gap were sparsely formed. (C and D1) In radiographs obtained at 8 and 12 weeks, radiopacity at the osteotomy line increased. (D2 and D3) CT images obtained at 12 weeks showed that the gap was fully filled with the trabecula-like bone columns. Note that bridging callus was not formed on the posterior cortex (yellow arrow).

Type 2 healing. (A and B) At 1 week, the lateral osteotomy line was indistinct in the radiographs. (C1) At 5 weeks, radiolucency of the medial opening space appeared to have increased in the radiograph, (C2 and C3 [CT]) but the lateral images show that a callus (yellow arrows) formed over the osteotomy line at the posterior cortex of the tibia. At 12 weeks, radiopacity at the osteotomy line further increased in the radiograph by an abundantly formed bridging callus (D1, D2, and D3 [CT]). CT, computed tomography.

Type 3 healing. (A1 and A2) At 1 week, the lateral osteotomy line was indistinct. At 5 weeks, radiolucency (yellow arrow) in the medial tibia increased (B1). (B2 and B3) In the computed tomography (CT) images, a small amount of extraosseous callus (blue arrow) was observed on the posterior cortex. (C1 and C2 [CT]) At 12 weeks, a wide osteolytic zone appeared, (C3 [CT]) while a large amount of callus was formed on the posterior cortex. (D1 and D2 [CT]) At 24 weeks, although the radiolucent zone still existed, (D3 [CT]) the abundantly formed bridging callus became sclerotic.
Progression of bone healing at the closing wedge osteotomy site could be radiologically classified into 3 types according to the criteria shown in Table 3.
Criteria to Classify Progression of Bone Healing After iVHTO Into 3 Types a

Postoperative observations were made using radiographs and computed tomography (CT) images.
In the knees showing type 1 healing, the osteotomy line was indistinct in the radiographs at 5 weeks (Figure 4B1), and the CT images indicated that trabecula-like bone columns penetrating the narrow bone gap were sparsely formed (Figure 4, B2 and B3). At 8 and 12 weeks, radiopacity at the osteotomy line increased in the radiographs (Figure 4, C and D1), and CT images obtained at 12 weeks showed that the bone gap was filled with the trabecula-like bone columns (Figure 4, D2 and D3). Thus, complete bone union in type 1 was achieved by the trabecula-like bone column formation penetrating the narrow bone gap, without extraosseous bridging callus formation (Figure 4D3).
In the knees showing type 2 healing, the osteotomy line was indistinct at 5 weeks, but radiolucency of the medial opening space, where bone chips had been densely packed, appeared to have increased in the radiographs (Figure 5C1). The CT images showed that a callus formed over the osteotomy line at the posterior cortex of the tibia (Figure 5, C2 and C3). At 8 to 16 weeks, radiopacity at the osteotomy line further increased in the AP radiograph (Figure 5D1) by an abundantly formed bridging callus (Figure 5, D2 and D3), although part of the medial opening space still appeared radiolucent.
In the knees showing type 3 healing, the osteotomy line became distinct and the radiolucency of the medial opening space, where bone chips had been densely packed, appeared to have increased in the radiographs at 5 weeks (Figure 6, B1 and B2). The CT images showed that the bridging callus was slightly formed on the posterior cortex (Figure 6B3). At 8 and 12 weeks, a wide radiolucent zone appeared in the radiographs (Figure 6C1), and the CT images showed that a wide osteolytic zone was found in the central-posterior portion of the tibia with extraosseous callus formation on the posterior cortex (Figure 6, C2 and C3). At 20 and 24 weeks, the radiographs and CT images showed that the abundantly formed bridging callus became sclerotic, although the radiolucent zone still existed (Figure 6, D1-D3).
Time of Completion of Bone Union Among the 3 Types
Concerning these scoring systems, the weighted kappa was 0.955 (95% CI, 0.953-0.974), indicating strong agreement. Interrater reliability was evaluated by comparing the scores of the 3 observers (T.K., D.S., and J.O.). The weighted kappa was 0.853 (95% CI, 0.821-0.884) between raters 1 and 2, 0.803 (95% CI, 0.753-0.851) between raters 2 and 3, and 0.775 (95% CI, 0.726-0.817) between raters 3 and 1, all indicating strong agreement. Based on these scoring systems, the bone union rate and the time of bone union were determined in each patient.
