
Abstract
Background:
The anterior cruciate ligament (ACL) is essential for knee stability, and reconstruction aims to restore functionality. High secondary ACL injury rates after primary ACL reconstruction (ACLR) pose significant clinical, public health, and economic challenges. Although tibial spine height (TSH) has been identified as a risk factor for primary ACL injuries, its role in secondary ACL injury after primary ACLR remains poorly understood.
Purpose:
To investigate whether the increase in TSH between pre- and postoperative MRI measurements is associated with secondary ACL injury after primary ACLR.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
A case-control study was conducted at a single institution, including 32 patients who underwent revision surgery after noncontact secondary ACL injury and 107 patients who maintained intact ACL grafts without revision after primary ACLR during a minimum 2-year follow-up period. The primary outcome was the increase in TSH between pre- and postoperative MRI scans. Logistic regression was used to examine the association between the increase in TSH and secondary ACL injury, and the area under the receiver operating characteristic (ROC) curve (AUC) was calculated to assess the model's discriminative ability. Other imaging characteristics and anteroposterior instability using KT-2000 were analyzed.
Results:
Each 1-mm increase in postoperative medial TSH (MTSH) was associated with secondary ACL injury (adjusted odds ratio, 7.62; 95% CI, 3.80-18.55; P = .0001). This increase in MTSH (postoperative value minus preoperative value) suggests potential bony changes after ACLR that may be associated with secondary ACL injury risk. Additionally, the notch width index was smaller in the secondary ACL injury group compared with the control group. The increase in MTSH demonstrated strong diagnostic potential for predicting secondary ACL injury using a threshold value derived from our ROC analysis. Specifically, the AUC of 0.93 ± 0.034 indicates the model's ability to discriminate between patients who developed secondary ACL injury and those who maintained intact ACL grafts based on the increase in MTSH.
Conclusion:
This study demonstrates a significant association between increased MTSH and secondary ACL injury after primary reconstruction. Using a 1-mm increase in MTSH as the cutoff value, our model showed excellent discriminative ability in predicting secondary ACL injury (AUC, 0.93; 95% CI, 0.86-0.99; sensitivity, 77.42%; specificity, 98.13%). These findings suggest that evaluating after reconstruction MTSH changes, particularly increases of ≥1 mm, may serve as a valuable risk assessment tool for secondary ACL injury.
The anterior cruciate ligament (ACL) is crucial for knee stability, and its reconstruction (ACLR) aims to restore function.3,13,26 However, secondary ACL injuries after reconstruction are common and pose significant clinical, public health, economic, 14 and psychological challenges.2,20 Long-term studies report cumulative failure rates of 11.9% at ≥10 years after surgery. 5 Graft failure occurs in 9% to 11% of patients within 2 years. 23 Secondary ACL injuries lead to increased morbidity, extended rehabilitation, and reduced quality of life, with broader societal implications, including higher health care costs and potential long-term disabilities. 4
Previous studies have explored the risk factors for primary ACL injury, including age,1,11,16 autograft use,17,21 surgical techniques, 1 obesity, 16 and imaging findings, such as bone tunnel position,18,27 larger lateral posterior tibial slope,7,25 and smaller medial posterior tibial slope. 8 However, studies examining the predictive factors for secondary ACL injury after reconstruction, particularly tibial spine height (TSH), are limited. Nie et al 19 reported that higher lateral TSH (LTSH) heights could be a risk factor in male patients. Additionally, lower medial tibial spine volume (MTSH) has been identified as a risk factor for primary ACL injury 24 ; but another study has suggested that lower MTSH and LTSH heights are common compared with normal knees. 10 Smaller tibial spines might lead to abnormal knee motion after reconstruction, 15 whereas the mechanism of TSH is still unclear.
We hypothesize that an increase in TSH after primary ACLR will be associated with secondary ACL injury after reconstruction because of its potential to reflect joint instability and compensatory bone changes. This study used magnetic resonance imaging (MRI) for the precise temporal assessment of TSH to investigate its potential as an association with secondary ACL injury.
