
Abstract
Background:
An alternative single-bundle anatomic anterior cruciate ligament (ACL) reconstruction (ACL-R) devised by the senior author comprised an anterolateral reinforcement using an iliotibial band (ITB) autograft. The knee biomechanics of this technique have not been compared with standard ACL-R methods.
Purpose:
To compare the knee kinematics of ACL-R using bone–patellar–tendon bone graft with lateral extra-articular tenodesis (BTB+LET) versus ITB ACL-R with anterolateral reinforcement.
Study Design:
Controlled laboratory study.
Methods:
A total of 20 unpaired fresh-frozen human cadaveric knees (mean age, 41.4 years) were tested using a robotic system under 3 loads: (1) 89-N anterior tibial (AT) load (at 0°-90° of flexion); (2) 5-Nm internal rotation (IR) tibial torque (0°-90° of flexion); and (3) a simulated pivot-shift (PS) load, as a combined 7-Nm valgus moment and 5-Nm IR torque (at 0°, 15°, and 30° of flexion). All knees were tested with the ACL intact; one ACL-R group (n = 10) was tested with ITB reconstruction, and the other group (n = 10) was tested with BTB graft reconstruction, both with (BTB+LET) and without a LET procedure.
Results:
Significantly less AT translation, IR, and tibial displacement during simulated PS were detected at all knee flexion angles in the ITB, BTB, and BTB+LET states compared with the ACL-deficient state (P < .05). There was no statistically significant difference during AT loading, IR torque, and simulated PS between BTB and ITB states at all knee flexion angles (P .05). In response to AT loading, significantly less translation was detected in the BTB+LET state compared with the ITB state at 15° (mean difference [MD], 1.6 ± 0.7 mm; P = .048), 30° (MD, 1.8 ± 0.7 mm; P = .03), and 60° (MD, 1.5 ± 0.6 mm; P = .03) of knee flexion. In response to IR torque, the only statistically significant difference between ITB and intact state was at 0° of knee flexion. In response to simulated PS, significantly less tibial displacement was detected in the BTB+LET state compared with the intact state at 15° (MD, 1.7 ± 0.5 mm; P = .04) of knee flexion.
Conclusion:
BTB and ITB ACL-R both improved knee stability compared with the ACL-deficient state in response to AT, IR, and simulated PS loading; however, no method restored the intact ACL behavior. BTB+LET caused overconstraint at 15° of knee flexion during simulated PS loading.
Clinical Relevance:
ITB ACL-R provides an alternative technique to improve stability of the ACL-deficient knee.
The incidence of anterior cruciate ligament (ACL) injury is increasing in physically active adolescents. 41 While delayed or nonoperative treatments have historically been preferred for this age group, surgical management has increased in recent years.28,41 However, ACL reconstruction (ACL-R) failures in this group are significantly higher than in adults.4,9
Graft choice for adolescent ACL-R has a direct effect on the success of the surgery, with allograft ACL-R failing 3.8 times more often than autograft. 6 Hamstring tendon, bone–patellar tendon–bone (BTB), and quadriceps tendon are the most commonly used autografts in this age group, with hamstring tendon autograft demonstrating the highest risk for graft failure.9,18,26,33 Additionally, BTB autografts can lead to donor-site morbidities such as anterior knee pain and patellar fracture, while quadriceps tendon autograft has been shown to decrease knee extensor strength.7,20 Interestingly, the use of iliotibial band (ITB) autograft has resulted in comparable functional outcomes and failure rates to BTB autograft, while achieving faster postoperative knee extensor mechanism recovery than BTB, quadriceps tendon, and hamstring tendon autografts.39,44
Adolescent patients are at increased risk of ACL-R failure, and therefore lateral extra-articular tenodesis (LET) procedures have been recommended in this age group to reduce the risk of rerupture. 15 Biomechanical studies have demonstrated that LET and anterolateral ligament reconstruction reduce residual laxity to a similar degree during ACL-R.10,14 However, these procedures may cause overconstraint of the knee.14,45 A technique combining ACL-R with a lateral extra-articular procedure using ITB autograft for skeletally immature patients has previously been described, with a reported failure rate of 6% at 5-year follow-up. 24 This technique was shown to reduce tibial translation and rotatory knee instability to the same degree as the all-epiphyseal ACL-R and over-the-top techniques. 22 The proposed anatomic ACL-R with ITB autograft avoids the need to drill additional tunnels for the anterolateral reinforcement by using the same femoral tunnel as the anatomic ACL-R.