The occurrence rate was 75.2% for type 1, 18.3% for type 2, and 6.4% for type 3 (Table 4). In type 1 knees, the bone union time at the osteotomy site was determined by the RUST-CT, because the RUST-CT was higher than the RUST at each examination time. On the other hand, in type 2 and 3 knees, the bone union time was determined by the RUST, because the RUST was higher than the RUST-CT at each examination time. Bone union was achieved without any additional treatments in all knees classified as type 1 or 2. One knee in the type 3 knees was diagnosed with possible nonunion at 6 months and underwent an additional surgery (addition of medial plate fixation with autologous iliac bone grafting to the radiolucent lesion). So, the bone union rate in type 3 was 85.7%. There was statistical significance (P < .001) in the bone union rate among the 3 types. The mean overall bone union rate after this iVHTO procedure was 99.1% (108 in the 109 knees). The mean time required to complete bone union was 10.6 weeks in type 1 knees, 16.8 weeks in type 2 knees, and 22.3 weeks in 6 of the 7 knees (the nonunion knee was excluded) classified as type 3 (Table 4). There was a significant difference (P < .001) among the 3 types. In the 108 knees with no additional surgery, the mean bone union time was 12.4 ± 4.4 weeks. Additionally, in the 102 knees classified as types 1 and 2 (93.6% of the 108 knees), the mean bone union time was 11.0 ± 2.3 weeks.
Occurrence Rate of the 3 Types, and Comparisons of Bone Union Rate and Time of Bone Union Among the 3 Types

Time required to complete bone union.
Analysis of the Potential Factors Affecting Occurrence of the 3 Types
To analyze potential factors affecting the occurrence of type 3, the background and surgical factors and the dimensional factors reflecting the degree of correction by HTO surgery were compared among the 3 types (Table 5). However, there was no significant difference in each factor among the 3 types.
Comparisons of the Background and Surgical Factors Among the 3 Types a

Data are presented as n (%) or mean ± SD. BMD, bone mineral density; BMI, body mass index; FTA, femorotibial angle; HKA, hip-knee-ankle angle; %MA, ratio of point at which the mechanical axis passed across the joint line to the width of the tibial plateau; MPTA, medial-proximal tibial angle; YAM, young adult mean.
Comparisons of Postoperative Complications Among the 3 Types
In the 82 knees classified as type 1, there were 3 cases (3.7%) of minor complications, including incomplete peroneal nerve palsy and delayed wound healing, which healed within 3 weeks. In the 20 knees classified as type 2, there were 3 cases (15.0%) of delayed bone union. In all 7 knees classified as type 3, delayed union occurred (Table 6). There were significant differences (P < .001) in the complication rate among the 3 types. In 1 of the 10 knees diagnosed with delayed union, a medial plate fixation was added with iliac bone grafting at 3 months postoperatively, because the radiolucent zone was enlarged. In the remaining 9 knees with delayed union, 1 case was advised to wear a knee brace when walking, and the other 8 cases were instructed to decrease walking distance and activities of daily living. As a result, bone union was completed in these 6 knees 4 to 9 months after surgery. The overall rate of major complications was 9.2% (10/109 knees).
Comparisons of the Postoperative Complications Among the 3 Types a

Data are presented as n (%). NS, not significant.
Comparisons of Clinical Outcomes Among the 3 Types
Preoperatively, there were no significant differences in JOA score, Lysholm score, or KOOS among the knees of the 3 types. In the 2-year follow-up evaluations, all scores were significantly improved in each type (P < .001), while 1 knee of type 3 in need of additional surgery was excluded from the postoperative evaluation. In the 2-year clinical outcomes, there were no significant differences in these 3 scores among the 3 types (Table 7).
Comparisons of the JOA Score, Lysholm Score, and KOOS Subscores Among the 3 Types a

Data are presented as mean ± SD. The P values show the results of comparing each item among the 3 Types. Additionally, the effect of inverted V-shaped high tibial osteotomy on each item was evaluated by comparing the pre- and postoperative data (significant P values [P < .001] of this comparison are denoted with an asterisk). JOA, Japanese Orthopaedic Association; KOOS, Knee injury and Osteoarthritis Outcome Score.
Discussion
The first important finding in the present study is that the progression of bone healing at the osteotomy site after iVHTO fixed with an LCP could be classified into 3 types. Type 1 is characterized by early completion of the bone union via direct healing, in which the trabecula-like bone columns penetrating the narrow gap between the osteotomy surfaces were formed without extraosseous bridging callus formation. A characteristic of type 2 is that the bone union is completed via direct healing, in which the extraosseous bridging callus was formed beyond the osteotomy site. Type 3 is characterized by a large radiolucent zone that appears at the osteotomy site at 5 weeks postoperatively. The incidences of types 1, 2, and 3 were 75.2%, 18.3%, and 6.4%, respectively.