Methods
Study Design and Setting
This case-control study was conducted at a single university hospital between 2009 and 2023. Our center maintains a high patient retention rate due to its geographical and social characteristics, including low population mobility and flexible scheduling for follow-up visits. The study focused exclusively on patients who underwent primary ACLR between 2009 and 2021, comparing those who required revision surgery because of secondary ACL injury with those who maintained intact grafts during a minimum 2-year follow-up period. For the analysis, we focused on patients diagnosed with secondary ACL injury and matched them at a ratio of approximately 1:4 based on age and sex with patients who had been followed up for ≥2 years without secondary ACL injury. The institutional review board approved the study, ensuring adherence to ethical guidelines and the Strengthening the Reporting of Observational studies in Epidemiology statement.
Participants
Between January 2009 and April 2021, 596 patients underwent ACLR at our institution. The following exclusion criteria were applied for both groups: (1) age ≥30 years at primary ACLR, (2) bilateral injury, (3) follow-up period <2 years, (4) combined ligament injuries (posterior cruciate ligament, medial collateral ligament, or lateral collateral ligament), (5) no preoperative MRI available, (6) traffic accident–related injuries, and (7) incomplete medical records. An additional criterion for the case group only was contact injury mechanism. Of the initial 596 patients, 71 experienced secondary ACL injury. After applying the exclusion criteria, 32 patients with noncontact injuries were included in the case group. Among the 71 patients, 39 were excluded based on these criteria: (1) no preoperative MRI (n = 22), (2) combined ligament injuries (n = 10), and (3) incomplete records (n = 7). From the 525 patients without secondary ACL injury, we randomly collected 107 patients who met all criteria, for the control group. The final study groups were defined as (1) the case group: patients who sustained a secondary noncontact ACL injury after primary ACLR (n = 32); and (2) the control group, those patients who maintained an intact ACL graft after primary ACLR without secondary injury during the minimum 2-year follow-up period (n = 107) (Figure 1).

Study flowchart. ACL, anterior cruciate ligament; MRI, magnetic resonance imaging.
Demographic Data
Age, sex, height, weight, body mass index (BMI), duration between injury and surgery, observation period, primary injury mechanism (contact vs noncontact), duration between surgery and secondary ACL injury, Tegner activity score before and after surgery, type of graft used, graft diameter on the femoral and tibial sides, length of the femoral bone tunnel, presence of medial and lateral meniscal injuries, and augmentation method were evaluated.
Primary Outcome
The primary outcome was TSH measured on preoperative and postoperative MRI scans. TSH was measured as follows: the highest point of each tibial plateau (medial and lateral) was identified on coronal MRI slices; a tangent line was drawn at each plateau's surface; and the perpendicular distance from the tibial spine peak to this tangent line was measured in millimeters. The change in TSH was defined as the postoperative minus the preoperative value, with positive values indicating an increase and negative values a decrease. Postoperative MRI was performed either 1 year after surgery or before revision in the case group, and at 1 year or the final follow-up visit in the control group. Although MRI scans were obtained from multiple systems rather than a single standardized machine, all measurements were performed using standardized anatomical landmarks to ensure consistency. A single blinded evaluator conducted all measurements (K.G.) (Figure 2).

Morphological evaluation of the tibial spine using magnetic resonance imaging. A tangent was drawn at each sliced highest part of the medial tibial plateau and the most elevated part of the lateral tibial plateau. The distance from the upper ends of the tibial spine (A and C) to the tangent line (B and D) is considered the height of the lateral tibial spine or the medial tibial spine. The distance between the lines drawn from the upper ends of the tibial spine to the tangent was considered the tibial spine.
