
Abstract
Background:
Superior labral anterior-posterior (SLAP) tears are increasingly common shoulder injuries in adolescent athletes participating in overhead throwing.
Purpose/Hypothesis:
The purpose was to evaluate outcomes, satisfaction, and competitive level progression in adolescent baseball athletes who underwent SLAP repair. It was hypothesized that pitchers may experience inferior outcomes compared with nonpitchers, and collegiate athletes may have decreased outcomes compared with lower-competition-level athletes.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients aged 10 to 19 years who underwent SLAP repair from 2008 to 2018 with a minimum 2-year follow-up were identified from a single institution’s medical records. Nonbaseball athletes and nonthrowing shoulders were excluded. Patients were contacted via telephone to complete patient-reported outcome (PROs) scores, including the Western Ontario Shoulder Instability Index (WOSI), Kerlan-Jobe Orthopaedic Clinic Shoulder and Elbow Score, 12-item Short Form Survey Mental Component Summary and Physical Component Summary, Single Assessment Numeric Evaluation, and a custom return-to-play (RTP) questionnaire.
Results:
A total of 59 baseball players met the inclusion criteria, and 76.3% (45/59) were successfully contacted for follow-up. All patients were male, with a mean age of 17.4 ± 1.5 years (range, 14-19 years). The mean follow-up was 5.3 ± 2.6 years (range, 2.1-12.1 years). The overall RTP rate was 75.6% (34/45), with a mean time from surgery to initiation of throwing of 5.9 ± 2.0 months (range, 2-12 months) and a mean time of 11.3 ± 3.5 months (range, 6-22 months) until full competition. Athletes continued competitive baseball for a mean of 2.9 ± 1.9 years (range, 0.5-8.0 years) after surgery. At the time of final follow-up, 71.1% (32/45) of players had stopped playing baseball and 22% (10/45) attributed cessation to subjective shoulder limitations. No significant differences were found in RTP rates or PROs, although pitchers reported worse postoperative performance (P = .013).
Conclusion:
Adolescent baseball players undergoing SLAP repair had favorable RTP rates and PROs, with no significant differences between pitchers and position players. Despite pitchers reporting worse postoperative performance, overall satisfaction rates were high. Adolescents who stopped playing baseball generally discontinued play for reasons other than postsurgical shoulder function. These findings can help orthopaedic surgeons set realistic expectations for adolescent baseball players undergoing SLAP repair.
The superior labral anterior-posterior (SLAP) lesion, first described by Andrews et al 2 and coined by Snyder et al, 27 receives its designation due to the characteristic tear pattern commonly seen in throwing athletes. Several credible mechanisms of injury have been proposed, with one of the most common mechanisms relating to the overhead throwing athlete’s repetitive throwing motion.2,4,11,27,29 This motion, compounded over time, puts tremendous stress on the biceps tendon and thus significant strain on its attachment to the superior labrum, which ultimately results in a SLAP tear. 4 Shoulder injuries are especially common among baseball athletes, and early participation in pitching has been shown to lead to the development of anatomic changes in the young thrower. 15
Part of the changes to the throwing shoulder may be attributable to the increase in participation in high school sports and the general trend for earlier sport specialization among adolescent athletes. Unfortunately, these so-called highly specialized athletes are at higher risk for injury. 3 In baseball specifically, a major risk factor for shoulder and elbow injuries is increased total pitch counts whether in the form of more games per year or starting pitching at a younger age. 21 Despite the awareness of increased risk for these young athletes, shoulder and elbow injuries continue to be on the rise with the goals of highly coveted college scholarships and higher career aspirations on the line. The initial standard of care remains nonoperative management. For SLAP tears, this entails initial time off from throwing, focused therapy to address any glenohumeral internal rotation deficits, periscapular strengthening, and a graduated throwing program, all of which allow most athletes to return to sport at a similar level. 28 However, the number of high school baseball athletes requiring surgery for throwing-related injuries has significantly increased. 21
Overall, the reported return-to-play (RTP) rates after SLAP repair have varied greatly and, as a whole, remain unsatisfactory.5,7,9,19,20,22,23 In a systematic review, Sayde et al 25 reported that 73% of patients with SLAP type 2 lesions were able to return to their previous level of play, but only 63% of overhead athletes were able to achieve their previous level. In the largest single study on RTP after SLAP repairs in >200 baseball players, Gilliam et al 8 found that, overall, 62% of athletes returned to play. Although their cohort did include high school–aged athletes (n = 47), no athletes younger than high school age were included, and the cohort likewise incorporated athletes who were already professional at the time of injury.
