
Abstract
Background:
Superior labrum from anterior to posterior (SLAP) lesions represent a significant cause of shoulder pain and disability among active duty members of the US military. However, few data exist regarding the surgical management of type VIII SLAP lesions.
Hypothesis:
We hypothesized that arthroscopic repair would decrease pain and increase function at the midterm follow-up and allow for a high rate of maintenance of active duty status.
Study Design:
Case series; Level of evidence, 4.
Methods:
Consecutive active duty military patients were identified from January 2011 through June 2015 who underwent arthroscopic repair of type VIII SLAP lesions performed by a single surgeon. Patients were excluded if they underwent glenoid microfracture, other capsulolabral repair, or rotator cuff repair. Outcome measures were completed by patients within 1 week before surgery and at latest follow-up: pain visual analog scale, Single Assessment Numeric Evaluation, American Shoulder and Elbow Surgeons shoulder score, and Rowe instability score.
Results:
A total of 30 patients met the inclusion criteria for the study. The mean ± SD follow-up was 96.60 ± 10.91 months. At final follow-up, the mean visual analog scale score improved from 8.17 ± 1.6 to 1.63 ± 1.90 (P < .0001), the Single Assessment Numeric Evaluation score from 41.65 ± 16.78 to 87.63 ± 13.02 (P < .0001), the American Shoulder and Elbow Surgeons score from 36.47 ± 10.26 to 88.07 ± 13.94 (P < .0001), and the Rowe score from 35.33 ± 6.56 to 90.00 ± 14.68 (P < .0001). Three patients reported postoperative complications, and 1 progressed to further surgery. Overall, 90% of patients remained on active duty military service and were able to return to preinjury levels of work and recreational activity. The failure rate, defined as persistent instability or activity-limiting pain, was 10%.
Conclusion:
The results of this study demonstrated favorable outcomes for the majority of patients after arthroscopic repair of type VIII SLAP lesions at midterm follow-up, supporting repair as a viable treatment option for type VIII SLAP tears in this patient population.
Superior labrum from anterior to posterior (SLAP) lesions represent a significant cause of shoulder pain and disability among active duty members of the US military. 14,31 First described by Andrews et al 1 in 1985, SLAP lesions have since been characterized by Snyder et al 28 and Maffet et al. 16 Type II lesions, the most common variant, occur when there is detachment of the superior labrum and the origin of the long head of the biceps tendon insertion from the superior aspect of the glenoid. 10,29 More recently, type VIII SLAP lesions have been defined as type II lesions with posteroinferior extension involving the posterior band of the inferior glenohumeral ligament (Figure 1). 6,9,17
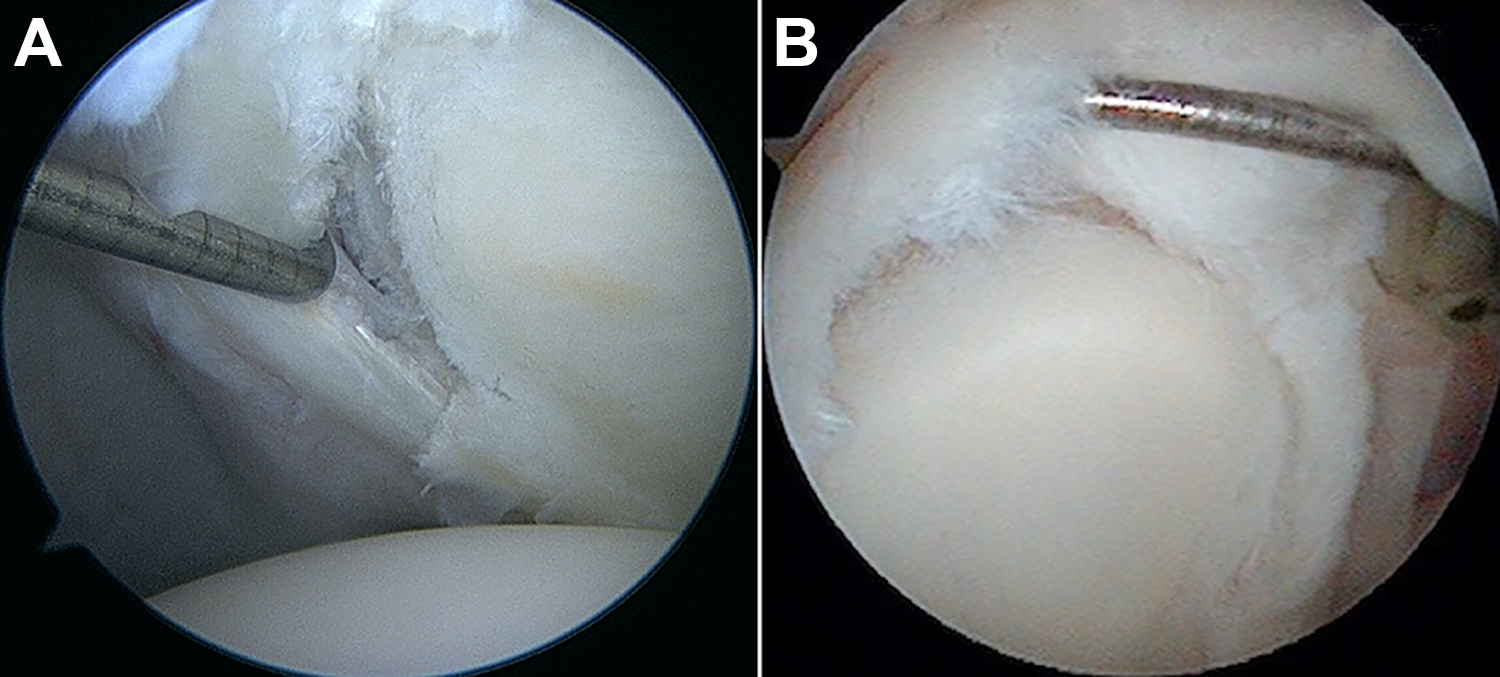