Secondary Outcomes
We selected other imaging characteristics based on previous studies that identified potential risk factors for secondary ACL injuries after primary ACLR. We evaluated the posterior tibial slope (medial or lateral), 28 notch width at the level of the popliteal sulcus, notch width at the level of the joint line, 9 tibial spine width, notch outlet length (NOL), distance between the lateral and medial posterior condyles, and notch width index (NWI)6,10 (Figures 2 -4). All measurements were performed by a single evaluator (K.G.) blinded to the study objectives.
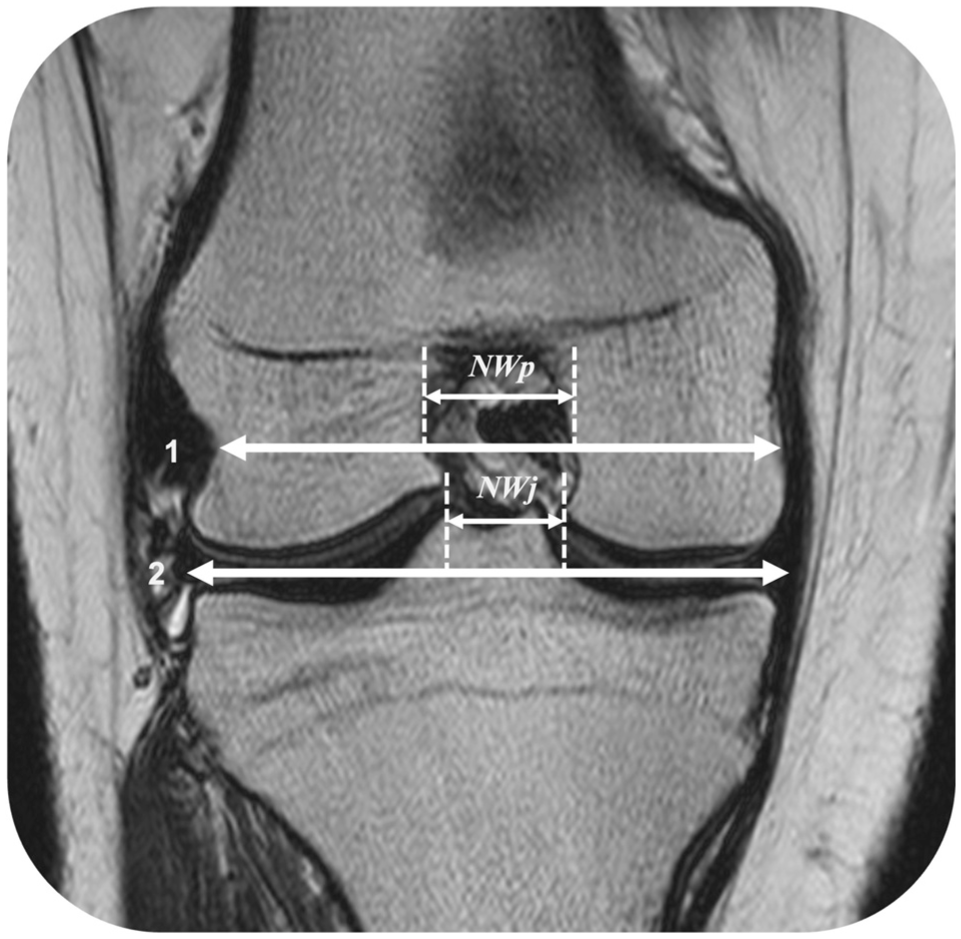
Measurements on coronal images show a tangential line (2) drawn between the femoral condyles and another line (1) drawn parallel to the tangential line between the 2 femoral condyles at the level of the popliteal tendon and sulcus of the lateral femoral condyle. The notch widths at the level of the joint line (NWj) and popliteal groove (NWp) were measured.

Magnetic resonance imaging (MRI) of the femoral intercondylar notch. The axial knee MRI images with the longest transepicondylar length (from E to F), notch outlet length (from G to H), the length between the medial and lateral posterior condyles (from I to J), and the notch width index (G–H/I–J× 100) were measured.