The aim of this study is to compare the kinematic effects of isolated ACL-R using BTB with (BTB+LET) and without LET to the ITB autograft anterolateral reinforcement ACL-R. It was hypothesized that the extra-articular reinforcement provided by the BTB+LET and ITB autograft anterolateral reinforcement ACL-R would similarly reduce anterior and rotational knee laxity compared to ACL-R with/without LET.
Methods
Institutional review board approval was obtained at the University of Pittsburgh for the use of cadaveric knee specimens. Twenty unpaired fresh-frozen human cadaveric knee specimens were tested (3 female and 17 male; mean age, 41.4 years (range, 23-62 years). Each specimen was kept frozen at −20°C and thawed at room temperature for ≥24 hours before testing. Prior to testing, each knee was assessed physically for stability and arthroscopically evaluated to ensure that all intra-articular structures were intact and that any osteoarthritis was not a grade >2 on the Outerbridge scale. For the knees in the ITB group, the ITB was identified and surgically harvested while keeping the tibial insertion intact. Then, for all knees, soft tissues 15 cm proximal and distal to the knee joint were removed before potting the femur and tibia in cylindrical molds with an epoxy compound for fixation in custom clamps for robotic testing.
Knees in the BTB ACL-R group were tested in 4 different states in the following order: (1) intact, (2) ACL-deficient, (3) ACL-R with a BTB graft (BTB), and (4) BTB ACL-R with LET (BTB+LET). Each knee in the ITB ACL-R group was tested in 3 states: (1) intact knee, (2) ACL- deficient, and (3) skeletally mature ACL-R technique using reinforcement with ITB (ITB) (Figure 1). Within each of the 2 groups, the knee kinematics of the different states were compared within each specimen. Between the 2 groups, knee kinematics were compared for the BTB alone, BTB+LET, and ITB knee states.

Illustration of anterior cruciate ligament reconstruction technique in skeletally mature knee using reinforcement with iliotibial band autograft.
Robotic Testing
All knee specimens were tested using a robotic testing system (CASPAR Stäubli RX90; Orto Maquet), with a robotic arm with ±0.02 mm of motion repeatability at each joint and an end effector with a universal force-moment sensor (Model 4015; JR3) with a force and moment accuracy of ±0.2 N and ±0.1 Nm, respectively, as per the manufacturer.8,27,46 The tibia and femur of each specimen were placed in custom cylinder fixtures, with the tibia connected to the robotic end effector and the femoral fixture secured to a fixed base. A cartesian coordinate system was used by the robotic testing system, with defined axes in the anteroposterior, mediolateral, and proximodistal directions of the tibia as described by Fujie.13,40 Data acquisition was performed using a custom MATLAB program (MathWorks) to perform the controlled motion and measure the force-moments in all 6 degrees of freedom. The robotic system determined the passive path of knee flexion of the cadaveric knee by minimizing forces (<0.5 N) and moments (<0.25 Nm) in all remaining degrees of freedom from full extension to 90° in increments of 0.5°.42,43
All specimens were tested under 3 loading conditions: (1) an 89-N anterior tibial (AT) load (simulated KT-1000 arthrometer test) to assess AT translation (ATT),11,21 (2) a 5.0-Nm internal rotation (IR) tibial torque, and (3) a 7.0-Nm valgus moment followed by a 5.0-Nm IR tibial torque (simulated pivot-shift [PS] test). 30 ATT and IR were measured at 0°, 15°, 30°, 45°, 60°, and 90° of knee flexion, while the simulated PS load was evaluated at 0°, 15°, and 30° of flexion.
Surgical Procedures
All surgeries were performed by the same fellowship-trained sports medicine surgeon (E.A.O.) with >5 years of experience.
