
Abstract
Background:
Bone block length for bone–patellar tendon–bone (BPTB) anterior cruciate ligament (ACL) reconstruction has traditionally been 25 mm in length. The previous surgical technique did not require the surgeon to pay particular attention to the length of the bone block, and therefore, there is scant evidence in the literature describing ideal lengths. With the gaining popularity of accessory medial portal drilling of the femoral tunnel, concerns with tunnel length and graft shuttling have surfaced. Newer techniques have advised shortening of the femoral bone block to accommodate the shorter tunnel and for ease of bone block manipulation into the aperture of the tunnel.
Purpose:
To compare the effects of bone block length on the pull-out strength of patellar tendon grafts using metal interference screws in a porcine ACL reconstruction model. The hypothesis was that the pull-out strength of each length of bone block under cyclic and ultimate load to failure testing would surpass the physiologic loads experienced by a normal ACL.
Study Design:
Controlled laboratory study.
Methods:
This study used 27 unmatched porcine femurs and BPTB constructs. Specimens were randomly assigned to a 10-, 15-, or 20-mm bone block reconstruction and a cycle load of 100, 500, or 1000 cycles. This resulted in 9 specimen groups with 3 specimens in each group. A central composite design (CCD) for the test matrix was selected, as this was optimum for requiring relatively few experiments while still exploring the complete range of interest for 2 independent variables. Each reconstruction used a 7 × 20–mm titanium interference screw. All reconstructions were performed on the femoral side using 10-mm-wide patellar tendon grafts, and tensile tests were performed. The loading protocol started with a 20-N preload, then cyclic testing to the appropriate number of cycles in the elastic region between 50 and 150 N at a strain rate of 200 mm/min, and then ended with ultimate load-to-failure testing. Ultimate load to failure, peak stress, elongation, and stiffness were all recorded. The patellar tendon graft mode of failure was measured by visual inspection.
Results:
During load-to-failure testing, 5 of 9 graft constructs in the 10-mm group failed at the bone block, while 2 of 9 failed in the 15-mm group at this interface. In the 20-mm group, all 9 specimens failed at the tendon, and none failed at the bone block. There was a statistically significant difference in modes of failure between the bone block length groups in the reconstructed ACL grafts. Analysis indicates that a smaller bone block length graft is more likely to fail due to a bone block failure than a tendon failure. The average ± standard deviation failure load for all specimens was 573 ± 171 N. The mean failure loads for the 10-, 15-, and 20-mm groups were 614 ± 110, 658 ± 92, and 540 ± 203 N, respectively. There was no statistical significance between the groups in any of these measurements.
Conclusion:
Bone blocks of 20 to 25 mm in length are normally used in surgical practice. Thus, the purpose of this study was to explore the effects of a smaller bone block length in the fixation strength of a graft. This study could not yield a significant difference in failure load for differently sized bone blocks. There was a significant tendency of shorter bone block lengths to fail due to bone block failure.
Clinical Relevance:
Bone block failure was defined as slippage of the bone block or interference screw. These results show that using a smaller bone block may increase the likelihood of a graft failure in an ACL reconstruction.
Bone block length for bone–patellar tendon–bone (BPTB) anterior cruciate ligament (ACL) reconstruction has traditionally been 25 mm, since first described by Jones 7 and Clancy et al 5 in 1963 and 1982, respectively. The surgical technique at the time did not require the surgeon to pay particular attention to the length of the bone block, and therefore, there is scant evidence in the literature describing ideal lengths.
With the gaining popularity of accessory medial portal drilling of the femoral tunnel, concerns with tunnel length and graft shuttling have surfaced. 8 Newer techniques have advised shortening of the femoral bone block to accommodate the shorter tunnel and for ease of bone block manipulation into the aperture of the tunnel. Only 1 study, to date, has looked at the length of bone block. Meuffels et al 9 performed a biomechanical test of 10- versus 20-mm bone block in ultimate load-to-failure testing and showed no statistical difference between the 2 lengths. However, this study was not performed with cyclic loading, which more accurately replicates the in vivo rehabilitation environment of the early post-ACL reconstructed knee.