An anteroposterior instability examination was performed using the KT-2000 arthrometer, a device that quantified the anterior movement of the tibia and served as a general objective indicator; the KT-2000 is commonly used in meta-analyses for post-ACLR evaluations. 26 We measured the side-to-side difference between the affected and healthy knees before and after surgery using the KT-2000 arthrometer at 30 N of anterior force. Missing values were excluded from the evaluation.
Statistical Analysis
Sex, primary injury mechanism, graft type, presence of medial and lateral meniscal injuries, and augmentation were treated as nominal scales and analyzed using Fisher exact test. Age, height, weight, BMI, and Tegner activity score before and after surgery, as well as MRI-measured variables, underwent t test analysis if they conformed to a normal distribution and the Mann-Whitney U test if they did not. Additionally, in the logistic regression analysis, we limited the number of independent variables to 3 (increase in MTSH, posterior tibial slope of lateral side [PTSL], and NWI) based on the statistical principle that recommended approximately 10 cases per variable in multiple regression analyses. With 32 cases in our study, this allowed for a maximum of 3 explanatory variables to maintain statistical validity. These variables were chosen because the increase in MTSH was the primary hypothesis of interest in this study, and PTSL and NWI have been reported as risk factors in previous studies for imaging findings of knee joint injury.6,11 The odds ratio (OR) was calculated as an indicator of the effect, and the area under the receiver operating characteristic (ROC) curve (AUC) was calculated to evaluate the diagnostic accuracy of the increase in MTSH in identifying patients at risk for secondary ACL injury. A logistic regression analysis was performed with a classification cutoff value of 0.5. This conventional threshold was selected because it represented equal misclassification costs for both positive and negative cases. This cutoff value represented the threshold of the increase in MTSH that best discriminated between patients who developed secondary ACL injury and those who maintained intact grafts. For the sensitivity analysis, we divided the analytic cohort into male and female subgroups to evaluate whether the results were consistent across these populations. Subsequently, we conducted the same analyses using the increase in MTSH, PTSL, and NWI as explanatory variables to evaluate whether the results were consistent across these subgroups. Statistical analyses were performed using Prism10 (GraphPad), with the significance threshold set at P = .05.
Results
This study included 32 patients who underwent revision surgery as a result of secondary ACL injury after primary ACLR (18 female and 14 male patients; median age, 20.5 years) and 107 patients who maintained intact ACL grafts after primary reconstruction (55 female and 52 male patients; median age, 19.0 years) (Table 1). All demographic data, excluding height, observation period, and femoral bone tunnel length, did not follow a normal distribution and are presented as median and interquartile range. Comparison of demographic data between the 2 groups revealed differences in the observation period, postoperative Tegner score activity, semitendinosus graft, and tibial bone tunnel size (P < .05). No other significant differences in the demographic data were observed.
Demographic Data of Patients a

Data are presented as mean ± SD for normal distribution, median (IQR) for nonnormal distribution, or n (%). BMI, body mass index; N/A, not available. Bold values indicate statistical significance at p < .05.
Two-sample t test (parametric test), Mann-Whitney U test (nonparametric test), and Fisher exact test (sex, contact injury, hamstrings, augmentation, medial meniscal suture, and lateral meniscal suture) for comparison between noninjury and reinjury.
Table 2 shows the differences in the characteristic image data between the 2 groups. All image data, except for PTSM, PTSL, NOL, and NWI, followed a nonnormal distribution. The PTSM, PTSL, NOL, NWI, and MTSH over 1 year, and LTSH over 1 year were lower in the case group than in the control group (P < .05).
Comparison of Variables a

Data are presented as mean ± SD for normal distribution or median (IQR) for nonnormal distribution. LPC, length between lateral and medial posterior condyle; LTSH, lateral tibial spine height; MTSH, medial tibial spine height; NOL, notch outlet length; NWj, notch width at the level of the joint line; NWp, notch width at the level of the popliteal sulcus; NWI, notch width index; Post, postoperative; Pre, preoperative; PTSL, posterior tibial slope of lateral side; PTSM, posterior tibial slope of medial side; TSW, tibial spine width. Bold values indicate statistical significance at p < .05.