BTB ACL-R Group
Standard arthroscopic anterolateral and anteromedial portals were created, and anatomic single-bundle ACL-R was performed.8,27,36,46 The ACL was transected using a punch and motorized shaver. The femoral tunnel for ACL-R was drilled in the center of the femoral ACL footprint using a 10-mm cannulated femoral drill (Acufex; Smith & Nephew) via the transportal technique. A tibial aiming guide (Acufex; Smith & Nephew) set to 55° was then used to drill the tibial tunnel in the center of the tibial footprint. A 10 mm–diameter BTB autograft was harvested from each cadaveric specimen. 36 The cancellous bone end of the graft was positioned in the shallow aspect of the femoral tunnel, and the patellar tendon side of the graft was positioned in the deep aspect of the femoral tunnel. 3 The autograft was fixed using a 9 × 20–mm bioabsorbable screws (Biosure; Smith & Nephew) on the femur and tibia. Tibial fixation was performed at 20° of knee flexion and tensioned at 80 N using a tension meter (Meira Corp).3,8,29
The LET was performed using the modified Lemaire technique previously described in the literature. 38 An oblique 5-cm lateral skin incision was created from just behind the lateral epicondyle to the Gerdy tubercule. An ITB autograft (1 cm wide and 8 cm long) was harvested 1 cm anterior to the posterior border of the ITB, with the distal end left attached to the Gerdy tubercle. The ITB graft was sutured to be tubularized from its proximal end using a No. 2 nonabsorbable suture (Ultrabraid; Smith & Nephew) and then passed deep to the lateral collateral ligament (LCL). The femoral attachment site was positioned 5 mm posterior to the lateral epicondyle. 45 The femoral tunnel of the LET was drilled using a 6-mm cannulated femoral reamer aiming 20° proximal and anterior. 14 The LET graft was tensioned at 20 N using a tension meter, fixed at 70° of knee flexion, and at neutral rotation of the tibia with a bioabsorbable screw (7 × 25 mm).19,45
ITB ACL-R Group
Standard arthroscopic anterolateral and anteromedial portals were created and the ACL was resected using a punch and motorized shaver. Based on the insertion site of the native ACL, the femoral tunnel entry site was determined intra-articularly. An oblique 5-cm lateral skin incision was created from just behind the lateral epicondyle to the Gerdy tubercule. The ITB's anterior and posterior borders were identified, and the proximal ITB was removed ≥15 cm via Metzenbaum scissors (Aesculap) advanced under the skin from the lateral epicondyle along the ITB direction, leaving 2 mm at each border of the ITB.24,32 ITB harvesting was continued from the distal end of the lateral epicondyle to the lateral femoral condylar joint line, leaving the ITB distal insertion and joint capsule intact. The ITB graft was sutured to be tubularized at a length of 4 cm from its proximal end, and the graft diameter was measured as either 7.5, 8, or 9 mm depending on the size of the tissue. The lateral femoral condyle and LCL were then identified. The femoral tunnel extra-articular entry point was positioned 5 mm posterior to the lateral epicondyle, similar to the LET femoral tunnel in the study group. 45 The femoral tunnel retrograde drilling technique aiming guide (ACUFEX TRUNAV; Smith & Nephew) was inserted from the lateral portal and placed at predetermined intra- and extra-articular points. The femoral tunnel was created in an antegrade manner using a femoral drill that was sized the same as the predetermined graft sizes over the 2.4-mm guide wire via femoral aiming guide. An appropriately sized tibial tunnel was drilled using a tibial aiming guide set to 55°. The graft was passed over the LCL and through the femoral and tibial tunnels. A lateral reinforcement procedure was performed with the knee flexed to 80° during neutral rotation, and a bioabsorbable screw 1 mm thicker than the graft and 25 mm in length (Biosure) was inserted inward from the outside of the femoral tunnel while applying 80 N tension to the graft using a ligament tension meter. The ACL graft was then tensioned to 80 N using a ligament tension meter while the knee was at 20° of knee flexion during neutral rotation, and a bioabsorbable screw 1 mm thicker than the graft and 25 mm in length (Biosure) was inserted (Figure 1).3,8,29
Statistical Analysis
The specimens were divided into 2 age-matched groups. The data were analyzed using 1-way analysis of variance (SPSS Version 26.0; IBM Corp) with knee state as a factor to assess if there was a difference; that was followed by paired t tests with a Bonferroni correction. For within ACL reconstruction group comparisons, a repeated-measures analysis was used. Normality was verified in the statistical analysis. Statistical significance was set at P < .05 prior to the Bonferroni correction. The given P values have been scaled so that with the Bonferroni correction, significance still occurred with P < .05. The primary variable in this study was knee rotation under simulated PS loading. To determine the number of test samples, previous studies1,23 were considered and an a priori power analysis was performed (G*Power 3.1.9.2; Heinrich Heine University) 12 using a 2-tailed, paired t test and a significance level of.05, a power of 0.80, and a hypothesized effect size of d = 1.0, 34 which resulted in n = 10 samples. All data are given as the mean and standard deviation.