The goal of this study was to compare the effects of bone block length on the pull-out strength of patellar tendon grafts using metal interference screws in a porcine ACL reconstruction model. Our hypothesis was that the pull-out strength of each length of bone block under cyclic and ultimate load-to-failure testing would surpass the physiologic loads experienced by a normal ACL.
Materials and Methods
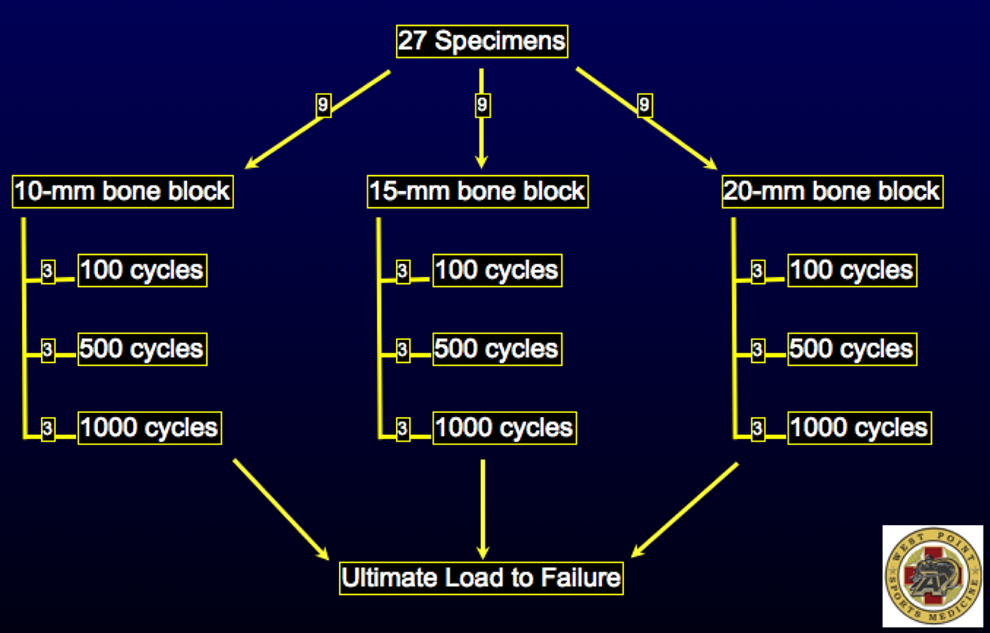
This study used 27 unmatched porcine femurs and BPTB constructs. The specimens were randomly assigned to a 10-, 15-, or 20-mm bone block reconstruction. They were then randomly assigned a cycle load of 100, 500, or 1000 cycles. This resulted in 9 specimen groups, with 3 specimens in each group (Figure 1). A central composite design (CCD) for the test matrix was selected as this was optimum for requiring relatively few experiments while still exploring the complete range of interest for 2 independent variables. The corresponding CCD test matrix requires 9 experimental groups, as shown in Table 1. The CCD used for this experiment is a face-centered design. The first 4 experiments are based on sampling the design space extremes using a 2k full factorial orthogonal array design. Then, intermediate points are sampled in the last 5 experiments, with the center point sampled in experiment number 5. 6 To provide insight into test-to-test variability within an experimental group, 3 samples were tested for each experimental setting.
Central Composite Design (CCD) for Testing

Central composite design of the testing protocol.
Each reconstruction used a 7 × 20–mm titanium interference screw (Arthrex, Naples, Florida, USA). All reconstructions were performed on the femoral side using 10-mm-wide patellar tendon grafts. Each femur was cut approximately 3 inches above the knee joint, though this depended on the size of the femur. All soft tissue was debrided to allow proper placement of the graft. The tunnels were positioned to a standard 11 o’clock position for the right knee and 1 o’clock position for the left knee. The tunnels were reamed to the length of the bone block. Tensile tests were performed using a tensile testing machine (MTS Insight 150SL loading machine; MTS, Eden Prairie, Minnesota, USA). All loading was completed parallel to the long axis of the graft construct (Figure 2).

Specimen setup with graft tension parallel to long axis of the femur.
Our loading protocol started with a 20-N preload, then cyclic testing to the appropriate number of cycles in the elastic region between 50 and 150 N at a strain rate of 200 mm/min, and ended with ultimate load-to-failure testing. Ultimate load to failure, peak stress, elongation, and stiffness were all recorded using the MTS Test Works V.4 software (MTS). Patellar tendon graft mode of failure was measured by visual inspection.
