
Abstract
Background:
Medial epicondylar apophyseal avulsion fractures of the distal humerus represent an understudied severe variant of elbow overuse injury in youth throwers.
Purpose:
To characterize medial epicondylar apophyseal avulsion fractures in a population of youth throwers, as well as to describe outcomes after both operative and nonoperative treatment.
Study Design:
Case series; Level of evidence, 4.
Methods:
Skeletally immature athletes with a medial epicondylar apophyseal avulsion fracture sustained during throwing from 2003 to 2017 at a tertiary care pediatric referral center were identified. Exclusion criteria were injuries sustained during nonthrowing events or previous elbow fractures. Patients treated operatively were compared with those treated nonoperatively, and the overall study population was compared with a control group of patients diagnosed with medial epicondylar apophysitis only, with no fracture.
Results:
A total of 50 patients with medial epicondylar avulsion fractures (100% male; 49 baseball pitchers, 1 football quarterback) were identified. These patients had higher body mass index (BMI) than the control group with medial epicondylar apophysitis only. Of the 37 avulsion fracture patients with documentation regarding presence or absence of preoperative symptoms, 31 patients (84%) reported preexisting elbow pain before their acute injury. Of the 12 patients who underwent shoulder exams at presentation, 5 (42%) demonstrated glenohumeral internal rotation deficit (GIRD). Of the total 50 patients, 22 (44%) underwent open reduction and internal fixation (ORIF) with a single cannulated screw, 1 (2%) patient underwent suture-based fixation, and 27 (54%) patients were treated nonoperatively. For each additional millimeter of displacement, the odds of surgical intervention increased by 6.4 times (odds ratio, 6.36; 95% CI, 1.83-22.07; P = .004) when controlling for age and BMI. All patients returned to sports, with no significant difference in recurrent elbow pain between cohorts, although 41% of applicable ORIF patients (9 of 22) underwent secondary screw removal.
Conclusion:
Displaced medial epicondylar apophyseal avulsion fractures in youth throwers may be effectively treated with operative screw fixation, although >40% of patients may require secondary screw removal. Nonoperative treatment may be appropriate for minimally displaced cases. Given that a large majority of patients reported preexisting elbow pain, and a substantial cohort demonstrated GIRD, this severe presentation of Little League elbow may be preventable.
Keywords
As participation in youth sports increases, so too does the incidence of overuse injuries in pediatric athletes.3,5,9,23,31 Among adolescents participating in throwing sports such as baseball, the elbow is a common source of pain after repetitive use.15,16,28 Valgus forces during the late cocking and acceleration phases of throwing place high levels of strain on the apophysis of the medial epicondyle in particular.1,7 With time, overuse can result in a stress injury to the medial epicondylar apophysis, often referred to as “Little League elbow” (LLE). While this term has occasionally been used in the literature to describe alternative conditions in different anatomic elbow locations, LLE most accurately and specifically refers to medial epicondylar apophysitis. 4
The same repetitive traction forces on the medial elbow that lead to apophysitis may also result in an acute avulsion fracture of the medial epicondyle with a single throwing event. Such avulsion fractures may therefore be considered a severe variant of LLE. Importantly, the vast majority of medial epicondylar fractures seen in children do not occur in association with throwing, but rather with traumatic falls onto an outstretched hand. Despite being a common pediatric orthopaedic injury with extensive previous literature, the optimal treatment of displaced medial epicondylar fractures in skeletally immature patients remains controversial. ‖ Some investigators advocate for surgical fixation of even mildly displaced fractures, particularly in youth athletes, while others promote the more historically pursued nonoperative management.12,17,18,26
In the setting of this controversy, few studies have described the unique subset of medial epicondylar avulsion fractures resulting from throwing.26,29 The purpose of the present study was to analyze a cohort of adolescent throwers who had these medial epicondylar avulsion fractures. We sought to better characterize the clinical and radiographic features of the injuries as well as assess outcomes of both operative and nonoperative management.