Results
There was no statistically significant difference in ATT between the BTB and BTB+LET states at any knee flexion angle (P > .05) (Figure 2). A significantly higher ATT was detected at 0°, 15°, 30°, 45°, and 60° of knee flexion in the BTB and BTB+LET states compared with the intact state (P < .05). A significantly higher ATT between the ITB state and the intact state occurred at all flexion angles (P < .05) (Figure 3). There was no statistically significant difference during AT loading between BTB and ITB states at any knee flexion angles (P > .05) (Figure 4). However, there was significantly less ATT in the BTB+LET state compared with the ITB state at 15° (mean difference [MD], 1.6 ± 0.7 mm; P = .048), 30° (MD, 1.8 ± 0.7 mm; P = .03), and 60° (MD, 1.5 ± 0.6 mm; P = .03) of knee flexion.

Anterior tibial translation (ATT) under 89-N anterior tibial loading for bone–patellar tendon–bone (BTB) anterior cruciate ligament reconstruction (*P < .05 vs intact; +P < .05 vs DEF). DEF, deficient; LET, lateral extra-articular tenodesis.

Anterior tibial translation (ATT) under 89-N anterior tibial loading for iliotibial band (ITB) anterior cruciate ligament reconstruction (*P < .05 vs intact; +P < .05 vs DEF). DEF, deficient.

Anterior tibial translation (ATT) under 89-N anterior tibial loading for bone–patellar tendon–bone (BTB) and iliotibial band (ITB) anterior cruciate ligament reconstruction (#P < .05 ITB vs BTB+LET). LET, lateral extra-articular tenodesis.
Under an IR torque, there was a significantly higher IR with BTB compared with the intact ACL at 0° (P < .001) and 15° (P = .006) of knee flexion (Figure 5). There was no statistically significant difference in IR between the BTB+LET and intact state at any flexion angle; however, adding LET to ACL-R reduced IR at 15° and 30° of flexion compared with BTB ACL-R alone. There was a statistically significant difference in IR between the intact ACL and the ITB states only at 0° of knee flexion (P = .005) (Figure 6). Further, there was no statistically significant difference between the BTB and ITB states at any knee flexion angle under the IR torque (Figure 7). There was significantly less IR in the BTB+LET state compared with the ITB state at 15° (MD, 4.1°± 1.4°; P = .01) of knee flexion (Figure 7).
