
Abstract
Background:
Little League elbow, including humeral epicondylitis and osteochondritis dissecans, is a severe throwing injury in school-aged pitchers. Recent rule revisions have been implemented, and thus, prevention awareness may have increased.
Purpose:
To compare the incidence of elbow injury in 2011 from a previous study with that in 2021 and examine changes in the incidence and characteristics of players with elbow injuries.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A survey based on the 2011 survey was conducted from September 1 to December 31, 2021, among 4060 third- to sixth-grade Little League players belonging to 203 teams in Kyoto, Japan. This survey included a 23-item checklist on physical condition and injury. The participants were classified into 2 groups according to the presence or absence of an elbow injury in the dominant arm during the season. The Wilcoxon rank-sum test was conducted to compare differences in basic information between the 2 groups. We also compared the differences in the 23 checklist items between the 2 groups using the chi-square or Fisher exact probability test.
Results:
Overall, 98 teams (1335 players; age range, 8-12 years) returned the questionnaires (collection rate, 32.9%). The final analysis population (excluding incomplete questionnaires) was 678 (mean age, 10.6 ± 1.1 years). Elbow injuries accounted for 30.7% of all injury sites in the players. Overall, 61 players (9.0%) reported elbow injuries in 2021 compared with 19.1% of the players in the 2011 survey (P < .01) A significantly higher percentage of players with elbow injuries had elbow pain in extension (item 2 on the survey checklist, P < .001) and flexion (item 4, P < .0024), were regular players (item 5, P = .0288), played baseball under fatigue (item 8, P = .0028), and had lower and upper limb inflexibility (item 17, P = .0379; item 18, P = .0146; and item 22, P = .0085).
Conclusion:
Study findings indicated that the incidence of elbow injuries has decreased significantly over the past 10 years, although the elbow joint still accounted for almost one-third of all injuries in Japanese youth baseball players.
Baseball is one of the most popular sports in Japan, with approximately 10,000 youth baseball teams for elementary school children. 9 Baseball-related throwing injuries occur frequently in schoolchildren throughout Japan. 12 Among these, Little League elbow, including humeral epicondylitis and osteochondritis dissecans, is among the most severe throwing injuries that reportedly occur in 20% to 40% of school-aged pitchers.12,15-18 A survey of Little League baseball players in Japan revealed that the highest percentage of players experienced pain in the elbow joint compared with the other parts of the body (elbow, 24.8%; shoulder, 19.3%; ankle, 18.7%; heel, 12.4%; knee,10.5%). 1 The number of cases requiring surgery due to throwing injuries in juveniles is increasing, and early prevention is needed.5,6,12
Numerous studies have been conducted to investigate the actual status of throwing injuries and identify risk and predictive factors in Little Leaguers.2,3,7,15,17,23 Factors that have been reported to increase the risk of throwing injuries include throwing curveballs, sliders, and other breaking pitches;15,17 an increase in the number of pitches thrown;3,15,17 decreased shoulder joint range of motion (ROM); 23 and decreased shoulder joint muscle strength. 2 Among these risk factors, measures have been introduced to prevent disorders related to the number of pitches thrown. In 2011, the Japan Rubber Baseball Association adopted a throwing limit for the first time, which allowed pitchers to pitch only 1 game per day. 10 In the following year, the rule was changed to limit pitches to 7 innings per day, and a more detailed limit of 70 pitches per day is currently implemented. 10 The Japan Boys League also adopted a throwing limit allowing pitchers only 70 pitches per day, and the baseball world, in general, is implementing measures to prevent injury through throwing restrictions. 8 We searched studies on prevention of baseball throwing injuries in which the participants were aged between 6 and 18 years using the PubMed database on November 10, 2022. Approximately 84% of all studies were conducted after 2011, which means that there is a growing awareness of injury prevention during this decade.
In 2011, our group conducted a survey on the occurrence of elbow injury among Little League players in Kyoto, Japan. 26 When throwing restrictions were first introduced, the incidence of elbow injury was 19.1%. 26 In addition, athletes with elbow joint disorders are reportedly taller and have a greater increase in stature over 12 months. 26 Compared with 2011, the incidence of elbow injury may have decreased with the increased awareness of the prevention of throwing injuries in the past decade. In this study, we aimed to compare the incidence of elbow injury between 2011 and 2021 and examine changes in incidence and the characteristics of players with elbow injury. It was hypothesized that the incidence of elbow injury will have decreased with the increased awareness of throwing injury prevention throughout the baseball community, including coaches and players.