Methods
Following institutional review board approval, electronic medical records at a tertiary care pediatric hospital were queried to identify all patients diagnosed with a medial epicondylar fracture sustained while throwing between January 1, 2003, and December 31, 2017. Inclusion criteria consisted of skeletal immaturity, age between 8 and 16 years old, and a physician’s diagnosis of a medial epicondylar apophyseal avulsion fracture sustained while throwing. Patients were excluded if injuries occurred during alternative traumatic events, such as a fall onto an outstretched hand, a collision/direct blow, or if the patient had a history of previous elbow fracture that might confound their clinical course or outcome. Clinic notes, radiographic images, and operative reports, when applicable, were reviewed for study variables.
Collected data included patient demographics and athletic data (age, sex, body mass index (BMI), sport played, sport position, injury laterality). In addition, relevant clinical and injury data, such as concomitant fracture or ligamentous injury, presence and duration of elbow symptoms before fracture, pertinent results of any shoulder examinations performed (eg, glenohumeral internal rotation deficit, or GIRD), and ulnar nerve symptoms at the time of injury were collected. Injury radiographs (Figures 1A, B and 2A, B) were reviewed for concomitant injuries and medial epicondylar fracture displacement, which was measured as the maximal distance between the displaced fragment and its origin, as seen on the anteroposterior (AP) view of the elbow, in keeping with previously described methods. 30

Operative treatment. Radiographs at time of injury demonstrating a 7.3-mm displaced medial epicondylar avulsion fracture. Radiographs 12 weeks following open reduction internal fixation showing a healed fracture. (A) Injury AP view; (B) injury medial oblique view; (C) 12-week post-operative AP view; (D) 12-weekpost-operative medial oblique view. AP, anteroposterior.

Nonoperative treatment. Radiographs at time of injury demonstrating a medial epicondylar avulsion fracture with 4.6-mm displacement. Radiographs following 11 weeks of nonoperative management showing a healed fracture. (A) Injury AP view; (B) injury medial oblique view; (C) 11-week post-injury AP view; (D) 11-week post-injury medial oblique view. AP, anteroposterior.
Treatment, including operative versus nonoperative management, and any associated complications, were recorded and surgical details documented. All treatment decisions and surgeries were performed by 1 of 20 different fellowship-trained pediatric orthopaedic surgeons at the study institution.
For patients who underwent operative management, the technique consisted of an open approach to the medial epicondyle, with identification and protection of the ulnar nerve. In all but 1 patient, provisional reduction of the fragment with a guide wire was achieved before internal fixation with a partially threaded, cannulated screw (either 3.5 mm or 4.0 mm in diameter), with or without the addition of a screw washer. The other patient treated operatively underwent suture-based fixation of a partial medial epicondylar fracture fragment that was also attached to the ulnar collateral ligament. Subsequent immobilization in all surgical cases consisted of a temporary cast (median duration 14 days; IQR, 12-19 days) followed by transition to a hinged elbow brace.
Primary nonoperative treatment included cessation of athletic activities and elbow immobilization in a long arm fiberglass cast, hinged elbow brace, or simple sling for a median duration of 32 days (IQR, 26-43 days). All patients in both cohorts were prescribed physical therapy after immobilization for strengthening and range of motion exercises. Follow-up clinical metrics, including duration of follow-up, time to symptom resolution, time to return to sports, and any recurrent elbow pain, were recorded. Recurrent elbow pain related to symptomatic hardware in operatively treated patients or recurrent similar medial epicondylar symptoms in nonoperatively treated patients were recorded. Available follow-up radiographs were assessed for bony union, which was defined as the presence of continuous bony trabeculae to the fragment or bridging peripheral callus (Figures 1C, D and 2C, D).