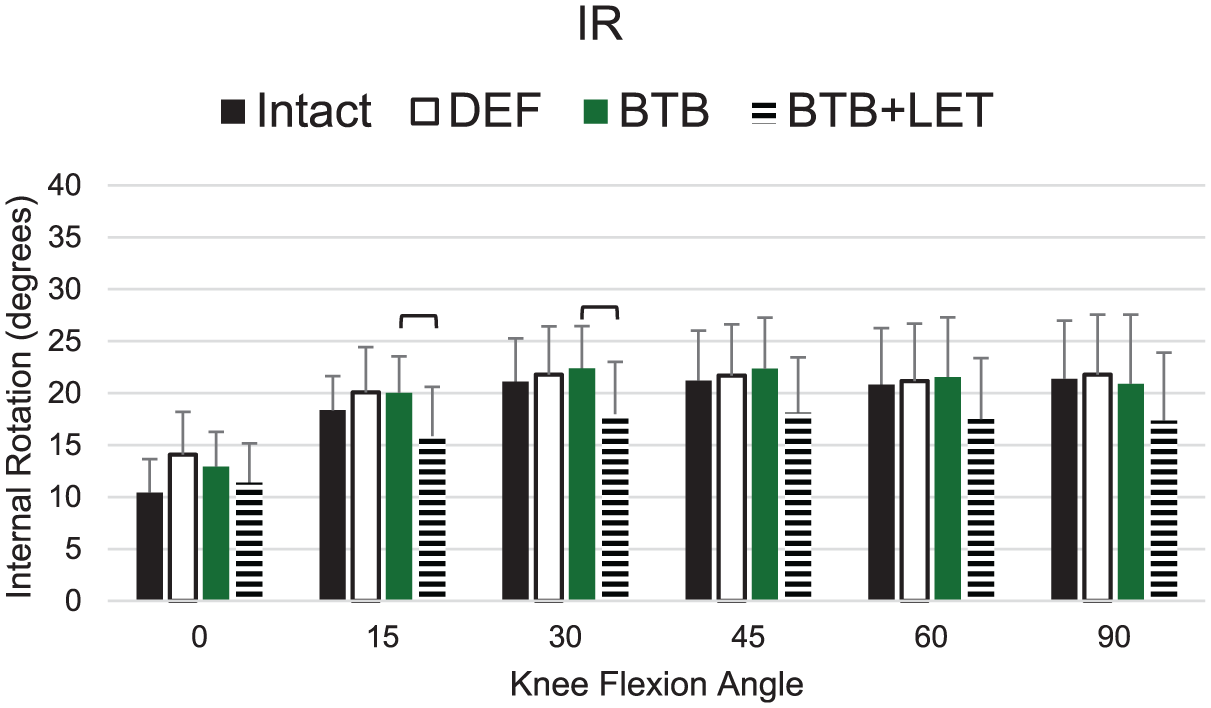
Internal rotation (IR) under 5-Nm IR tibial torque for bone–patellar tendon–bone (BTB) anterior cruciate ligament reconstruction (P < .05 BTB vs BTB+LET groups). DEF, deficient; LET, lateral extra-articular tenodesis.

Internal rotation (IR) under 5-Nm IR tibial torque for iliotibial band (ITB) anterior cruciate ligament reconstruction (
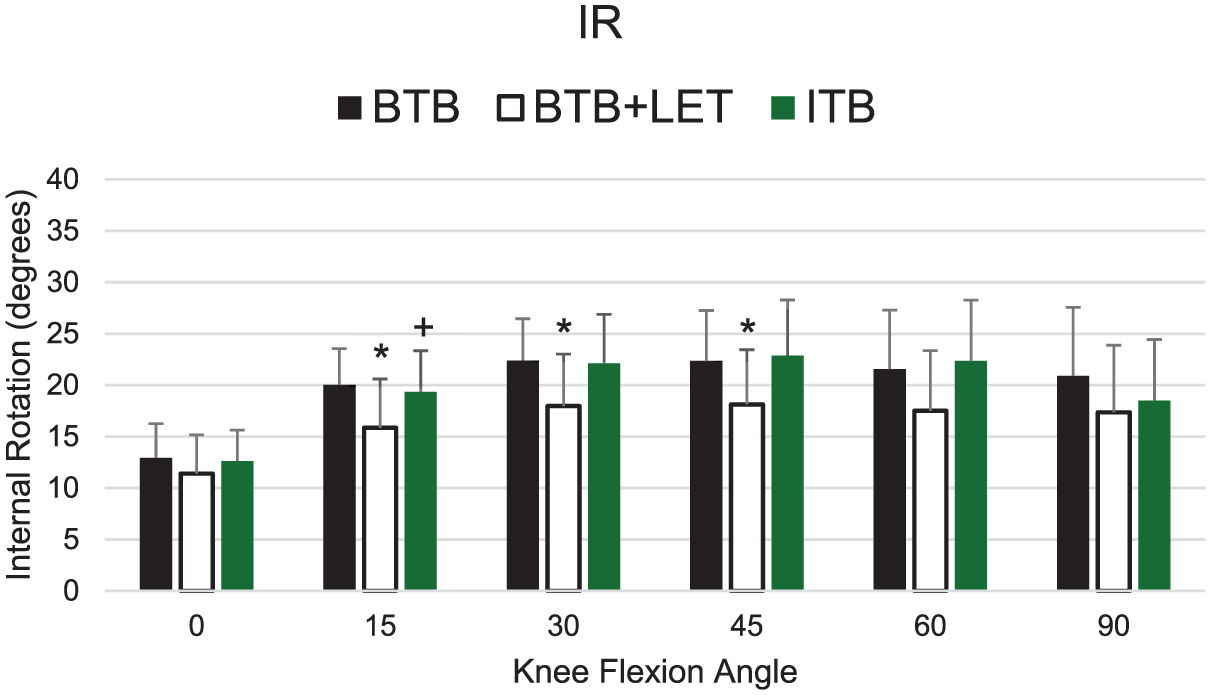
Internal rotation (IR) under 5-Nm IR tibial torque for bone–patellar tendon–bone (BTB) and iliotibial band (ITB) anterior cruciate ligament reconstruction (*P < .05 BTB vs BTB+LET; +P < .05 ITB vs BTB+LET). LET, lateral extra-articular tenodesis.