The purpose of this study was to evaluate the clinical outcomes after SLAP repair in adolescent baseball players. Secondarily, we wished to characterize the sport progression of these young athletes after injury and their rates of career advancement. We hypothesized that RTP rates and functional outcomes would be similar to those previously reported in the literature and that rates of advancement in these young athletes would be low. We also hypothesized that pitchers would perform worse than position players and collegiate players would perform worse than their younger counterparts due to the increased demands of higher-level competition.
Methods
Institutional review board approval was obtained (20E.392) under exempt status on April 23, 2020. Patients between the ages of 10 and 19 years, per the World Health Organization definition of adolescent age, who underwent a primary SLAP repair over a 10-year period from 2008 to 2018 with a minimum 2-year follow-up were identified by a database query in the medical records of a multicenter single-practice group. No formal power analysis was performed before study initiation. Seventeen surgeons contributed cases to this query. From this initial cohort, nonbaseball athletes and injuries to nonthrowing shoulders were excluded. Patients were also excluded if they had labral pathology outside the 11-o’clock to 1-o’clock position, a full-thickness rotator cuff tear requiring a repair, anterior glenohumeral instability, or acromioclavicular joint osteoarthritis/instability. After identifying these patients, a thorough chart review of the patient’s imaging, clinic, and operative notes was performed to gather patient demographics and intraoperative details. A SLAP tear diagnosis was rendered based on clinical suspicion and supported by magnetic resonance imaging. All patients had failed nonoperative management and were thereafter indicated for a SLAP repair for continued symptoms of shoulder dysfunction and pain.
All SLAP repairs were done arthroscopically using suture anchors. Knotted versus knotless technique, simple versus mattress sutures, and implant company varied among the cohort and were left to the discretion of the surgeon. The RTP protocol followed a similar physical therapy–guided rehabilitation progression among surgeons in the cohort without a uniform definitive time for initiation of a throwing program or clearance for full return to competition.
Patients were only included in our analysis if they were able to be contacted via telephone to complete patient-reported outcome (PRO) scores, including the Western Ontario Shoulder Instability Index (WOSI), Kerlan-Jobe Orthopaedic Clinic (KJOC) Shoulder and Elbow Score, 12-item Short Form Survey Mental Component Summary and Physical Component Summary, Single Assessment Numeric Evaluation, and a custom RTP questionnaire (Appendix).1,12,30 Within the custom RTP survey, patients were asked about the current status of their shoulder, level of competitive play before and after surgery, their ability to RTP, and time to return to throwing/competition, among several other items. Complete RTP in our cohort was defined as the date that patient was able to return to game play.
Statistical Analysis
Continuous variable data are reported as means with standard deviations, and categorical data are reported as frequencies with percentages. Continuous variables compared between 2 groups were assessed using the t test, while categorical variables between ≥2 groups were assessed using the chi-square or Fisher exact test. Both Shapiro-Wilk and Kolmogorov-Smirnov tests were used to ensure normality of data. Statistical significance was set at a P value <.05. All statistical analyses were performed with Statistical Package for the Social Sciences (SPSS) Statistics software Version 26 (IBM).