For added clinical context, relevant patient metrics of this cohort were compared with those for a control group of 267 patients who presented to the study institution and were diagnosed with medial epicondylar apophysitis, or LLE, only. While no patients in this comparison cohort sustained a medial epicondylar apophyseal avulsion fracture, all were also skeletally immature athletes in the same age range who were evaluated during the same defined study window. Comprehensive details of the presentation, treatment, and clinical course of this cohort are described in a separate study. 20
Measures of clinical, radiographic, and surgical characteristics were summarized using descriptive statistics. Median and interquartile range were utilized to account for any non-normally distributed data. Formal normality testing was not performed. Fisher’s exact tests, Mann-Whitney U tests or Wilcoxon signed-rank tests were used, as appropriate, for comparative analysis. Multivariable logistic regression analysis was used to determine the effect of avulsion displacement on the likelihood of surgical intervention controlling for patient characteristics including age at presentation and BMI. The adjusted odds ratio (OR) for avulsion displacement was estimated along with a 95% CI. All tests were 2-sided and a P value < .05 was considered statistically significant. Statistical analysis was conducted using RStudio (Version 2024.12.0+467; Posit Software, PBC).
Results
A total of 50 patients, all of whom were male, met study criteria. Of these, 45 (90%) patients were right-hand dominant in sports, with 49 (98%) patients playing pitcher in baseball and 1 (2%) playing quarterback in football. Median BMI was 21.3 kg/m2 (IQR, 19.3-23.2 kg/m2) and median age at presentation was 13.1 years (range, 8-16 years). When compared with the control cohort diagnosed with medial epicondylar apophysitis only (median BMI, 19.2 kg/m2; median age, 12.8 years), the current avulsion fracture population demonstrated significantly greater BMI (P = .004) but was not significantly older (Table 1).
Medial Epicondylar Apophysitis Only Versus Avulsion Fracture a
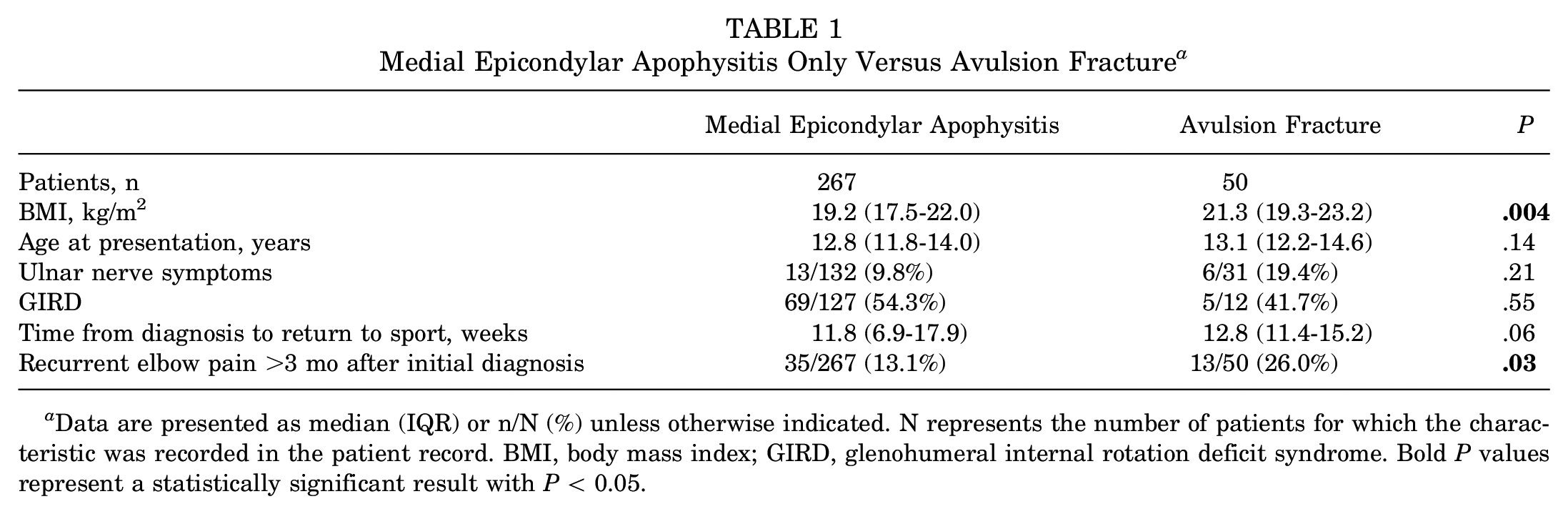
Data are presented as median (IQR) or n/N (%) unless otherwise indicated. N represents the number of patients for which the characteristic was recorded in the patient record. BMI, body mass index; GIRD, glenohumeral internal rotation deficit syndrome. Bold P values represent a statistically significant result with P < 0.05.