In response to PS simulation, no statistically significant difference was detected between the BTB and intact states at any knee flexion angle (P > .05) (Figure 8). There were significant reductions in the tibial displacement at 0° (P = .048), 15° (P = .02), and 30° (P = .03) of knee flexion between BTB ACL-R with LET and BTB ACL-R without LET. Statistically significantly less tibial displacement was detected in BTB+LET state compared with intact state at 15° of knee flexion (MD, 1.7 ± 0.5 mm; P = .04). In response to PS simulation, while higher tibial displacement was detected in the ITB state compared with the intact state at 0° (mean 1.7 ± 0.4 mm; P = .008) and 15° (mean 1.8 ± 0.5; P = .02) of knee flexion, no statistically significant difference was found between both states at 30° of knee flexion (P > .05) (Figure 9). Further, no statistically significant difference was detected between the BTB and ITB states during PS simulation at any knee flexion angles (P > .05) (Figure 10). In response to PS simulation, significantly less tibial displacement was detected in the BTB+LET state compared with the ITB state at 0° (MD, 1.9 ± 0.5 mm; P = .004), 15° (MD, 3.6 ± 0.7 mm; P < .001), and 30° (MD, 3.1 ± 0.8 mm; P = .002) of knee flexion.
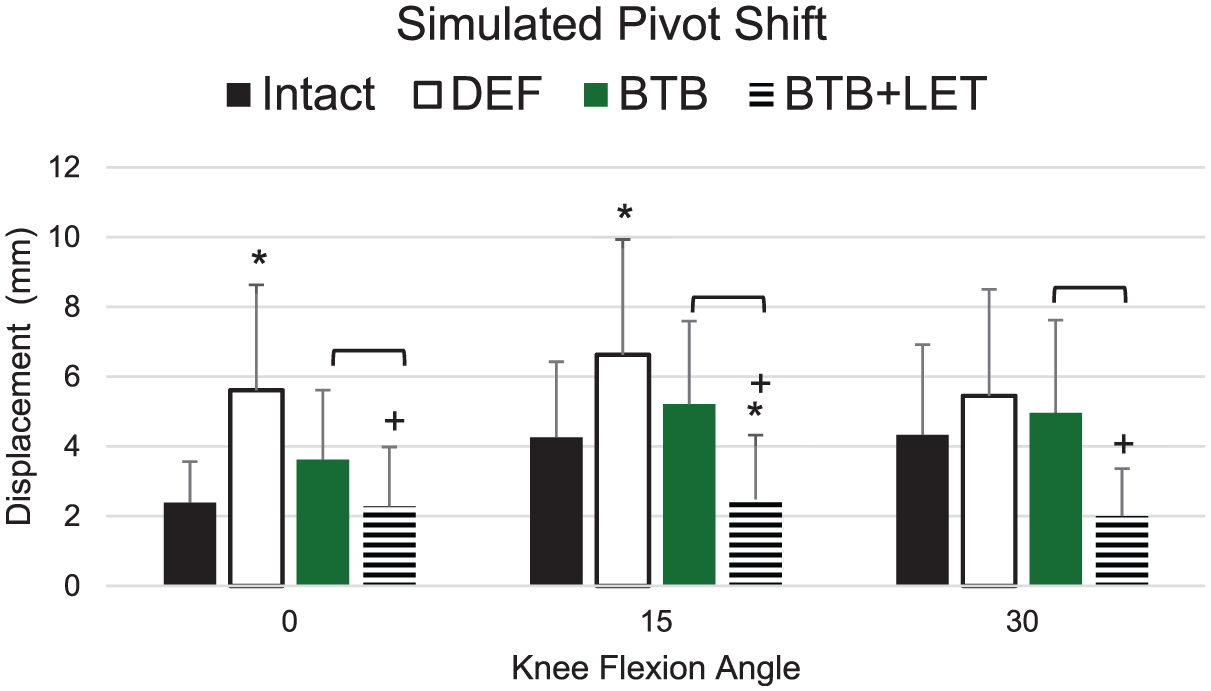
Anterior tibial displacement (mm) under simulated pivot-shift loading for bone–patellar tendon–bone (BTB) anterior cruciate ligament reconstruction (*P < .05 vs intact; +P < .05 vs DEF; ⎴P < .05 between BTB and BTB+LET groups). DEF, deficient; LET, lateral extra-articular tenodesis.

Anterior tibial displacement (mm) under simulated pivot-shift loading for iliotibial band (ITB) anterior cruciate ligament reconstruction (*P < .05 vs intact). DEF, deficient.

Anterior tibial displacement (mm) under simulated pivot-shift loading for bone–patellar tendon–bone (BTB) and iliotibial band (ITB) anterior cruciate ligament reconstruction (*P < .05 BTB vs BTB+LET; +P < .05 ITB vs BTB+LET) LET, lateral extra-articular tenodesis.
Discussion