Results
A total of 59 baseball players met the inclusion criteria for this study, and 76.3% (45/59) of patients were successfully contacted to complete final follow-up surveys at a minimum of 2 years. All patients were male, with a mean age of 17.4 ± 1.5 years (range, 14-19 years). The mean body mass index of this cohort was 25.3 ± 3.4 (range, 21-31). The mean number of anchors used for all athletes was 2.98 ± 1.5, and the mean percentage of patients receiving knotless anchors was 29% (12/41). The mean follow-up of this cohort was 5.3 ± 2.6 years (range, 2.1-12.1 years). At the time of the injury, there were 17 (37.8%) pitchers, 15 (33.3%) infielders, 9 (20.0%) catchers, and 4 (8.9%) outfielders. Overall, there were 2 (4.4%) players competing in middle school, 29 (64.4%) players competing in high school, and 14 (31.1%) players competing in college. The path to inclusion is demonstrated in a flowchart in Figure 1. RTP rates by position and education level are listed in Table 1.
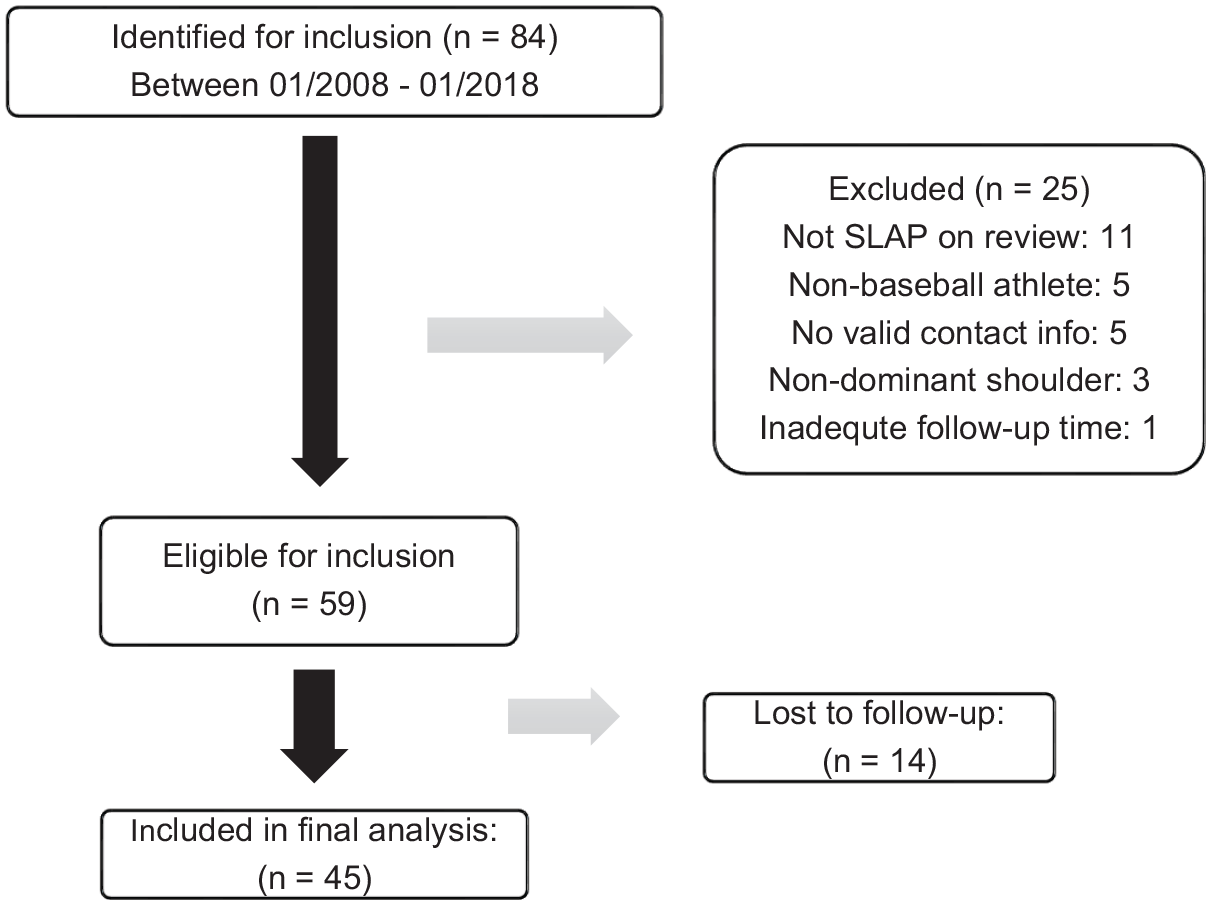
Flowchart demonstrating the initial full patient population and final patients meeting the inclusion criteria. SLAP, superior labral anterior-posterior.