The median time of presentation after injury was 3.5 days (IQR, 1.0-11.0 days). Of 37 patients with documentation of having been questioned regarding preinjury medial elbow discomfort, 31 (84%; 62% overall) patients endorsed preexisting medial elbow pain before their acute injury, while 6 (16%; 12% overall) denied pain before the inciting throw. One avulsion fracture patient had been diagnosed with medial epicondylar apophysitis during a clinic visit at the study institution 19 weeks prior, after which the patient had been noncompliant with recommended follow-up and treatment recommendations, with intermittent pain up to the time of the avulsion fracture. Six of 31 patients (19%) with documentation of having been questioned regarding ulnar nerve symptomatology reported the presence of ulnar nerve symptoms. GIRD syndrome was diagnosed in 5 of the 12 (42%) patients with a documented shoulder examination.
All 50 patients underwent radiographic assessment of the affected elbow, with 9 patients (18%) also undergoing contralateral elbow radiographic assessment for comparison purposes. Thirteen patients (26%) received a magnetic resonance imaging (MRI) scan of the affected elbow, to confirm the diagnosis of fracture in the setting of minimal or mild apophyseal displacement. Five patients received both MRI of the affected elbow and contralateral plain radiographs. Median fracture displacement of the overall cohort, as measured on AP radiographs of the elbow, was 4.2 mm (IQR, 2.8-5.1 mm; range, 1.4-7.7 mm).
A total of 23 patients (46%) were treated with open reduction internal fixation (ORIF) of the medial epicondylar fracture at a median time from presentation of 4 days (IQR, 2-6 days). In 10 ORIF patients (43%) a washer was used in association with the single screw, while 13 patients (57%) received no washer. One patient underwent only suture-based fixation of a partial medial epicondylar fragment attached to the ulnar collateral ligament (UCL) by passing the UCL/fragment sutures proximally through 2 drill holes in the medial column, tying the sutures over a bone bridge. Two patients (9%; 4% overall) underwent concomitant procedures. One patient underwent screw fixation of the medial epicondyle and concomitant suture anchor–based repair of a partial tear of the UCL. One patient underwent screw fixation of the medial epicondyle and concomitant single-screw fixation of an associated olecranon apophysitis, diagnosed based on gross radiographic apophyseal widening of the olecranon and correlating with the patient’s report of a 1-month history of both medial and posterior elbow pain with throwing before the discreet traumatic throwing event.
Of the total cohort, 27 patients (54%) were treated nonoperatively with immobilization (cast, n = 9; hinged elbow brace, n = 14; sling, n = 4). Patients treated operatively had a median fracture displacement of 5.0 mm, while those treated nonoperatively had a median displacement of 3.0 mm (P < .001) (Figure 3). Multivariable analysis determined that for each additional millimeter of displacement, the odds of surgical intervention increased by 6.4 times (OR, 6.36; 95% CI, 1.83-22.07; P = .004) when controlling for age and BMI. Additionally, though documentation was limited, patients who had surgery were more likely to have had GIRD at the time of presentation (P = .027).

Initial fracture displacement for patients treated operatively and nonoperatively.