The second important finding in the present study is that the mean time required to complete bone union was 10.6 weeks in type 1 knees, 16.8 weeks in type 2 knees, and 22.3 weeks in type 3 knees, showing significant differences among the 3 types. In the 108 knees with no additional surgery, the mean bone union time was 12.5 weeks. Furthermore, in the 102 knees classified as types 1 and 2 (93.6% of all 109 knees), the mean bone union time was 11.0 weeks. In addition, the complication rate was 3.7% in type 1, 15.0% in type 2, and 100.0% in type 3, showing significant differences (P < .001) among the 3 types.
Concerning the first important finding, we considered the nature of the 3 types of bone healing progression at the osteotomy site, which occurred after iVHTO fixed with an LCP. It is well known that both direct healing and indirect healing occur in the bone healing mechanism.8,19 Direct healing occurs without extraosseous callus formation, when the space between bone contact surfaces is <1000 µm and micromotion of the contact surfaces is completely suppressed by a rigid internal fixation. On the other hand, indirect healing occurs with extraosseous bridging callus formation, when the micromotion of the contact surfaces is not completely suppressed by internal or external fixation.8,19 The radiological findings shown in the present study suggest that direct bone healing occurred in the knees classified as type 1, because bone union was completed within 12 weeks with the trabecula-like bone column formation penetrating the narrow gap and without bridging callus formation. Indirect bone healing occurred in the knees classified as type 2, because bone union was obtained with extraosseous bridging callus formation. The type 3 findings indicate that delayed union occurred in these knees. Here, it should be noted that type 1 bone healing occurred in 75.2% of all knees. This is a remarkable feature of the iVHTO using LCP fixation, because no studies have reported that direct bone healing occurred after HTO surgery. According to our experience with LCWHTO,1,38 indirect bone healing almost always occurred after surgery.
Regarding the second important finding, the time required to complete bone union has not been quantitatively evaluated in previous studies on LCWHTO procedures. However, patients who undergo LCWHTO as well as iVHTO commonly want to return to labor or sports activities as soon as possible. Therefore, it should be recognized that the longer bone healing is delayed after these surgeries, the more the patient experiences various social or economic losses. Thus, the bone union time is important for evaluating the clinical value of these HTO procedures. Furthermore, delayed union should be recognized as a major complication after these HTO surgeries. In the present study, the RUST system was used to judge the completion of bone union at the osteotomy site. The RUST system was developed by Whelan et al 35 in 2010 to standardize the evaluation of tibial fracture healing and was slightly modified by Leow et al 16 in 2016. The RUST system has been recognized as the most reliable and repeatable outcome measure to evaluate radiographic union of tibial fractures, and this system is frequently applied to fractures of other bones. 6
We searched the PubMed database for previous papers in which the bone union time after various LCWHTO procedures was described, to compare with the results of our study. Only 1 paper was found. Takahara et al 31 reported that the mean bone union time after the improved LCWHTO procedure was 4.5 months in 44 knees (80% of 55 knees), while it was >6 months in 11 knees (20% of the 55 knees). The mean bone union time in all 55 knees was calculated to be >4.8 months. This result cannot be simply compared to that of our study because the inclusion and exclusion criteria, the background factors of the patients, and the postoperative management are not the same between the 2 studies. However, we believe that the mean bone union time reported in the present study (overall bone union time, 12.5 weeks) can be a target value to be surpassed in future clinical studies to improve LCWHTO and iVHTO procedures. On the other hand, it is well known that the course of bone healing after MOWHTO is extremely different from that after iVHTO and LCWHTO, because healing after MOWHTO proceeds by the formation of new bone tissue in the vacant space. Therefore, there is little clinical utility in comparing the bone healing course after MOWHTO procedures to that after other procedures.
