
Abstract
Background:
Hip arthroscopy effectively treats femoroacetabular impingement (FAI) to preserve joint function and alleviate symptoms. Joint space widths (JSWs) and ratios may predict surgical outcomes, especially in older patients.
Purpose:
To assess the relationship between the preoperative lateral-to-medial (L/M) ratio, the central-to-medial (C/M) ratio, and postoperative functional scores following arthroscopic treatment for FAI in patients aged ≥35 years.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients who had primary hip arthroscopy for FAI between February 5, 2013, and June 1, 2022, with a minimum 2-year follow-up, were included and categorized into 2 age groups (≥35 years and <35 years). Radiographic measurements of JSW on plain anteroposterior pelvic radiographs were used to calculate L/M and C/M ratios. Patient-reported outcomes included the modified Harris Hip Score (mHHS) and visual analog scale for pain. Statistical analysis included chi-square, Mann-Whitney U, and Wilcoxon tests to compare categorical and continuous variables. The receiver operating characteristic (ROC) curve and area under the curve (AUC) assessed threshold values for L/M and C/M ratios predicting the Patient Acceptable Symptom State (PASS) for mHHS at 2 years.
Results:
A total of 110 patients (114 hips) were identified, comprising 56 hips from the older group (age ≥35 years) and 58 hips from the younger group (age <35 years). The ROC curve for preoperative C/M effectively distinguished between patients who achieved and did not achieve a second-year PASS value, with an AUC of 0.70 in older patients. Older patients, compared with younger, demonstrated lower postoperative mHHS (89 ± 10 vs 94 ± 8; P = .01) but similar rates of PASS achievement (75% vs 88%; P = .07). The C/M ratio was a significant predictor of functional outcomes in patients aged ≥35. Patients with a preoperative C/M ratio ≥1.08 achieved significantly better outcomes. No significant predictive value was found for L/M ratios in older patients or for L/M and C/M ratios in younger patients.
Conclusion:
Our study demonstrated that the central JSW is a sensitive prognostic indicator in older patients undergoing primary hip arthroscopy. A preoperative C/M ratio ≥1.08 correlates with higher rates of achieving PASS. Identifying preoperative predictors, such as the C/M JSW ratio, assists surgeons in determining patients (≥35 years) who are more likely to benefit from hip arthroscopy.
Keywords
Hip arthroscopy is a successful treatment for the femoral-based deformity seen in cam impingement and for acetabular-based abnormalities associated with pincer-type impingement. 10 In recent decades, the utility of hip arthroscopy has expanded significantly and has proven to be effective. The purpose of this procedure is to preserve the joint and alleviate associated symptoms.7,16,21 Despite advancements in surgical technique, older age has been identified as a negative predictor of outcomes at 2 and 5 years after primary hip arthroscopy.3,4,6,14 Many studies indicate comparable functional outcomes between younger and older cohorts; however, total hip arthroplasty conversion rates are notably higher among older individuals.5,6
The width of the joint space measured on pelvic radiographs has been associated with cartilage damage, joint survival rates, and the duration free from total hip arthroplasty after primary hip arthroscopy.24,32 A more recent study reported the lateral joint space to medial joint space ratio measured at the lateral and medial edges of the sourcil in pelvic radiographs as the most significant factor in predicting survivorship. They tried to explain this by stating that the lateral joint space represents the area where the labrum is more susceptible to injury in femoroacetabular impingement (FAI). 23 In a separate study, damage to the central acetabular cartilage showed lower survival rates compared with damage to the lateral joint cartilage, likely indicating a more advanced stage of the disease. 32
The purpose of this study was to clarify the relationship between the lateral-to-medial (L/M) joint space and central-to-medial (C/M) joint space width (JSW) ratios and functional scores. The hypothesis was that both the L/M and the C/M ratios are crucial for identifying clinical significance, with higher ratios correlating with better functional scores. Furthermore, our secondary hypothesis is that these ratios are considered more significant for individuals aged ≥35 years than for those <35 years.
Methods
This study included 110 patients (114 hips) who underwent hip arthroscopy for FAI between February 5, 2013, and June 1, 2022, and had 2 years of follow-up. Data were prospectively collected and retrospectively reviewed in all patients. Patients were stratified into group 1 (≥35 years of age) and group 2 (<35 years of age). Ethical approval was obtained from the Dokuz Eylul University.