Median postoperative follow-up for patients in the operative cohort was 22 months (IQR, 8-47 months). In the subset of 22 patients who underwent radiographic assessment ≥4 weeks after surgery, bony union was present in 19 of 22 (86%) patients. Among the 22 operative patients for whom documentation was available regarding return to sports, all 22 (100%) were able to return to throwing sports at a median of 13 weeks after surgery (IQR, 12-19 weeks; range, 10-38 weeks). Two patients (9%; 4% overall) reported residual postoperative ulnar nerve symptoms, one of whom underwent a subsequent operation for ulnar nerve decompression and transposition 5 days after ORIF. Nine operative patients (41%; 18% overall), all of whom had been able to successfully return to sports, underwent secondary surgery for implant removal due to implant-related pain or overlying soft tissue irritation at a median of 12 months (IQR, 7-14 months; range, 3-36 months) after screw fixation surgery. There was no significant difference in the rate of implant removal between patients in whom a washer was utilized in association with screw fixation versus those in whom a washer was not used (40% vs 38%; P≥.99). Seven of the 9 patients had adequate documentation regarding returning to sports again after the implant removal surgery, and all successfully returned to sports. However, one of these patients reported recurrent elbow pain 32 months after the index surgery and 20 months after implant removal.
Median follow-up time for the 27 patients treated nonoperatively was 28.8 months (IQR, 11-43 months; range, 1-92 months). Follow-up radiographs were taken irregularly, with 17 patients receiving radiographs ≥4 weeks after initial diagnosis. Six of these patients (35%) showed clear evidence of bony union, while the rest were not followed radiographically until confirmation of union (Table 2). Among the 22 nonoperative patients for whom documentation was available regarding return to sports, all 22 (100%) were able to return to sports at a median of 13 weeks (IQR, 9-11 weeks; range, 4-51 weeks ) after diagnosis. Four patients of the 27 (15%) reported recurrent elbow pain at a median of 23 months (IQR, 20-24 months; range, 11-26 months) after diagnosis. Although this percentage was lower than the rate of recurrent elbow pain necessitating implant removal in the operative cohort, this difference was not statistically significant (P = .06). None of the 27 patients who were initially treated nonoperatively underwent operative intervention at a later date.
Comparison of Operative Versus Nonoperative Cohorts a

Data are presented as median (IQR) or n/N (%). N represents the number of patients for which the characteristic was recorded in the patient record. BMI, body mass index; GIRD, glenohumeral internal rotation deficit syndrome. Bold P values represent a statistically significant result with P < 0.05.
Rate reflects subpopulation with adequate imaging >4 weeks after diagnosis or surgery, rather than true rates of bony union.
Discussion
Pure avulsion-type medial epicondylar fractures in children represent a unique and understudied variation of medial epicondylar apophyseal fractures. These fractures, which typically occur with falls onto an outstretched hand, are common, accounting for 12% of elbow fractures in skeletally immature patients. 33 However, despite this frequency, the optimal treatment remains a subject of considerable controversy with even less known about the subset suffered during a single traumatic throw.
Medial epicondylar fractures in children with <2 mm of displacement have generally been treated nonoperatively, 33 with ongoing debate regarding the degree of displacement that warrants surgical fixation and the subpopulation of children in whom surgery may be most appropriate.10,13,21 Furthermore, there is a wide spectrum in reported rates of delayed union or nonunion with nonoperative treatment, based on displacement or other factors. 24 Some authors have reported favorable outcomes after nonoperative treatment of medial epicondylar fractures displaced appreciably >2 mm.6,8,26 Farsetti et al 12 found no difference in functional range of motion and nonunion rates between operative and nonoperative management for fractures with displacement between 5 mm and 15 mm. Similarly, Stepanovich et al 32 found no difference in patient satisfaction or elbow function scores between operatively and nonoperatively treated fractures. Hughes et al 22 assessed treatment preferences of 13 pediatric orthopaedic surgeons via 60 case vignettes of medial epicondylar fractures. These authors found significant variation in treatment decisions, and the only attributes to significantly influence a surgeon’s decision to perform surgery were elbow dislocation and fracture displacement.