Return-to-Play Data a
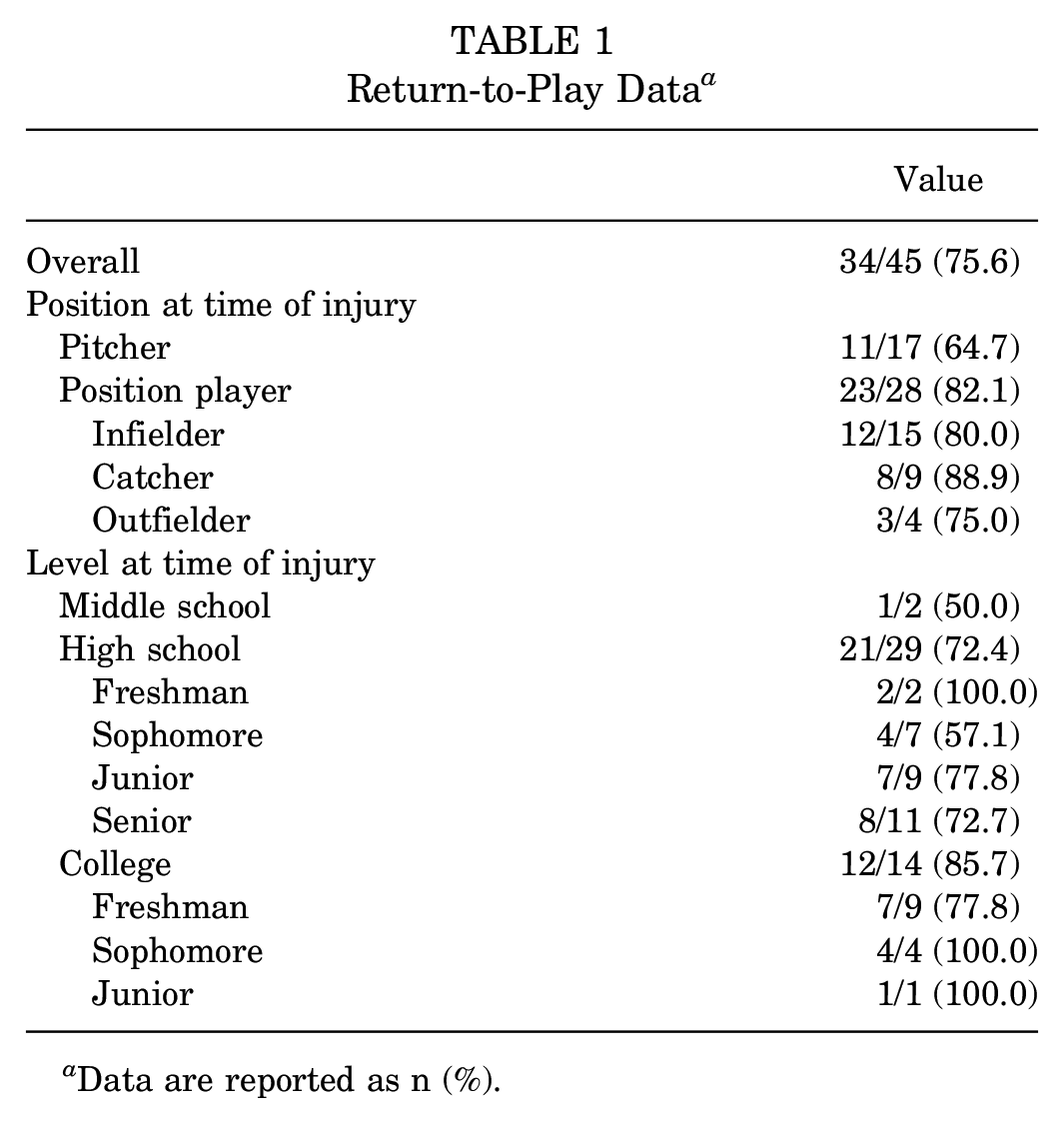
Data are reported as n (%).