The most important finding of this study was that no statistically significant difference was found during AT loading, IR torque, and simulated PS between BTB and ITB states at all knee flexion angles. In response to AT loading, significantly less translation was detected in the BTB+LET state compared with the ITB state at 15°, 30°, and 60° of knee flexion. In response to IR torque, the only statistically significant difference between ITB and intact state was at 0° of knee flexion. In response to simulated PS, significantly less tibial displacement was detected in the BTB+LET state compared with the intact state at 15° of knee flexion. The hypothesis that ITB ACL-R would lead to improved knee laxity similar to BTB+LET was not found with the laxity in IR and simulated PS displacement generally being between BTB alone and BTB+LET.
Although high rates of return to sport are achieved after ACL-R in adolescents, high rates of ACL-R failure are also reported in this age group.7,9 Because the lowest failure rates are reported following ACL-R with BTB autograft, it has been the subject of many biomechanical studies18,26; however, the results have been conflicting.14,29 Two recent studies reported no statistically significant difference in ATT between ACL-R performed with BTB and intact knees during AT loading.14,25 Another biomechanical study, however, reported that higher ATT was observed after BTB ACL-R at 0° to 60° of knee flexion when compared with intact knees. 19 In our study, while there was no statistically significant difference during anterior loading at 90° of knee flexion, higher ATT was detected after ACL-R at all other flexion angles compared with the ACL intact. In addition, no statistically significant difference in ATT was found between BTB and ITB during AT loading.
There is general support in the literature that ACL-R with LET augmentation provides similar stability to the intact knee during AT loading.19,25 One study reported that with LET augmentation fixed at 70° knee flexion with 44-N tension, similar ATT was detected to the intact state only at 30° and 90° of knee flexion in response to AT loading. 25 Another study reported that, with LET augmentation fixed with 20-N tension at 30° knee flexion, similar ATT was detected at all knee flexion angles with the intact ACL. 19 However, in our study, statistically significant difference ATT was detected between the BTB+LET and intact ACL during AT loading at flexion angles other than 90°. This may be due to the knee flexion angle or the applied tension of the LET fixation.