Pure avulsion-type fractures suffered during a single traumatic throw represent a uniquely and minimally studied variation of traumatic medial epicondylar fractures in children. Intuitively, this injury pattern is more likely in the setting of underlying apophysitis of the medial epicondyle, or LLE. However, the degree to which such an avulsion fracture can occur in the absence of medial epicondylar apophysitis has not been documented.
As both the static and the dynamic medial stabilizers of the elbow may remain attached to the medial epicondylar fracture fragment, some have advocated operative fixation of fractures with any degree of displacement in throwing athletes.2,27 One report of 8 skeletally immature baseball players who sustained medial epicondylar avulsion fractures during throwing also presented a potential treatment algorithm, in which fractures with <5 mm of displacement on AP radiographs underwent nonoperative management, while those with >5 mm of displacement underwent ORIF. 29 Similar to this previous study, the current series demonstrated favorable return to sports rates among both operatively and nonoperatively treated patients. While the operative cohort had significantly greater displacement than the nonoperative cohort, this difference of only 2 mm suggests substantial overlap between the cohorts in terms of displacement, which may preclude definitive recommendations regarding surgical indications based specifically on displacement. While approximately half of our operative cohort demonstrated displacement <5 mm, and therefore might have been successfully treated nonoperatively, notably these patients had a successful postoperative course overall. Moreover, 15% of the nonoperative cohort reported recurrent elbow pain after returning to sports, although in some instances this arose after skeletal maturity. Given the overall favorable clinical outcome and return to sports in both groups, it seems clear that in the setting of minimal displacement, nonoperative management of medial epicondylar avulsion fractures may be a viable option after careful shared decision making with families, even in pitchers.
In the setting of displaced fractures, operative treatment was effective in the current cohort. While the precise indications or rationale for surgery were not explicitly stated in all cases in this retrospective study, optimization of bony healing may be more important in the athletic subpopulation of throwers than the overall population of children sustaining traumatic medial epicondylar fractures. Importantly, medial elbow symptoms, which can arise secondary to fibrous nonunion after injury, have been postulated to negatively affect youth baseball performance, due to impaired integrity of the medial stabilizers to the bony medial column of the distal humerus. These patients may not experience deficits in their activities of daily living with a fibrous nonunion, but persistent pain, subjective instability, or decreased velocity of throwing have been reported in high-use patients.14,25 Importantly, radiographic follow-up to bony union was not always performed in the present study, thus the proportion of patients who went on to fibrous nonunion remains unclear. These potential athletic consequences of nonunion among nonoperatively treated patients should be considered by surgeons and families, especially in high-level pitchers, even in the setting of favorable outcomes for nonoperatively treated patients, including ability to return to sport. Furthermore, because painful or irritating implants may be common after ORIF, particularly in children, it is also important to inform families that the likelihood of a secondary surgery, based on the current series, may be >40% of cases. The median time of such secondary procedures was approximately 1 year postoperatively, suggesting that these athletes were able to return for ≥1 athletic season after ORIF, so the implant-related symptoms may be mild, with only 1 instance of persistent elbow symptoms after removal surgery.