Arthroscopic images of a 27-year-old patient with a type VIII SLAP tear. Note the (A) posterior and superior involvement of the labrum, with (B) instability of the biceps anchor.
There is a paucity of data regarding the operative management of type VIII lesions. In an analysis of 46 patients, Fourman et al 9 found that arthroscopic repair of type VIII lesions led to significant improvements in outcome scores, pain, range of motion, and stability at midterm follow-up, albeit with better results reported among nonthrowing athletes. In a study of 13 patients with glenohumeral instability secondary to a type VIII lesion, Seroyer et al 26 reported favorable outcomes after capsulolabral reconstruction. Most recently, Arner et al 2 demonstrated significant improvements in pain, function, and range of motion at minimum 4-year follow-up after repair of type VIII lesions in 34 athletes. To our knowledge, there is no literature regarding the treatment of this injury in active duty military patients.
The purpose of this study was to report midterm outcomes after arthroscopic repair of type VIII SLAP lesions in active duty military patients <35 years old, a population that experiences a high incidence of SLAP lesions as well as posterior instability and is at increased risk for unsatisfactory postoperative outcomes. 3,4,31,33 We hypothesized that arthroscopic repair would decrease pain and increase function at midterm follow-up and allow for a high rate of maintenance of active duty status.
Methods
This was a retrospective analysis of prospectively collected data of military patients who underwent arthroscopic repair for type VIII SLAP tears between January 2011 and June 2015. Institutional review board approval was obtained before beginning the study. Informed consent was obtained from all participants.
Patient Population
Inclusion criteria included active duty military patients <35 years old with a minimum of 5 years of follow-up, defined as complete outcome scores pre- and postoperatively at latest follow-up. All surgical procedures were performed by the senior surgeon (N.P.), who is a shoulder and elbow fellowship–trained surgeon with a large active duty military population.
Exclusion criteria were previous shoulder surgery, age ≥35 years, any capsulolabral pathology other than a type VIII SLAP tear, concomitant rotator cuff pathology, glenohumeral cartilage injuries, calcific tendinitis, and psychogenic voluntary shoulder subluxation. During the study period, the senior surgeon surgically treated 53 patients with type VIII SLAP tears. Fourteen patients were >35 years old; 5 underwent concomitant microfracture of a glenoid osteochondral defect; and 2 had concomitant repair of a full-thickness rotator cuff tear. As a result, 32 patients were eligible for study inclusion. Two patients were lost to follow-up, leaving 30 (93.75%) available for final analysis.