Two-sample t test (parametric test) or Mann-Whitney U test (nonparametric test) for between noninjury and reinjury.
The increase in MTSH and LTSH were significantly greater in the case group compared with the control group (P < .0001), with the case group showing larger postoperative increases in spine height. The median values of the increase in MTSH and LTSH were 2.0 mm (IQR, 1.0-2.8 mm) and 1.0 mm (IQR, 0-2.0 mm) in the case group, compared with 0 mm (IQR, 0-0 mm) and 0 mm (IQR, 0-0 mm) in the control group, respectively. The increases in MTSH and LTSH were greater in the case group than in the control group (P < .0001).
We performed multiple logistic regression using clinically significant variables (the increase in MTSH; the increase in LTSH, PTSM, PTSL, tibial bone tunnel size, NOL, NWI, MTSH, and LTSH over 1 year) as independent variables, with secondary ACL injury as the dependent variable. The logistic regression analysis revealed that the increase in MTSH was significantly associated with secondary ACL injury (P = .0001). Using a cutoff value of 1-mm increase in MTSH, the analysis showed the following: initially, the unadjusted OR was 8.97 (95% CI, 3.41-33.6) (Table 3). After adjusting for other factors, each 1-mm increase in MTSH above this cutoff was associated with 7.62 times higher odds of secondary ACL injury (adjusted OR, 7.62; 95% CI, 3.80-18.55; P = .0001) (Table 4). Given the group size of 32 patients and the ideal recommendation to have ≤3 explanatory variables, we trimmed the analysis to include the increase in MTSH, PTSL, and NWI, based on previous research.9,19 This regression revealed that increased MTSH was independently associated with revision ACLR, with an adjusted OR of 7.62 (95% CI, 3.80–18.55; P = .0001). Additionally, a smaller NWI was significantly associated with revision surgery (P = .03), with an adjusted OR of 0.81 (95% CI, 0.67-0.96), indicating that for each unit decrease in NWI, there was a higher likelihood of requiring revision surgery (Table 4).