Methods
For this cross-sectional study, we created a paper-based questionnaire to identify any injuries during the baseball season among third- to sixth-grade Little League players. Then, we distributed the questionnaire to 4060 players belonging to 203 teams in Kyoto (the same area as in our 2011 survey) from September 1 to December 31, 2021. 26 Players with injuries or pain arising from nonbaseball activity were excluded. Because the participants were minors, the purpose and methods of this study were explained in detail to their parents, both orally and in writing, and their consent was obtained. Players and parents were asked to complete the questionnaire together to obtain more reliable responses. After completion of the questionnaire, parents were asked to check the contents and mail the forms to the university. The university’s ethics committee approved the study protocol.
The demographic and developmental factors studied were age, height, weight, height growth, and weight gain over the past 12 months; hours of sleep per night; and occurrence of elbow injury during the season. Height and weight gain were determined based on annual measurements recorded at each elementary school by the Japanese educational system. In addition, only self-reported episodes of elbow joint pain during throwing were included in the analysis. In this study, elbow injury was defined as elbow joint pain in the dominant arm that was perceived during the season. “Season” refers to the period of team activity in 2021 (January through the offseason months).
Study Questionnaire and Checklist Items
A questionnaire based on the one used in our 2015 study was developed, 25 with additional checklist items to estimate factors associated with elbow injury occurrence. The current questionnaire was developed by a group consisting of an orthopaedic surgeon (T.A.) and 3 physical therapists (T.M., C.K., and M.O.) in accordance with the Delphi method and after critical discussions between uninvolved physical therapists and youth baseball coaches.
Basic information was recorded in the questionnaire, including age, height, weight, height growth, weight gain over the past 12 months, hours of sleep per night, and medical history. Information on baseball, including years of baseball experience, position, dominant hand, throwing style (overthrow, three-quarter throw, side throw, or underthrow), number of practice days, and self-care, was also collected. Regarding position, participants were classified as fielders, pitchers, catchers, or pitchers or catchers.
To assess overall injuries during the season, the respondents were asked about the injury site, injury type, cause of the injury, painful movements/phase of pain felt, and duration of pain. Respondents selected from among the following injury sites: shoulder joint, elbow joint, wrist, finger, hip joint, knee joint, ankle joint, lower back, anterior thigh, posterior thigh, or other body area. If the same person had 2 or more impairments in the same area, the impairment with the greatest severity was selected.
The condition of the elbow joint of the participants was assessed using a 23-item checklist (Table 1). The following 4 risk areas for elbow injury were evaluated: (1) condition of the elbow joint of the dominant arm, (2) information on game performance and practice, (3) throwing form, and (4) flexibility. The checklist items were based on 2 criteria from a checklist used in a fact-finding survey conducted in 2013, 25 as follows: (1) whether they have been reported as risk factors for throwing-related elbow joint injury and (2) whether they are sufficiently reliable to be assessed easily by coaches and parents. To help parents without medical knowledge to understand the questions, we used photographs with checklist items 13 to 23 to explain the evaluation methods for throwing form and flexibility (see Supplemental Material, available separately). We did not directly measure ROM or muscle flexibility but adopted a simple test that the participants could use for self-evaluation (checklist items 17-23).
Each checklist item was answered by selecting either yes or no. Responses were scored as 0 or 1, with 1 indicating a higher risk of elbow injury.
The 23-Item Study Checklist for Evaluating Elbow Condition a

ROM, range of motion
Yes/no answers that correspond to 1 indicate a higher risk of elbow injury.
Accompanying photographs for these checklist items provided as Supplemental Material.
Statistical Analysis
Descriptive statistics were used to summarize the basic information and the occurrence of injuries for the participants in the current study. The participants were classified into 2 groups according to the presence or absence of elbow injury in the dominant arm during the season. After confirming the normality of the basic information using the Shapiro-Wilk test, a Wilcoxon rank-sum test was conducted to compare the differences between the 2 groups. The difference between the groups in positive responses to each checklist item (ie, responses corresponding to 1) were evaluated using the chi-square test or Fisher exact probability test. The difference in the incidence of elbow injury between the 2011 and 2021 seasons was compared using the Fisher exact probability test. Statistical significance was set at P < .05.