FAI was diagnosed based on clinical symptoms and radiographic findings (alpha angle >55° for cam deformity using the Dunn 45° view13,19 and lateral center-edge angle [LCEA] ≥40°).15,30 Inclusion criteria were patients who experienced persistent hip pain lasting >3 months, had no intra-articular pathologies, such as tumors, stress fractures, and avascular necrosis, and had not responded to nonoperative treatment such as physical therapy and pain medication. However, we propose direct surgical treatment for patients with delayed outpatient presentation, defined as seeking medical attention >3 months after symptom onset despite prior use of analgesic medications and engagement in physical therapy exercises without satisfactory clinical improvement. Patients were excluded if they had avascular necrosis, advanced-level hip osteoarthritis (Tönnis grade >1), 28 any previous ipsilateral hip surgery, revision hip arthroscopy, incomplete radiographs, or hip dysplasia (LCEA <25°) 31 or could not be reached for follow-up.
Surgical Procedure
The patient was placed supine on a hip arthroscopy–specific traction table to obtain appropriate hip distraction against a well-padded perineal post. A standard anterolateral and anterior portal were established with fluoroscopic and arthroscopic guidance. Additionally, a distal anterolateral portal was created and used for suture anchor placement. A horizontal interportal capsulotomy was used to improve visualization and access to the central compartment. A 4.5-mm arthroscopic bur was used to perform acetabuloplasty. Degenerative labral tears, or those with multiple cleavage planes, were considered irreparable, and unstable flaps were selectively debrided. Additionally, focal chondral lesions observed during arthroscopy, particularly in patients with lower Tönnis grades, were treated with selective chondral debridement to remove unstable cartilage and promote a more congruent articular surface. Tears that involved the base of the labrum with chondrolabral disruption were repaired using 1 to 3 suture anchors (Doratek). Traction was then released, the peripheral compartment was entered, and decompression of the cam deformity was performed and confirmed by intraoperative fluoroscopy and arthroscopic dynamic examination. The capsule was routinely left open at the end of the procedure, and capsular repair was not performed in the cases included in this study.
Rehabilitation
All patients were instructed to use crutches to limit weightbearing for 2 weeks. Daily passive range of motion exercises began on the first postoperative day. At 3 weeks, active range of motion and full weightbearing commenced. After 6 weeks, strengthening and light treadmill walking began. For the first 4 weeks, daily oral anti-inflammatory medication was prescribed.
We collected data on continuous and categorical demographic and clinical variables, including age, sex, type of labral treatment, and duration of symptoms before surgery.
Radiological and Clinical Assessment
Radiographs were obtained and evaluated in all patients using the anteroposterior supine pelvic radiograph and 45° Dunn radiograph. LCEA was measured using the method described by Wiberg 30 at the pelvic radiograph. The alpha angle (α) was measured using preoperative and early postoperative Dunn 45° views.13,19
Joint space measurements were performed on anteroposterior supine pelvic radiographs. The sourcil, the sclerotic weightbearing portion of the acetabulum, was used as the reference for joint space measurements. The medial joint width was measured at the most medial border of the sourcil, while the lateral joint width was measured at the most lateral border of the sourcil. For the central JSW, a horizontal line connecting the centers of both femoral heads was used as a reference. The central JSW measurement was taken at the intersection of this horizontal line and a perpendicular vertical line extending from the center of the femoral head to the acetabulum (Figure 1). 24

Anteroposterior radiograph of the right hip showing joint space width measurements. The medial (yellow asterisk), central (pink asterisk), and lateral joint space (blue asterisk) measurements.
This study did not include a direct assessment or grading of chondrolabral lesion severity; instead, we evaluated indirect indicators such as Tönnis grade and JSW measurements.
Patient-reported outcomes, which included modified Harris Hip Score (mHHS) 27 and visual analog scale for pain (Pain VAS) were collected by direct contact with the patients. Reported Patient Acceptable Symptom State (PASS) values ≤5 years after hip arthroscopy for FAI are 83.6 for the mHHS.17,29 The minimal clinically important difference was not used because patients had been assessed at different time intervals.
Two orthopaedic consultants (S.A. and Ö.A.) performed radiographic assessments. Intraclass correlation coefficient (ICC) values of lateral joint width, central JSW, and medial joint width were calculated for interrater and intrarater reliability. For intrarater reliability, each observer repeated the measurements with a 15-day interval between sessions. An ICC of >0.80 indicates excellent reliability; 0.61 to 0.80 indicates substantial reliability; 0.41 to 0.60 indicates moderate reliability; 0.21 to 0.40 indicates fair reliability; and ≤0.20 indicates poor reliability. 9
Statistical Analysis
Data analysis was performed using SPSS Version 24 for Windows (SPSS Statistics; IBM Corp). Values of P < .05 were considered statistically significant. The effects of dichotomous or categorical variables were analyzed using the Fisher exact or chi-square test. Preoperative to postoperative changes in the variables were assessed using the Wilcoxon test. Continuous variables were analyzed using the Mann-Whitney U test.