Maximal Likelihood Estimates of Multiple Logistic Regression Model a
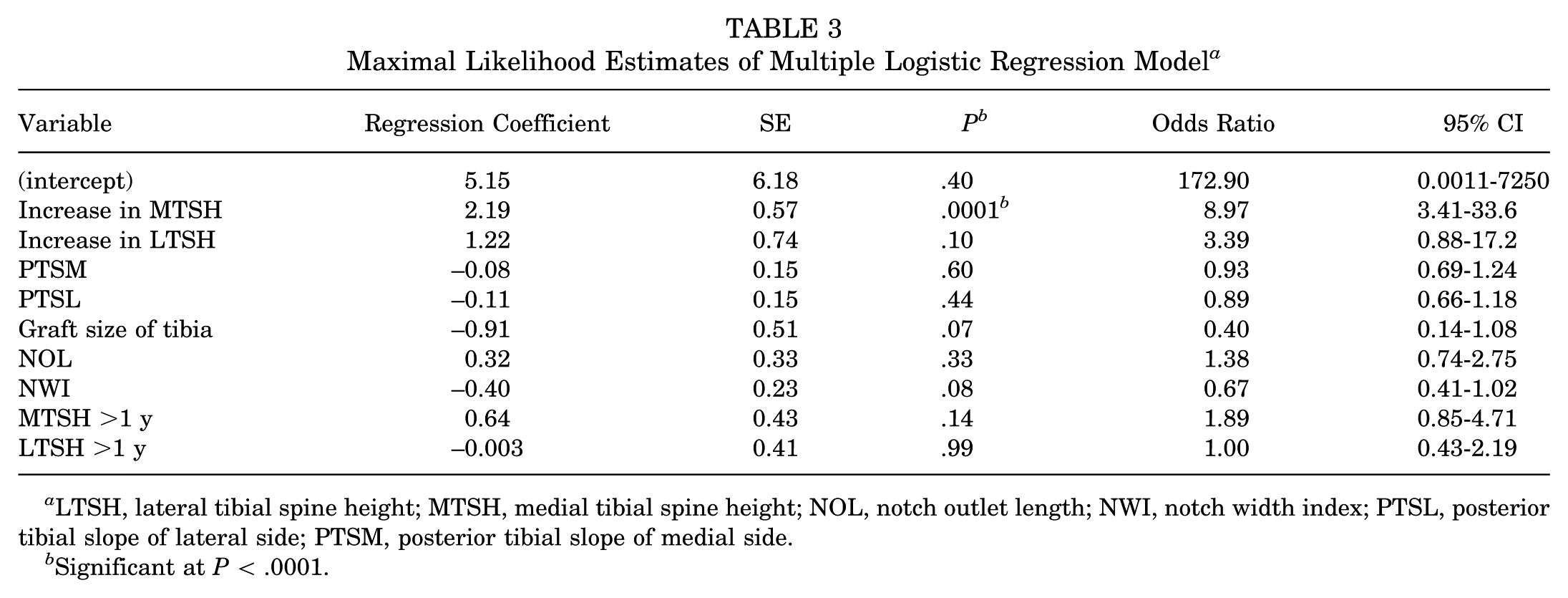
LTSH, lateral tibial spine height; MTSH, medial tibial spine height; NOL, notch outlet length; NWI, notch width index; PTSL, posterior tibial slope of lateral side; PTSM, posterior tibial slope of medial side.
Significant at P < .0001.
Adjusted Multiple Logistic Regression Model a

MTSH, medial tibial spine height; NWI, notch width index; PTSL, posterior tibial slope of lateral side.
Significant at P < .05.
For the sensitivity analysis by sex, the female subgroup showed a significant MTSH difference (P = .0007) with an adjusted OR of 20.65 (95% CI, 5.41-229.4), and NWI was significant (P = .03) with an adjusted OR of 0.59 (95% CI, 0.32-0.87). In male patients, the increase in MTSH was significant (P = .003) with an adjusted OR of 7.04 (95% CI, 2.38-32.27) (Table 5).
Multiple Logistic Regression Analyses Performed Separately for Both Sexes a
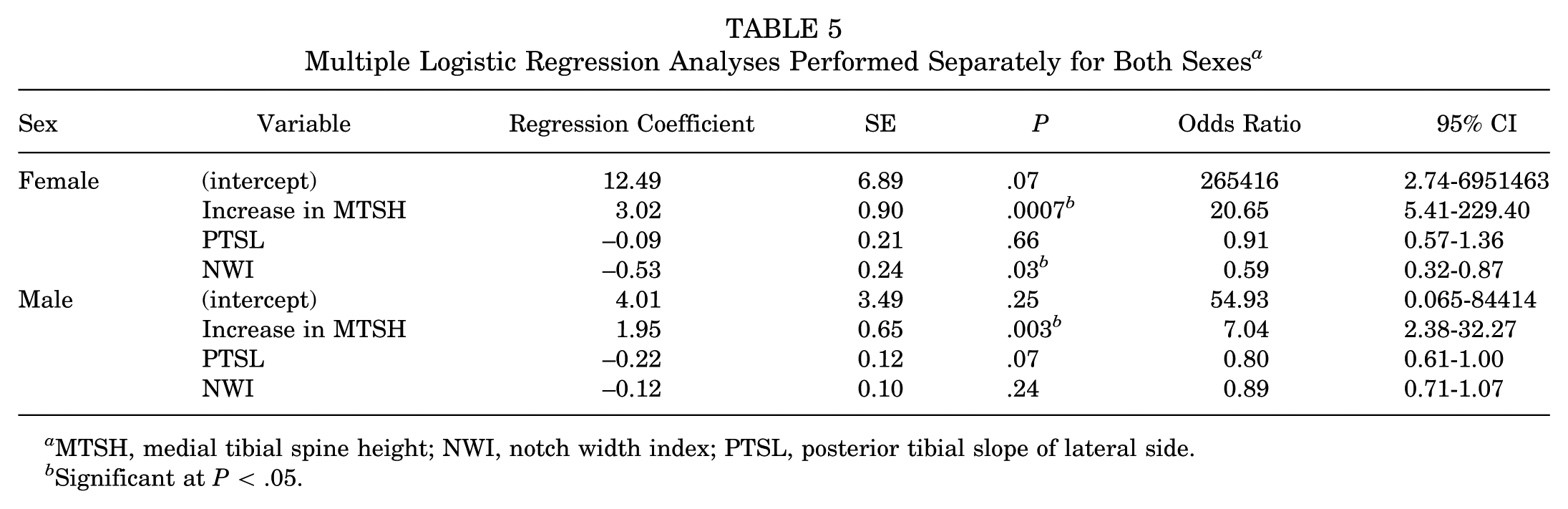
MTSH, medial tibial spine height; NWI, notch width index; PTSL, posterior tibial slope of lateral side.
Significant at P < .05.
Additionally, ROC curve analysis determined the diagnostic capability of the increase in MTSH for secondary ACL injury (Figure 5). Using a cutoff value of 1-mm increase in MTSH, the model demonstrated strong diagnostic potential with a sensitivity of 77.42% and specificity of 98.13%. This 1-mm threshold showed excellent discriminative performance with an ROC AUC of 0.93 (95% CI, 0.86-0.99).

Receiver operating characteristic (ROC) analysis of the increase in medial tibial spine height (MTSH) for predicting secondary ACL injury. The solid curve indicates the diagnostic performance of increased MTSH. The diagonal dashed line represents the reference line (area under the curve [AUC], 0.5). Using a cutoff value of 1-mm increase in MTSH, the ROC curve demonstrates excellent discriminative ability with an AUC of 0.93 ± 0.034 (95% CI, 0.86-0.99), sensitivity of 77.42%, and specificity of 98.13%. The AUC is a measure of the model's diagnostic accuracy, with higher values indicating better predictive performance. This cutoff value was determined using a classification threshold of 0.5 in the logistic regression model.