The overall RTP rate was 75.6% (34/45). Of 31 middle and high school players, 22 (71.0%) were able to RTP, whereas 12 (85.7%) of 14 collegiate players were able to RTP (P = .458). Of 45 athletes who were able to RTP, 27 (60%) did so in the same position. Of the players who were able to return, 6 precollegiate players and 1 collegiate player reported switching positions on return to full competition due to shoulder limitations, including pain, loss of velocity, or shoulder “not feeling the same.” Three players switched to playing outfield, 1 switched to catching, 1 switched to first base, 1 switched to designated hitting, and 1 responded “N/A” (not applicable). Two of these players were pitchers, one who switched to first base and the other to the outfield. The mean time from surgery to initiation of throwing was 5.9 ± 2.0 months (range, 2-12 months), and the mean time to return to full competition was 11.3 ± 3.5 months (range, 6-22 months) after surgery. After repair, the group that successfully returned reported continuing playing baseball competitively for a mean of 2.9 ± 1.9 years (range, 0.5-8.0 years) after surgery. Of those who returned to baseball after surgery, 12 high school players were able to continue playing through the collegiate level, as well as the 1 middle school player (13/31; 42%). None of the 12 collegiate players who returned were able to progress to the professional level. At the time of final follow-up, 71.1% (32/45) of players had stopped playing baseball. Of those who had stopped playing competitive baseball, 10 (31.3%) reported their shoulder prevented them from playing, 12 (37.5%) reported it was because they were not recruited to the next level, and 10 (31.3%) reported they lost the desire to play. Thus, 22% (10/45) of the original cohort stopped baseball specifically due to their shoulder.
When comparing pitchers with position players, RTP rates, duration required to return, and duration played on return were not significantly different. However, when postoperative sporting performance was subjectively assessed, pitchers were less likely to have felt they stayed the same or improved their performance level relative to their preoperative level when compared with position players (P = .013). When comparing precollegiate players with collegiate players, there was again no difference in RTP rates, time spent in rehabilitation before return to throwing, or duration of time played after surgery. However, collegiate players required longer to return to game play compared with their counterparts playing at a lower level (P = .024). Detailed information regarding time to return, postoperative performance, and duration of postoperative play is provided in Table 2.
Return-to-Play Comparisons by Position and Level a

Data are reported as mean ± SD unless otherwise indicated. Bold P values indicate statistical significance.
When analyzed by position, there were no significant differences in any of the PRO measures between pitchers and position players. Additionally, there were no significant differences when analyzed by level between precollegiate and collegiate-level players. The overall satisfaction score was 83.2%. Of all athletes, 86.7% (39/45) said they would undergo the surgery again if given the opportunity. Full PRO data are provided in Table 3.