It is also important to put this cohort of 50 patients into perspective within the larger national and international epidemiologic phenomenon of youth sports injuries. As youth sports participation continues to rise, the incidence of overuse injuries of the elbow will also likely increase. The current study demonstrated that throwing-related medial epicondylar apophyseal avulsion fractures likely represent a subset of the larger pool of LLE patients, which is the most common elbow overuse condition in pediatric athletes. Given that 84% of patients questioned described elbow pain preceding the single throw that led to their injury, most are likely to have had medial epicondylar apophysitis that had not been formally diagnosed, with the injury representing an acute consequence of longstanding stress. Previous studies have reported radiographic changes, such as medial epicondylar apophyseal widening, in as many as 60% of young baseball players.15,16,25 While radiographic findings and chronic elbow pain have been reported in baseball players of all positions, all but 1 of the patients identified in our study were pitchers. This suggests that higher valgus forces may lead to acute avulsion injuries in those subject to the greatest level of elbow stress, such as pitchers. Therefore, we believe that many of these medial epicondylar avulsion injures are preventable with improved awareness, adherence to pitching guidelines, and careful symptom monitoring in those identified with pain.
In conjunction with proper attention to pitching recommendations, identifying other specific risk factors will help facilitate injury prevention. Our results suggest that patients suffering medial epicondylar fracture during throwing may have higher BMIs than counterparts who have medial epicondylar apophysitis but do not sustain these fractures. Thus, the fracture cohort represents athletes who are bigger and who may impart higher degrees of strain on elbows through higher velocity throws, likely placing them at increased risk of fracture. Importantly, although only a quarter of patients had a documented physical examination of the shoulder, a significant proportion of study patients had underlying shoulder dysfunction in the form of GIRD. Just as previous studies have shown surprisingly high rates of elbow pain in those with ‘Little League shoulder’, 19 the current study underscores that the same shoulder-based risk factors, which may disrupt normal throwing mechanics, may be present in this severe variant of LLE. Thus, proper attention to the entire kinetic chain may help to mitigate overuse injuries in any part of the upper extremity.
Limitations
The current study has several limitations. As a retrospective study, it is inherently limited by incompleteness of clinical documentation within the medical record. Furthermore, as a study from a single institution, the findings may have limited generalizability for a sport with regional trends. Moreover, without a treatment algorithm, treatment decisions may reflect institutional biases for a condition with known controversy. Additional study in the form of prospective, multicenter trials may provide more definitive insights into outcomes after different management options. Prospective studies can also provide a more complete characterization of clinical history, sport intensity, and radiographic and long-term functional data among this athletic population. High variability of radiographic follow-up in our patient population also prevents us from making definitive conclusions regarding presence and time to bony union. Next, radiographic measurements of fracture displacement have variable levels of accuracy and reliability,11,30 although such measurements continue to influence clinical decision making. AP radiograph views were used in this study, as internal oblique views were not consistently available. Improvements in radiographic technique or the use of advanced imaging modalities may be helpful in better characterizing fracture patterns and anatomy. Combined with functional assessments of elbow instability, more clinically relevant assessments of fractures may be developed.
Conclusion
Displaced medial epicondylar apophyseal avulsion fractures in youth throwers may be effectively treated with ORIF, although >40% of patients may require secondary implant removal. Nonoperative treatment appears to be appropriate for minimally displaced cases. In our study cohort, 84% reported preexisting elbow pain, suggesting that this severe presentation of medial epicondylar apophysitis (LLE) may be preventable. Of patients undergoing shoulder exams at the time of injury, 42% demonstrated underlying GIRD syndrome, which may be an underappreciated risk factor for youth elbow overuse phenomena.
Footnotes
Final revision submitted April 24, 2025; accepted May 19, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.S.B. is a board member of the Pediatric Orthopaedic Society of North America. Y.-M. Y. is a consultant for Smith & Nephew and OrthoPediatrics and an editorial board member of the American Journal of Sports Medicine. B.E.H. is a consultant for Imagen Technologies Inc and an educational consultant for Arthrex Inc and Kairos Surgical, owns stock in Imagen Technologies Inc, has received fees for education from Arthrex Inc and Kairos Surgical, receives royalties from Springer Science & Business Media, has been a member of the board of directors of Pediatric Research in Sports Medicine, and has been a committee member and committee chair of the Pediatric Orthopaedic Society of North America. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Boston Children’s Hospital (No. IRB-P00033103).