Results
Of the 203 teams (4060 players) that received questionnaires, 98 (1335 participants, age range, 8-12 years) returned the questionnaires (collection rate, 32.9%). The final analysis population (excluding incomplete questionnaires) was 678 (age, 10.6 ± 1.1 years). There were no significant differences in age, height, weight, height, height/weight increases within the past 12 months, sleep duration, or baseball experience between the players with versus without elbow injury (Table 2). The basic information about the players included in the present study, and the 2011 survey are presented in Tables 2 and 3, respectively. 25 The incidence of injury of the players in this study is presented in Figure 1.
Comparison of Basic Information Between the Groups With and Without Elbow Injury in 2021 a
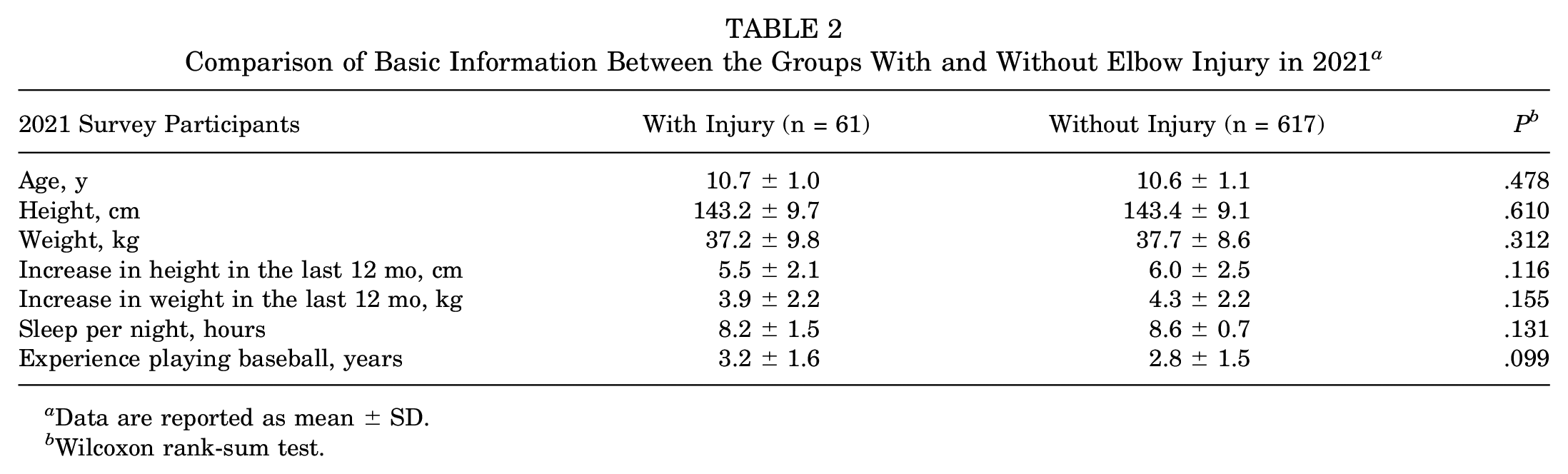
Data are reported as mean ± SD.
Wilcoxon rank-sum test.
Comparison of Basic Information Between the Groups With and Without Elbow Injury in 2011 a

Data are reported as mean ± SD. Boldface P values indicate statistically significant difference between groups (P < .05).
Unpaired t test for the interval scale.

(A) Percentage of players with injury according to area of the body. (B) Percent of players with elbow injury among players with pain in some part of the body..
A total of 61 (9.0%; age, 10.7 ± 1.0 years) experienced injuries in their dominant elbow during the 2021 season. By contrast, approximately 19.1% of all players reported elbow injuries in the 2011 survey. 26 Thus, the proportion of players with elbow injury decreased by approximately 10% compared with that 10 years ago (P = .01). In addition, 199 baseball players (29.4%; age, 10.8 ± 1.0 years) had experienced injuries in some part of the body during the 2021 season. Among these players, the proportion with elbow injuries (61 players) was 30.7% (Figure 1B).
A significantly higher percentage of players with elbow injuries had elbow pain in extension (item 2 on the study checklist, P < .001) and flexion (item 4, P < .0024), were regular players (item 5, P = .0288), played baseball under fatigue (item 8, P = .0028), and had lower and upper limb inflexibility (item 17, P = .0379; item 18, P = .0146; and item 22, P = .0085) (Table 4).