Discussion
The main finding of this study was that the logistic regression analysis showed that for every 1-mm increase in postoperative MTSH compared with preoperative measurements, the odds of secondary ACL injury were 7.62 times higher (adjusted OR, 7.62). Additionally, the case group demonstrated a significant increase in MTSH after ACLR, with measurements showing a median increase of 2.0 mm from preoperative values. This increase in MTSH was not observed in the control group.
The increase in MTSH in the postoperative secondary ACL injury may suggest compensatory bony changes in response to knee instability. Previous biomechanical studies have demonstrated that ACL deficiency leads to altered knee kinematics and increased anterior tibial translation. 3 Lansdown and Ma 15 reported that variations in tibial bone morphology, including TSH, can significantly influence knee kinematics in ACL-injured knees. The relationship between bony changes and joint instability has been well-documented in other contexts. Pottenger et al 22 demonstrated that osteophytes serve as a defensive response to knee joint instability, showing increased varus-valgus instability after osteophyte removal during artificial knee joint surgery. Similarly, Katsuragi et al 12 found a higher incidence of osteophyte formation in the intercondylar notch in patients with advanced osteoarthritis (OA) compared with those without OA over a 48-month follow-up period. From these findings, we hypothesize that increased TSH may represent a compensatory mechanism to resist anterior tibial translation in cases where ACLR has not fully restored normal knee kinematics. Therefore, the observed increase in TSH in our case group may indicate persistent anteroposterior instability after ACLR, potentially contributing to the higher risk of secondary ACL injury.