Patient-Reported Outcomes a

Data are reported as mean ± SD unless otherwise indicated. KJOC, Kerlan-Jobe Orthopaedic Clinic; MCS, Mental Component Summary of 12-item Short Form Survey; PCS, Physical Component Summary of 12-item Short Form Survey ; SANE, Single Assessment Numeric Evaluation; WOSI, Western Ontario Shoulder Instability Index.
None of the players reported any major postoperative complications, including infection, venous thrombosis, or embolism. However, 3 players reported having another injury requiring subsequent surgery at a mean of 14 months postoperatively. Two of the patients reported having a traumatic anterior shoulder dislocation that was reduced and eventually required surgical intervention during the study period. One of the traumatic dislocations occurred while throwing at 12 months after surgery. The second traumatic dislocation occurred at 18 months and did not occur during sporting activity. Finally, 1 patient underwent repair of a rotator cuff injury sustained while throwing at 24 months postoperatively in the ipsilateral shoulder. All 3 patients were noted to have SLAP repair intact at the time of revision surgery. All 3 patients were able to return to baseball after their second surgery.
Discussion
In our investigation of clinical outcomes after SLAP repairs in adolescent baseball players, we found that 75.6% (34/45) of players were able to RTP at a mean of 11.3 months postoperatively. A higher proportion of pitchers reported their subjective postoperative performance levels as lower than preoperative levels, in line with our hypothesis that pitchers would have inferior outcomes to position players. Likewise, collegiate players took 2 more months, on average, to RTP than lower-competition-level athletes. Otherwise, when analyzing outcomes by position or level of play, players had equivalent PRO scores and RTP rates.
While historical RTP rates after SLAP repairs have been extremely variable, our RTP rate of 75.6% falls within the wide range of 22% to 83% reported in the literature.6 -8,20,22,26 Although few studies have focused specifically on this younger population, our RTP rates were superior to those in the study by Gilliam et al, 8 who reported RTP rates of 62% and 60% in their high school (n = 47) and college players (n = 63), respectively. In contrast, the RTP outcomes of our cohort were inferior to those of Douglas et al, 6 who reported an RTP of 81% in their high school players (n = 27) and 83% in their collegiate players (n = 36), further emphasizing the variability seen in SLAP repair outcomes. Albeit reflective of the literature, this cohort’s outcomes after SLAP repairs support that further investigation is warranted on the best course of treatment for these patients. Only one surgical option was addressed in our study, but it is worth noting that bicep tenodesis is also an option for athletes who have failed nonoperative treatment. The outcomes for tenodesis show a similar variability between studies, as seen with SLAP repair, but most athletes fair well aside from pitchers, who have a notably inferior response to tenodesis. 14 It is likely that there is not one treatment option that will serve as a panacea for all-comers with SLAP pathology, and the best treatment option may require an individualized approach based on severity of symptoms, current level of play, and future competitive sporting goals.
Our study reveals that SLAP repair in this patient population results in outcome scores that are lower than would be expected for a healthy baseball player, especially in comparison with another common procedure in this population, ulnar collateral ligament reconstruction (UCLR). The mean overall KJOC score in the present study was 60.0, which is starkly inferior to the mean KJOC scores reported in a similar patient population after UCLR, which range from 83 to 85.10,24 The KJOC score has previously been demonstrated to be particularly sensitive in assessing symptoms in overhead athletes, as demonstrated by Kraeutler et al. 13 They found that only 16% (7/44) of asymptomatic pitchers had a KJOC score <90.
One of our secondary goals was to investigate the postsurgical athlete progression after SLAP repair in this infrequently analyzed population. It is possible that player advancement may have been negatively affected or that some lower-skill players were not captured and quit baseball after their injury, but 41.4% (12/29) of high school players were still able to advance to play in college in this cohort, which is notably higher than the 8.1% rate of high school athlete to National Collegiate Athletic Association participation conversion. 18 However, none of the players who were in high school or college at the time of injury were able to advance to professional status. Of note, only 22% of the cohort cited limitations from their shoulder as their reason for not continuing baseball by the time of final follow-up. Undoubtedly, early-career injuries can influence long-term career success, but the mean 3-year postoperative career is also likely to be due in part to how incredibly selective and competitive the collegiate and professional baseball recruitment process is.