Comparison of Positive Responses to Checklist Items According to Players With and Without Elbow Injury

Values are reported as n (%). A positive response was a value of 1 for that checklist item. Boldface P values indicate statistically significant difference between groups (P < .05).
Discussion
We found that, compared with 10 years ago, the proportion of Little League players with elbow injuries had decreased by approximately 10%, which was a significant decrease (P = .01). The results of this study also revealed that the elbow joint accounted for the highest percentage (22%) of all injury sites and that approximately 30% of players with injuries in 1 part of the body had elbow injuries. Although the percentage of players with elbow injuries decreased compared with that 10 years ago, the percentage of elbow injuries was still higher compared with other body areas. Finally, we found that the percentages of players who had elbow pain in extension and flexion, were regular players, played baseball under fatigue, and had lower and upper limb inflexibility were significantly greater in the players with elbow injury versus those without elbow injury.
Our first discovery was that there was a decrease in the percentage of players with elbow injuries compared with the 2011 survey. In recent years, medical examinations have been actively conducted to detect elbow injury before it becomes serious.11,13 The examination started in Tokushima in 1981 and Kyoto in 2008 for junior high and high school students. In 2010, the scope was expanded to include elementary school students. In 2015, the Kyoto Rubber Baseball Association officially requested that all elementary school students in Kyoto be eligible for these checkups. 13 Hence, health checkups are clearly and actively being introduced. Moreover, previous studies have reported that medical checkups are effective for the early detection and treatment of elbow joint disorders.11,13,22 Since 2011, rules for limiting throwing have been established to prevent elbow joint damage owing to excessive throwing. The Japan Rubber Baseball Association and Japan Boys League Incorporated imposed a throwing limit allowing pitchers only 70 pitches per day.8,10 In previous studies, an increase in the number of pitches thrown has been reported to be a factor that increases the risk of throwing injuries.3,15,17 Therefore, the promotion of throwing restrictions is expected to prevent excessive fatigue. Based on these findings, the expansion of medical checkups and promotion of throwing restrictions have likely enabled the early detection of Little League elbow and reduction of the physical burden, thereby preventing the condition from becoming more severe.
Our second discovery was with the characteristics of players with elbow injury in terms of elbow pain during elbow extension (checklist item 2, P < .001) and flexion (item 4, P < .0024) movements. As elbow injuries are caused by joint movement during the throwing motion, they involves pain during joint motion, and different trends may be observed between the 2 groups. Next, we examined their characteristics in terms of being regular players (item 5, P = .0288) and playing baseball under fatigue (item 8, P = .0028). Of the respondents who reported elbow injuries, 85.2% were regular players, significantly higher than the 72.3% of regular players without it. Regular players in baseball often continue to play from the beginning to the end of a game, and they may play more hours in a game and throw more pitches at full strength than nonregular players. Therefore, they might practice while their bodies remain fatigued. This fatigued state corresponds to item 8, where players who reported elbow injury played baseball with a tired arm at a significantly higher rate. In a previous study, a pitcher who regularly pitches despite arm fatigue reportedly has 36 times increased risk of injury. 19 Continued throwing without sufficient reduction in muscle fatigue and stress on the muscle-tendon attachments may induce pain due to the large load applied by continued throwing. 24 Based on these findings, a different trend may be observed between groups in items 5 (being regular players) and 8 (playing baseball under fatigue).
Regarding the relationship between checklist about lower and upper limb inflexibility (item 17 on the study checklist, P = .0379; item 22, P = .0085) and elbow injury. A significantly larger percentage of players with elbow injury had a higher risk of injury in items 17 (left-right difference in the angle when opening the leg with the knee closed while prone) and 22 (inability of the heel to cross the upper half line of the opposite thigh when raising the leg with the knee extended while in prone). If the player corresponded to the left-right difference in the angle of the leg opening with the knee closed while in supine (item 17), a decreased ROM of internal rotation of the hip joint was observed. In addition, if these players classify in no. 22, hamstring shortening occurs when the heel cannot cross the line of the upper half of the opposite thigh when the leg is raised with the knee extended on the back.