To minimize the potential confounding effect of age-related osteophyte formation on MTSH measurements, we specifically limited our study population to patients aged ≤30 years. This age restriction allowed us to focus on MTSH changes that were more likely related to postreconstruction knee biomechanics rather than degenerative changes. The increase in MTSH, with an OR of 7.62 and a high predictive accuracy based on the AUC, might be a potential risk factor for secondary ACL injury after primary ACLR.
However, the exact mechanism remains speculative, and MTSH may be influenced by surgical factors such as tibial tunnel position, with more medial placements potentially affecting postoperative spine height. Additionally, MTSH may reflect inherent morphological traits of the tibial plateau. Further research is needed to fully establish the relationship between tibial tunnel positioning and postoperative MTSH.
The lower NWI in the case group compared with the control group corroborates previous findings from randomized controlled studies that NWI is a risk factor for ACL injury. 6 The PTSL was smaller in patients with the case group compared with the control group (8.3°± 3.6° vs 11.2°± 4.0°). This finding contrasts with previous studies that reported larger PTSL in ACL-injured patients compared with healthy individuals. A previous case-control study with a larger sample size (N = 94) reported a 5.7-fold increased risk of secondary ACL injury with PTSL ≥10°. 6 While our study used MRI rather than radiographs for evaluation, our smaller case group sample size (n = 32) may have led to underestimation of results. The scarcity of studies comparing PTSL between secondary injury and primary reconstruction groups highlights the need for further research.
We conducted a sensitivity analysis according to sex because of the limited number of eligible cases during patient selection. Both male and female patients exhibited similar trends in the overall population. Furthermore, the OR for the increase in MTSH was notably high (20.65 in female patients). These results suggest that the study may still be robust despite the limited number of cases.
Limitations
The primary limitation of our study is the relatively small sample size in the case group (n = 32). While MRI was necessary for our detailed analysis, this imaging requirement contributed to the reduced number of eligible cases. Additionally, while MRI provides excellent soft tissue visualization, computed tomography scanning might have provided more precise measurement of bony landmarks. Study limitations include the lack of inter- and intrarater reliability testing for our measurements and the potential variability introduced by using MRI studies from multiple institutions with different imaging protocols. Additionally, the limited case group size restricted our ability to include potentially important variables such as graft type, tibial bone tunnel size, and postoperative Tegner activity score in the multivariate analysis.
The use of MRI images from different centers, with potentially varying equipment and protocols, could introduce variability in the measurements. This limitation may affect the consistency of TSH evaluation and should be considered when interpreting the study results. Despite these limitations, the novelty of our study lies in the higher-precision evaluation using MRI after ACLR, focusing on the increase in TSH, calculation of the OR, and achievement of high predictive accuracy based on the AUC. Finally, this study did not include patient-reported outcome measures because of excessive missing data. Because subjective patient evaluations and revisions after ACL are important public health concerns, these areas remain topics for future research.
Conclusion
This study demonstrates a significant association between increased MTSH after ACLR and secondary ACL injury. Using a 1-mm increase in MTSH as the cutoff value, our model showed excellent discriminative ability in predicting secondary ACL injury. For each 1-mm increase in MTSH, the odds of secondary ACL injury were 7.62 times higher. These findings highlight the potential of MTSH changes as a valuable risk assessment tool.
Footnotes
Acknowledgements
The authors are indebted to Prof. Marie Diener-West and Prof. Renan Castillo for their significant contributions and advice on this paper. They also acknowledge their invaluable guidance during Naofumi Hashiguchi's Master of Public Health studies at the Johns Hopkins Bloomberg School of Public Health. Naofumi Hashiguchi, MD, completed this work while he was a Master of Public Health student at the Johns Hopkins Bloomberg School of Public Health.
Final revision submitted March 5, 2025; accepted April 14, 2025.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating.
Ethical approval for this study was obtained from the Ethics Committee of Hiroshima University (No. E-1189).