The receiver operating characteristic (ROC) curve and the area under the curve (AUC) were analyzed to further determine discriminatory threshold values for preoperative L/M or C/M in relation to the frequency of reaching 2-year PASS values for the mHHS. An AUC of 0.5 suggests no discrimination, 0.7 to 0.8 is considered acceptable, and 0.8 to 0.9 is considered excellent. 12
Results
A total of 110 patients (114 hips) were included in this analysis. There were 56 hips in group 1 (age ≥35 years) and 58 hips in group 2 (age <35 years). Patient characteristics for both groups are shown in Table 1. There was no difference between groups except for age (P > .05).
Patient Characteristics a

Data are presented as mean ± SD (95% CI) unless otherwise indicated.
Radiological parameters and functional scores are presented in Table 2. The degree of osteoarthritis was higher in group 1 (more Tönnis grade 1 hips; P = .02). Although postoperative mHHS scores were lower in group 1 (P = .01), the frequency of reaching PASS values did not differ between groups (P = .07).
Radiological Parameters and Functional Results a

Data presented as mean ± SD or n (%). Bolded P values indicate statistical significance p < .05. LCEA, lateral center-edge angle; mHHS, modified Harris Hip Score; PASS, Patient Acceptable Symptom State; postop, postoperative; preop, preoperative; VAS, visual analog scale.
In the older patient group, the ROC curve for preoperative C/M demonstrated acceptable discrimination between those who reached the PASS value and those who did not, with an AUC of 0.70 (Figure 2). The Youden index identified a threshold of 1.08 for C/M. Patients with a preoperative C/M ≥1.08 achieved the PASS value at a notably higher rate than those with a preoperative C/M <1.08 (P = .03; sensitivity, 0.66; specificity, 0.71) (Figure 3).

Receiver operating characteristic (ROC) curve for preoperative central-to-medial Patient Acceptable Symptom State at the older patient group (area under the curve, 0.7; P = .03).
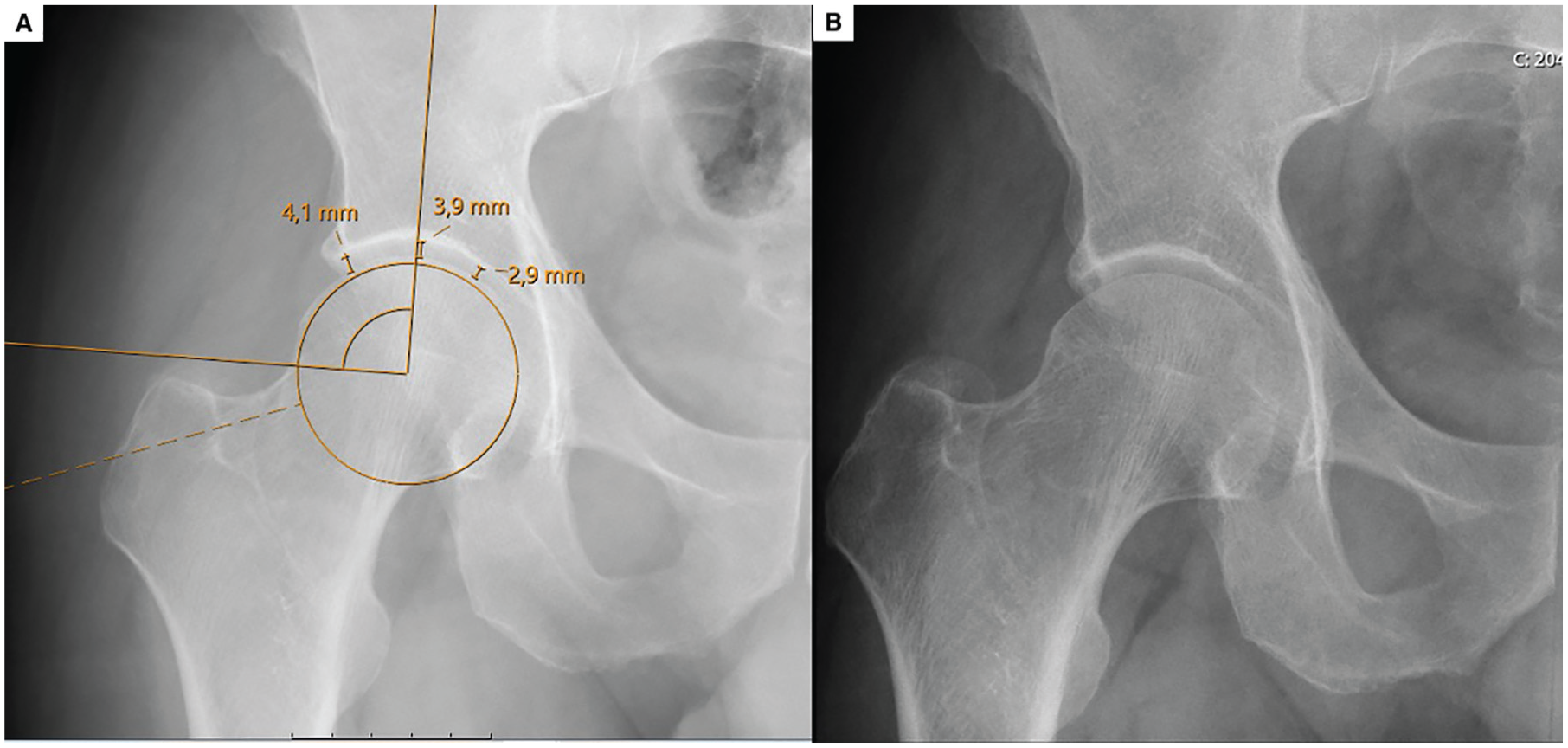
(A) Preoperative and (B) postoperative radiographs of a 48-year-old patient who underwent surgery because of right hip pain and was followed for 65 months. The central-to-medial ratio was assessed as >1.08 and measured as 1.34. Postoperatively, the patient achieved Patient Acceptable Symptom State positivity, with the modified Harris Hip Score improving from 41 preoperatively to 89 postoperatively.