Statistical Analysis
One-way analysis of variance (ANOVA) was used to calculate significant differences in failure mode when groups were based on bone block length. Significance was set at P < .05. All tabulated data are presented using mean values; nonparametric statistical methods were required to account for the discrete nature of the failure modes. Chi-square analysis and correlation studies for each bone block group were performed in addition to the initial 1-way ANOVA. SPSS software was utilized to perform the majority of the statistical analysis (version 19.0; IBM, Armonk, New York, USA).
Results
During load-to-failure testing, 5 of 9 graft constructs in the 10-mm group failed at the bone block, while 2 of 9 failed in the 15-mm group at this interface. In the 20-mm group, all 9 specimens failed at the tendon, and none failed at the bone block (Figure 3). There was a statistically significant difference in modes of failure between the bone block length groups in the reconstructed ACL grafts. The analysis indicates that a smaller bone block graft length is more likely to fail due to a bone block failure than a tendon failure, as depicted in Table 2. One-way ANOVA indicated statistically significant differences (P = .022). Post hoc testing was not possible since one of the failure modes had a sample set of 1. Correlation analysis was conducted using the Spearman rank correlation coefficient to verify statistical dependence between the groups. This analysis also indicated statistical dependence with 2-tailed significance at .012. Chi-square analysis was then performed to look at differences between the paired groups (10 vs 15 mm, 15 vs 20 mm, and 10 vs 20 mm). All comparisons between pairs indicated statistically significant differences, with P < .05.
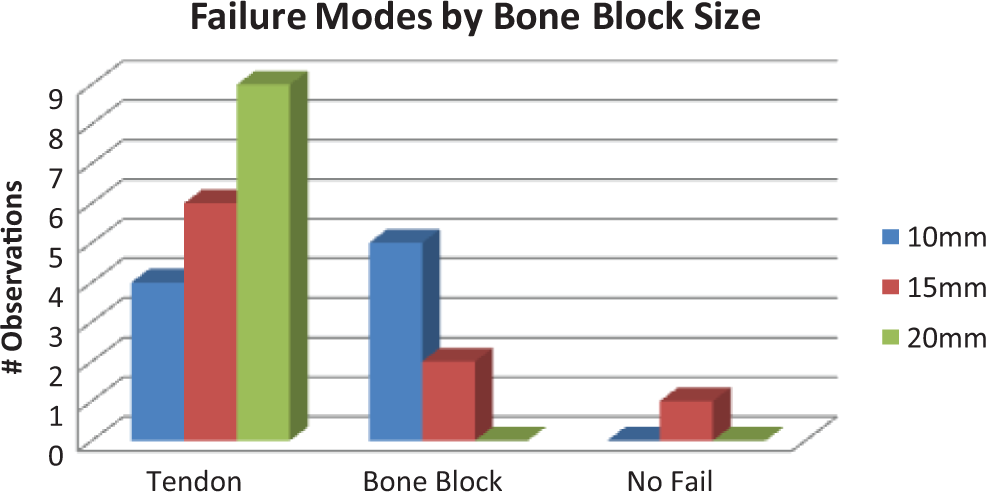
Failure modes for each construct size. The “no fail” condition occurred only when the maximum load was reached at 1000 N for the attached load cell.
Mode of Failure a

a BB, bone block failure; NF, no failure; T, tendon failure.
The mean ± standard deviation failure load for all specimens was 573 ± 171 N. For the 10-, 15-, and 20-mm groups, respectively, the mean failure loads were 614 ± 110, 658 ± 92, and 540 ± 203 N; mean stiffness values were 101.4, 135.5, and 100.8 N/mm; and mean elongation values were 2.43, 3.23, and 3.53 mm. There was no statistical significance between groups in any of these measurements. All data for the respective bone block lengths can be seen in Table 3.
Bone Block Length: Mean Values a

a SD, standard deviation.
Cyclic Loading: Mean Values

Table 4 shows the mean values for each of the group’s 9 specimens under different loading cycles. Each group contained 3 specimens of each bone block length. Last, we found that failure load, stiffness, and peak stress were not statistically different as the number of cycles increased from 100 to 1000 cycles. However, on average, elongation was greater and stiffness was lower as cycle number increased, as should be expected.