Specific shoulder injury rates vary between sports, but with respect to baseball, 32% to 35% of youth baseball pitchers will experience shoulder pain over the course of a season.16,17 While there have been several studies investigating outcomes of elite baseball players, there have been comparatively limited data for younger, preprofessional cohorts. The need for more data on younger cohorts becomes increasingly more crucial as our adolescent athletes continue to sport-specialize and put themselves at risk for injury at younger ages and ultimately surgical treatment. 21 Continued emphasis on limited year-round throwing, preseason conditioning, and proper throwing mechanics is imperative. Furthermore, careful compliance with recommendations set forth by multiple governing bodies including state and national baseball organizations’ recommended pitch counts is necessary to help decrease the incidence of SLAP lesions and posttreatment retears in this young population.
Limitations
While this study represents one of the first to present a single large group of adolescent baseball player outcomes after SLAP repairs and a novel initiative to detail their progression after injury, it is not without limitations. First, this is a retrospective investigation and is therefore subject to selection as well as recall bias. Our study lacked preoperative data, thus limiting our ability to quantify the average absolute benefit achieved by this surgical intervention. Our study also did not include a surgical intervention alternative, such as biceps tenodesis, with which to compare postoperative outcomes. Postoperative data were readily gleaned from charts, but given the large number of surgeons contributing to the cohort, their typical referral pattern based on athlete competition level, and regional variation of a large practice group, there is significant heterogeneity in the care across these athletes during the study period. While our focus was the adolescent athlete, the ceiling effect of competitive play makes the established postsurgical duration of play period difficult to generalize as the ability to continue long-term engagement even without injury is markedly different for an early-adolescence athlete versus an adolescent-aged collegiate athlete. Finally, while this study presents one of the largest sample sizes for this study population, there is still a relatively low number of athletes in this study group. Thus, it is likely that some comparisons made were underpowered to detect true differences.
Conclusion
Adolescent baseball players who underwent SLAP repair had good RTP rates and PROs with no statistically significant differences between pitchers and position players. Pitchers reported worse postoperative performance, although satisfaction rates were high in all positions. Of the adolescent athletes who stop playing baseball with time, a majority discontinued play for reasons other than a subjective limitation secondary to their postsurgical shoulder performance. These findings can help orthopaedic surgeons better counsel adolescent baseball players on expectations after SLAP repair.
Footnotes
Appendix
Please describe your symptoms after surgery:
Were you actively playing baseball when you had your shoulder injury and SLAP repair?
What was your primary position prior to surgery?
At what level of competition did you compete before your injury?
After your SLAP repair surgery did you return to baseball?
How many months after surgery did you return to throwing a baseball?
_____________
How many months after surgery did you return in a game?
______________
What was your primary position following your surgery?
At what level of competition did you first return to after surgery?
What was the highest level of competition that you were able to attain after surgery?
Which of the following best describes you currently?
How long did you play baseball competitively after your surgery (years)?
___________
Have you stopped playing baseball?
Why did you stop playing baseball eventually?
Additional details: ____________
Please describe your satisfaction with the result of your surgery on a scale from 1 to 100. ____________
If given the chance again, would you undergo the SLAP repair surgery you had?
Since your SLAP repair surgery, have you sustained an injury to either your throwing elbow or shoulder?
How many months after your surgery did you sustain this injury?
_____________
Please select all injuries that apply:
Did you experience any complications with your SLAP surgery? Please explain. ___________________
Acknowledgements
We acknowledge Gaston Davis, MD, for his assistance with data collection.
Final revision submitted April 14, 2025; accepted April 23, 2025.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Institutional review board approval was obtained (20E.392) under exempt status.