In the present study, delayed union after HTO was quantitatively defined as the bone healing status at the osteotomy site where bone union had not yet been completed at 4 months after surgery. The reasons for this definition are given in the Methods section. This definition is reasonable given that open reduction and internal fixation procedures for proximal tibial fractures are aimed at completion of bone union at 3 to 4 months postoperatively.2,5,34 Inverted V-shaped HTO and LCWHTO are procedures to create an artificial fracture in the proximal tibia. Therefore, osteotomies and internal fixations that favor bone union over accidental fractures must be performed. Thus, iVHTO and LCWHTO procedures that fail to achieve bony fusion 3 to 4 months postoperatively will not be highly regarded by patients who wish to return to work or high activity. In the present study, the overall occurrence rate of delayed union was 9.2% (10/109 knees). We searched for previous papers describing the occurrence rate of delayed union after various LCWHTO procedures to compare with our results but found none.3,20,30,32 According to our previous experience, 38 delayed union is common after LCWHTO. Further studies are required to clarify the occurrence rate of delayed union after LCWHTO. In the present study, there were no significant differences in clinical and functional outcomes among the 3 types. However, these clinical evaluations were performed postoperatively at 2 years, when most of the patients had returned to their desired labor or sports activities. Therefore, these evaluations may not reflect the dissatisfaction and social or economic loss of the patients during the period when bone union was not complete. In this study, 9 knees were diagnosed with delayed union but healed without additional surgery. Of these 9 cases, 1 case was advised to wear a knee brace when walking, and the other 8 cases were instructed to decrease walking distance and activities of daily living. These nonoperative treatments lasted from 2 to 4 months after the delayed union was suspected to occur in these knees. During such periods, the patients experienced social or economic disadvantages, because they were unable to return to work or health and sports activities. If patient-reported outcome assessments were performed during such periods, those patients might have rated the surgical treatment significantly lower. In the present study, the occurrence rate of delayed union was 9.2%. We are not satisfied with this result. Further studies are needed to eliminate the occurrence of delayed union.
This study is the first to report that early bone union via the direct healing mechanism occurs dominantly in the iVHTO procedure fixed with LCP. This suggests that this procedure has some technical and biomechanical advantages. First, since the size of the resected bone wedge in the iVHTO is about a quarter of that of the LCWHTO, it is easier to make full contact between the osteotomy surface with the iVHTO. This is supported by the fact that the osteotomy line was indistinct on the radiographs obtained immediately after surgery in almost all knees. Second, the osteotomy site with a concave-convex structure in the iVHTO, which is fixed with an LCP applying a high compression force, is stable against shear and rotational forces. 14 Third, the LCP developed for the iVHTO conforms to the outer shape of the tibia and allows for the insertion of 4 long locking screws each in the proximal and distal parts of the tibia, thus reducing micromotion at the osteotomy site. 11 Therefore, these biological and biomechanical environments might meet the necessary conditions for indirect healing to occur.
In the present study, however, knees classified as type 2 (indirect bone healing) and type 3 (delayed union) were found in 18.3% and 6.4%, respectively, even though the radiological findings of these knees were not different from those of type 1 knees immediately after surgery. We considered why types 2 and 3 occurred postoperatively, even though the findings in the radiographs obtained immediately after surgery were similar among types 1 to 3. It is well known that indirect bone healing occurs in operative treatments in which some micromotion occurs at the fracture site.22,23 In addition, too much micromotion and/or load results in delayed healing or nonunion. 7 Based on these facts, we considered that full weightbearing allowed at 5 weeks might increase micromotion at the osteotomy site to a greater degree in knees classified as types 2 and 3 than in the knees classified as type 1. Furthermore, the degree of micromotion at the osteotomy site in the knees classified as type 3 might be greater than that in the knees classified as type 2, and it might exceed a level that would induce a delayed union. Clinically, the occurrence of type 2 may be acceptable, but the emergence of type 3 should be completely prevented in the future.
To determine if there were specific clinical features of the type 3 group that significantly differed in incidence from the other groups, we compared the background clinical factors among the 3 types. The detection of such features would encourage future studies to determine the cause of the occurrence of type 3. However, the statistical analyses could not show any specific features of the type 3 group. In particular, although female knees comprised 6 of the 7 knees classified as type 3, there was no significant difference in the sex even between groups 1 and 3. In addition, neither the amount of correction nor the postoperative alignment was a causative factor. However, it should be recognized that the number of knees in the type 3 group was very small. This fact might have a significant impact on the statistical analyses. Therefore, we could not draw a definitive conclusion regarding this analysis.