Discussion
Bone blocks of 20- to 25-mm length are normally used in surgical practice. Thus, the purpose of this study was to explore the effects of a smaller bone block length in the fixation strength of a graft. This study did not yield a significant difference in failure load for different sized bone blocks. However, it did result in a significant tendency of shorter bone block lengths to fail due to bone block failure. Bone block failure was defined as slippage of the bone block or interference screw. These results show that using a smaller bone block may increase the likelihood of a graft failure in an ACL reconstruction.
However, the average failure loads for the smaller bone blocks were actually higher than in the 20-mm group. They were also able to withstand a greater peak stress before failure. In all bone block groups, the average failure loads were sufficiently higher than loads normally found in early rehabilitation exercise that near 200 N. 13
The 7 bone block failures were all found in the 10- and 15-mm bone blocks. Two failures occurred during cyclic loading. It is suggested that these specimens may have failed because of surgeon error or specimen variability, and are therefore considered anomalies. Of the remaining 5 failures, the lowest failure load was 543 N. This suggests that even though these failures were attributed to bone block failure, they may have been sufficient enough for ACL reconstruction purposes.
The cyclic loading was designed for the elastic region of the graft. It was intended to serve as a more ideal replication of an in vivo environment. Real-life applications are not usually 1 single load to failure actions. In early stages of rehabilitation following ACL reconstruction, the loading on the knee would model closer to a cyclic test than an ultimate failure load. 3,10,12 The cyclic loading results show that failure load and peak stress did not decrease with an increase in the number of cycles. The data also show that elongation increased as the cycle count increased, which is expected as longer time under stress should stretch the tendon length.
We chose to use porcine bone to model the bone–patellar tendon graft construct. This was done because of the easy availability of porcine specimens and their relatively low cost. All tested specimens came from pigs of the same farm and were considered to be relatively homogeneous. Young and elderly human cadavers can differ greatly, but porcine models were not found to have a statistical difference compared with young, human cadaver models. 2 A similar study contrasting the fixation strengths of 10- and 20-mm bone blocks used cadavers in their model. However, cadavers have been found to produce small populations of disproportionally high-age models. The biomechanical properties of porcine bone are comparable to human bone. Thus, many studies have transitioned to the use of animal tissue, thereby alleviating issues related to cost restraints, availability limitation, and human tissue regulation. 1
The tensile machine applied a force parallel to the long axis of the graft. This force applies the maximum amount of stress to the graft and is most likely to cause a graft failure. 14 This test design is ideal for replicating the worst loads a patellar tendon graft complex may endure immediately following ACL reconstruction.
The failure loads were slightly higher than studies that used human cadavers, but the means are within 100 N of each other. 2,4 Rupp et al 13 recorded a passive load of 128 ± 15 N and an active extension load of 219 ± 25 N for tensile forces in the human BPTB graft. All initial fixation strengths, with the exception of the 2 cyclic failures, greatly exceeded these loads. This suggests that most of these grafts would have sufficient fixations for rehabilitation purposes.
This study found that there is a statistical significance between distributions of failure mode when the bone block length is isolated as the factor of interest; a smaller bone block is more likely to fail before the tendon fails. However, the average values for ultimate failure load were above known sufficient values for initial fixation strength needed in early rehabilitation. This study may give surgeons clinical confidence if a smaller bone block size is necessary, but more research is needed to determine the exact effects of this smaller length. This study concluded that a graft failure is more likely in smaller bone blocks, but future research should be concentrated on whether those specimens reached a load with sufficient fixation for reconstruction purposes.
Limitations
It has been suggested that mean bone density can be used to help compare porcine bone strength to that of a healthy human specimen, even if the models differ. 11 This could be a possible solution to the difference in properties of porcine and cadaver bones. Although this study did not incorporate this practice, future biomechanical studies involving porcine models should consider this control.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: Arthrex supplied the interference screws and kit for graft fixation. The Army Research Lab awarded a grant to purchase porcine grafts and other tools for fixation purposes.
Acknowledgment
The authors thank Mr Michael Boss, Mr Jeff Butler, and Mr Rod Wilson from the Department of Civil and Mechanical Engineering at United States Military Academy for their expert technical assistance.