The throwing motion in baseball is generally subdivided into 6 phases. 14 In this study, the throwing motion is divided into the wind-up phase (beginning with wind-up during the preparation phase until the nonthrowing leg is maximally raised), stride phase (shoulder abduction and external rotation occur until the stepping leg touches the ground in the throwing direction), arm-cocking phase (shoulder joint of the throwing arm is externally rotated to the maximum), arm acceleration phase (starting with internal rotation of the upper arm until ball release), arm deceleration phase (from ball release to maximum internal rotation of the shoulder), and follow-through phase (until all movements are completed). In the case of a right-handed pitcher, the left leg is maximally raised in the right single-leg standing posture during the wind-up phase. During the stride phase, the pelvis undergoes left hip external rotation and right hip internal rotation movements. 4
Another study reported that decreased hip internal rotation ROM and hamstring shortening are inhibitors of optimal rotational motion of the hip, pelvis, and trunk, causing decreased energy transfer from the lower to the upper extremity. 21 Based on these findings, decreased hip internal rotation ROM and hamstring shortening may have caused a more upper body-dependent throwing form, which failed to reduce the load on the elbow joint applied during ball release, thus contributing to the development of the disorder.
A significantly larger percentage of players with elbow injuries had a higher risk of injury in item 18 (a left-right difference in height when the hands are placed behind the back and along the upper spine in an upward direction). A player with this left-right difference has a decreased internal rotation ROM of the shoulder joint. Previous studies have reported that decreased shoulder internal rotation ROM can be a risk factor for elbow disorders, 23 and that the interaction generated by shoulder internal rotation provides internal acceleration that protects against external loads on the elbow joint. 20 Thus, decreased internal rotation ROM of the shoulder joint may increase stress on the elbow joint applied during the throwing motion, thus leading to the development of injury.
Limitations
This study has several limitations. First, players were influenced by the recall and selection bias when answering the questionnaire. To minimize this bias, we asked for the cooperation of parents who could observe objectively as a third-party and nearby and instructed the parents and players to complete the questionnaire together. In addition, to help parents without medical knowledge to answer the questions, we used pictures to explain the evaluation methods for the throwing form and flexibility and simple tests that the participants could evaluate by themselves. However, accurate data are required to highlight causal relationships. Second, the number of pitches reported as risk factors has yet to be fully investigated. As this was a cross-sectional study, accurate annual pitch counts could not be collected. In addition, the causal relationship between the presence or absence of elbow injury and players’ physical characteristics is unknown. It is also possible that many other factors besides pitching limitations, such as strength and conditioning techniques, mechanics, and classes for pitchers, may be related to the reduced incidence of elbow injury. Finally, because this study was limited to Little Leaguers in Kyoto and the collection rate of this study (32.9%) was low, its generalizability to other populations and regions remains to be discovered. The low collection rate may have been due to the need for more enforcement of questionnaire collection, since the survey was paper-based with a lot of work and processes involved in returning the questionnaires. To increase the rate, online surveys are recommended as they are easier to complete with fewer processes associated with returning responses. Further research is needed to confirm the external validity of the incidence of injury and physical characteristics of players with injuries.
Conclusion
The incidence of elbow injury has decreased significantly over the past 10 years, although the elbow joint still accounts for almost one-third of all injuries in Japanese youth baseball players. In addition, players with elbow injuries had significantly higher rates of lower- and upper-limb inflexibility. This study was limited to Little Leaguers in Kyoto, and the collection rate of this study (32.9%) was low. Future research could involve expansion of the study sample to other populations and regions to investigate generalizability. In addition, a longitudinal study should be conducted to clarify the causal relationship between the incidence of elbow injury and player characteristics as well as number of pitches thrown.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671231200844 – Supplemental material for Incidence and Characteristics of Elbow Injury in Japanese Youth Baseball Players: Comparison Between 2011 and 2021
Supplemental material, sj-pdf-1-ojs-10.1177_23259671231200844 for Incidence and Characteristics of Elbow Injury in Japanese Youth Baseball Players: Comparison Between 2011 and 2021 by Chika Kouno, Miyu Onishi, Rika Kawabe, Naoki Doi, Yukinobu Tahu, Momoko Nagai-Tanima and Tomoki Aoyama in Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgements
The authors express their deepest gratitude to Yukinobu Tafu for his assistance in data collection; the members of the elementary school baseball team in Kyoto for their cooperation in measurements; and the members of the Department of Human Health Science, Graduate School of Medicine, Kyoto University, for their guidance in conducting this study. The authors also thank Editage (![]() ) for its English language editing.
) for its English language editing.
Final revision submitted April 9, 2023; accepted May 3, 2023.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Kyoto University (no. R3061).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.