While a minimal increase in IR has been reported in ACL-deficient knees, 31 IR plays a major role as one of the most important causes of noncontact ACL injury in pivoting action. 2 Several biomechanical studies have shown that in response to IR torque, rotational stability similar to the intact knee can be achieved with ACL-R with and without LET augmentation.3,19 However, one study reported that overconstraint of the knee was observed at 0° knee flexion of knee flexion during IR torque after LET augmentation. 14 In our study, it was found that ACL deficiency led to increased rotation near full extension. With the reconstructions, there was an increase in IR from the intact ACL at 0° knee flexion with ITB ACL-R and at 0° and 15° with BTB ACL-R, while no difference was found with BTB+LET ACL-R. Although LET augmentation reduced rotation below that of the intact knee, it was not significantly different.
It is recommended to add extra-articular surgeries during ACL-R surgery in adolescent athletes and patients with high-grade rotatory instability as detected by the PS test.16,37 There are time-zero studies in the literature reporting that similar stability of an intact knee can be obtained during PS simulation following ACL-R with BTB autograft.3,17,25 However, there are also biomechanical studies reporting that higher tibial displacement occurs following ACL-R compared with the intact knee with simulation PS loading at 30° of knee flexion.14,40 In our study, rotatory stability similar to an intact knee was achieved with ITB ACL-R only at 30° of knee flexion in response to PS simulation. Furthermore, no statistically significant difference was detected at any knee flexion angles between the BTB and ITB ACL-R during simulated PS loading; however, the addition of LET to the BTB ACL-R significantly reduced the laxity compared with BTB ACL-R alone.
There is an ongoing debate in the literature as to whether LET augmentation causes overconstraint of the ACL reconstructed knee. 35 Two recent biomechanical studies reported that the addition of LET augmentation to ACL-R causes overconstraint at 15° and 30° of knee flexion during PS simulation.14,25 However, it has been reported that the effect of LET augmentation on ACL-reconstructed knee stability is temporary in a recent randomized controlled study. 5 In our study, while overconstraint was observed in the BTB+LET state at 15° of knee flexion during simulated PS loading, statistically significantly less tibial displacement was observed in BTB+LET state compared with ITB and BTB at all knee flexion angles. No difference was found between the BTB and ITB reconstructions.
Limitations
This study has several limitations. This is a time-zero study and is not able to evaluate the effects of healing following ACL-R. Also, the properties of cadaveric grafts may be different from living tissue. The specimens were not of adolescent age and the majority were male. Finally, the LET augmentation was fixed under 20-N tension at 70° knee flexion, and these results may not be generalizable for other anterolateral ligament reconstructions and other lateral extra-articular procedures. Also, the clinical impact of overconstraint of the LET procedure has not yet been fully evaluated. With ITB ACL-R, the size of the graft is dictated by the size of the tissue and in general was smaller than the BTB grafts.
Conclusion
This cadaveric study determined that BTB and ITB ACL-R both improved knee stability compared with the ACL-deficient state in response to AT, IR, and simulated PS loading; however, no method restored the intact ACL behavior. BTB+LET caused overconstraint at 15° of knee flexion during simulated PS loading. ITB ACL-R provides an alternative technique to improve stability of the ACL-deficient knee.
Footnotes
Final revision submitted April 12, 2025; accepted May 29, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: E.A.O. has received grants from ESSKA–University of Pittsburgh Sports Medicine Clinical and Research Fellowship and the Scientific and Technological Research Council of Turkey. V.M. is a board or committee member of the ACL Study Group, AOSSM, International Society of Arthroscopy, Knee Surgery & Orthopaedic Sports Medicine, and J ISAKOS; has received other financial or material support from Arthrex Inc, Smith & Nephew, and Springer; is an editorial or governing board member of Knee Surgery, Sports Traumatology, Arthroscopy; is a paid consultant for Smith & Nephew; and receives publishing royalties from Springer. Y.-M. Y. is an editorial or governing board member of the American Journal of Sports Medicine and a paid consultant for Smith & Nephew. B.H. has received other financial or material support from Allosource, Springer, and Vericel; holds stock or stock options in Imagen Technologies Inc; is a board or committee member of the Pediatric Orthopaedic Society of North America and Pediatric Research in Sports Medicine; and receives publishing royalties from Springer. M.M. has received other financial or material support from Kairos Surgical Inc. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Pittsburgh for the use of cadaveric knee specimens (No. CORID ID 1148).