There was no acceptable discrimination for L/M in the older group and for both L/M, and C/M in the younger group (P > .05). Preoperative lateral JSW (intrarater, 0.95; interrater, 0.87), medial JSW (intrarater, 0.93; interrater, 0.87), and central JSW (intrarater, 0.97; interrater, 0.92) had excellent intra- and interrater reliabilities.
Discussion
The main finding of this study was that preoperative JSW, particularly the central joint space, determines the prognosis of older patients treated with hip arthroscopy. In patients aged 35 years or older, the ROC curve for the preoperative C/M demonstrated acceptable discrimination between those who achieved the PASS value and those who did not, with an AUC of 0.70. Patients with a preoperative C/M ≥1.08 achieved the PASS value at a significantly higher rate compared with those with a C/M <1.08 (P = .03; sensitivity, 0.66; specificity, 0.71).
In the literature, a joint space margin of 2 mm has been reported to be associated with the prognosis and occurrence of cartilage lesions. A joint space of <2 mm has been associated with an earlier conversion to total hip arthroplasty, resulting in lower patient-reported outcomes and presenting relative contraindications for hip arthroscopy.11,20
Recently, Kraeutler et al 8 tried to standardize the JSW and reported no difference between medial and lateral joint space or at symptomatic and asymptomatic hips, with a range of 3.9 to 4.5 mm. Later studies report a cutoff value for JSW as high as 4 mm, with lower values resulting in worse functional outcomes and a higher frequency of total hip arthroplasty conversions.2,22,32
Another study, however, found no link between JSW and observed cartilage damage in the joint. The researchers concluded that a narrower joint space might be an anatomic variation in individuals with mild or absent osteoarthritis. Additionally, it was noted that if the lateral joint space is narrower relative to the medial joint space, it could suggest damage to the acetabular cartilage. 24 A subsequent study by the same group, testing their previous hypothesis, found that the L/M JSW ratio is the most significant predictor of survivorship after hip arthroscopy. 32 They did not analyze the relation of C/M JSW ratio.
Our study did not establish a connection between the L/M JSW ratio and clinical outcomes. One reason could be the presence of calcified labra in patients, which might exhibit narrowing of the lateral joint space before surgery. However, after removing labral calcification, the JSW does not show considerable changes at the medial or central JSW, with the postoperative increase of lateral joint space. 18 Additionally, the central joint space may be a more sensitive prognostic indicator, signifying a more advanced degree of joint damage. 32
Limitations
There are some limitations in our study. First, we utilized only the mHHS and the Pain VAS as patient-reported outcomes, excluding other metrics such as the Hip Outcome Score or International Hip Outcome Tool–12. Additionally, we did not assess the severity of chondrolabral lesions. Nevertheless, we investigated the type of labral treatment and the number of anchors employed, and we evaluated indirect indicators of cartilage damage, including Tönnis grading and JSW measurements.1,25,26 Third, this study involves patients treated by a single surgeon with a small patient group, lacking a control group and adjustments for confounding factors, while conducting a retrospective analysis of prospectively collected data. Finally, the present study did not report the relationship between raw JSW and clinical outcomes; instead, it focused on the ratio of space widths to avoid potential magnification errors.
Conclusion
Our study demonstrated that the central JSW is a sensitive prognostic indicator in older patients undergoing primary hip arthroscopy. A preoperative C/M ratio ≥1.08 correlates with higher rates of achieving the PASS. Identifying preoperative predictors, such as the C/M JSW ratio, assists surgeons in determining patients (≥35 years) who are more likely to benefit from hip arthroscopy.
Footnotes
Final revision submitted April 18, 2025; accepted May 20, 2025.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Dokuz Eylul University Non-Interventional Research Ethics Committee (2024/43-13).