It is likely that various mechanical factors combine to affect the occurrence of type 3, according to our clinical experience. The biomechanical properties of the tibia-LCP complex should differ among the patients, depending on the biomechanical properties of the cortical and cancellous bones of the tibia, the length of the screws, the location of the LCP, and so on. Therefore, it is possible that the fixation of the osteotomy site in knees classified as type 3 was more mechanically unstable than in those classified as type 2. Furthermore, to these mechanically vulnerable knees, a combination of some clinical factors, such as increased body weight and enhanced physical activities, might additionally yield adverse effects, resulting in the occurrence of type 3. However, it is impossible to quantify these mechanical factors in clinical studies. To verify this hypothesis, biomechanical studies using cadaveric knees should be conducted in the future.
It is clinically useful to radiologically diagnose which type of bone healing is occurring in patients who are in the rehabilitation phase after iVHTO, because the orthopaedic surgeon can predict the subsequent healing course of the osteotomy site and instruct each patient to return to sports or labor activities at the proper time. In addition, this prediction is important to optimize the late phase rehabilitation for each patient. For example, when the orthopaedic surgeon detects the occurrence of type 3 healing, the surgeon should change the planned rehabilitation protocol and apply some nonoperative measures in the patient's care. Such management can avoid additional surgery. However, the most essential solution to the problems associated with type 3 is to eliminate the occurrence of type 3 healing. To achieve this, patient selection is important. At present, the cause of type 3 healing is unknown. In the present study, however, we did not explore physiological factors that influenced the development of type 3 healing. For example, if preoperative examinations on vitamin D level, bone metabolism markers, and endocrine status are performed in a future study, physiological factors associated with the development of type 3 healing could be detected. Advances in such studies would optimize preoperative patient selection. On the other hand, from the perspective of advancing surgical technology, it is also important to devise or develop useful devices that have sufficient fixation strength even for fragile bones.
Recently, Kondo et al 13 reported the following clinical advantages of the iVHTO procedure with an LCP: (1) it does not induce patella baja or alta, (2) it does not change the tibial length, (3) it rarely induces postoperative complications, and (4) it does not alter the amount of bone in the proximal tibia and the shape changes are minimal, resulting in easy implementation of potential total knee arthroplasty in the future. The present study has added the following advantages of the iVHTO procedure with an LCP: (5) the time of complete bone union is very early (mean, 12.5 weeks in all knees; mean, 11.0 weeks in knees without delayed union) compared with other HTO procedures. However, this procedure has the following disadvantages, which are common in all LCWHTO procedures: (1) it needs an additional osteotomy to shorten the fibula, (2) it is technically difficult compared with MOWHTO, (3) and the start of weightbearing is somewhat later than that after MOWHTO.
The present study has some limitations. First, 18 patients (20 knees) of 114 patients (129 knees) who underwent iVHTO were lost to follow-up. The exact impact of the loss to follow-up of these patients on the analysis of this study is unknown. Second, the number included in this study, 109 knees in 96 patients, may be insufficient to draw absolute conclusions. Third, the 2-year follow-up period is not long enough to observe the effect of the large correction on the clinical outcomes, although it is long enough to observe the effect on bone healing. Fourth, there were no histological evaluations to support the radiological findings for the classification of bone healing progression. Fifth, this study dealt only with knees that underwent the iVHTO procedure fixed using an LCP. Therefore, we could not discuss the superiority or inferiority of this procedure compared with other procedures. Sixth, we did not examine physiological factors that might affect healing after osteotomy before surgery. Therefore, the cause of type 3 healing was not explored in the present study. Despite these limitations, however, this study provides important information on the iVHTO procedure to the clinical field regarding HTO.
Conclusion
The present study demonstrated that (1) the progression of bone healing at the osteotomy site after this iVHTO procedure could be classified into 3 types, type 1 (direct bone healing), type 2 (indirect bone healing), and type 3 (delayed bone healing); and (2) type 1 accounted for 75.2% of all 109 knees, and the mean time required to complete bone union was 10.6 weeks postoperatively, without any major complications. The mean overall bone union time was 12.5 weeks, and the rate of major complications was 9.2%, which included only cases of delayed union. The fact that type 1 bone healing occurred in 75.2% of knees is a unique feature of iVHTO fixed with an LCP. Early completion of bone union with rare complications is one of the clinical advantages of this iVHTO procedure.
Footnotes
Acknowledgements
The authors thank the staff of the Radiography Division, Yagi Orthopaedic Hospital, for their professional support in performing the MRI examinations. The authors appreciate Howard Tarnoff, professor emeritus of Health Sciences University of Hokkaido, for proofreading the English draft.
Final revision submitted April 16, 2025; accepted May 29, 2025.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the ethics review board of Yagi Orthopaedic Hospital.