In our practice, an initial trial of nonoperative management is preferred, given the higher risk of poor postoperative outcomes after SLAP repair observed in active duty patient populations. Nonoperative management was composed of activity modification, anti-inflammatory medications, home exercise programs, and at least 3 months of physical therapy. Activity modification consisted of placement on a temporary physical profile to allow for modification of physical readiness training and avoidance of combat arms training and combatives. All patients were evaluated with 1.5-T magnetic resonance gadolinium arthrogram, which was retrospectively reviewed with arthroscopic images and operative reports. All patients on diagnostic arthroscopy had detachment of the biceps anchor from the glenoid with posteroinferior extension involving the posterior band of the inferior glenohumeral ligament.
Patient demographics were collected, including age, sex, military occupation, and laterality. Pre- and postoperative evaluation (minimum 5-year follow-up) involved range of motion, visual analog scale for pain, the Single Assessment Numeric Evaluation (SANE) score, the Rowe instability score, and the American Shoulder and Elbow Surgeons (ASES) shoulder score. Complications and return to activity were also collected as part of the postoperative evaluation.
Surgical Procedure
The senior surgeon’s surgical technique did not change markedly during the study period. All patients were positioned in a modified beach-chair position after administration of general anesthesia and a presurgical interscalene block. An examination was performed under anesthesia to assess range of motion and shoulder stability in the anterior and posterior directions. All patients had a 3+ posterior drawer with no increased laxity in the anterior and inferior directions. A Spider hydraulic arm holder (Smith & Nephew) was then used to stabilize the operative shoulder, and the patient was draped. Diagnostic arthroscopy was conducted through the posterior viewing portal and anterior portal.
To identify detachment of the biceps anchor from the glenoid (type II SLAP tear) and differentiate it from the sublabral foramen (normal anatomic variant), we performed the peel-back test, in which the arm is brought to a position of abduction and external rotation and the superior labrum is peeled back from the superior glenoid. In addition, we passed a probe from the anterior portal to assess the stability of the biceps anchor. Typical intraoperative findings included chondromalacia at the area of detachment with corresponding fraying on the underside of the detached superior labrum. Evaluation of the posterior labrum was performed with the arthroscope in the anterior portal.
Any present intra-articular pathology was addressed. Arthroscopic acromioclavicular joint resection arthroplasty was performed if patients had preoperative physical examination findings or symptoms suggestive of acromioclavicular joint osteoarthritis. Subacromial decompression was performed for all patients, as we have found that the delay from time of injury to appropriate treatment often observed in active duty military patients predisposes the affected shoulder to develop subacromial bursitis secondary to altered kinematics.
SLAP repairs were performed using double-loaded suture anchors (Gryphon PEEK; DePuy Mitek). The number and placement of anchors were determined by the location and size of the lesion, although most tears were repaired with 4 or 5 anchors (mean ± SD, 4.03 ± 0.81; range, 3-5). Anchors anterior to the biceps root were placed through an anterosuperolateral portal, and anchors posterior to the biceps root were placed via the trans–rotator cuff portal as described by O’Brien et al. 19 Repair of the posterior labrum from inferior to superior was completed first, followed by repair of the SLAP component. Simple sutures were passed, and sliding knots were tied arthroscopically (Figure 2).

Intraoperative pictures of a completed type VIII SLAP repair in the patient shown in Figure 1. (A, B) Posterior views demonstrate good restoration of the capsulolabral bumper. (C) Superior view shows repair of the type II SLAP tear at the superior labrum, with demonstrated stability of the biceps anchor.
Postoperative Rehabilitation
Patients were discharged the same day of the procedure and instructed to begin pendulum shoulder and elbow, wrist, and finger active range of motion exercises without shoulder movement once they experienced resolution of the interscalene block. Narcotic pain medications were prescribed for up to 10 days postoperatively.
Patients were immobilized in neutral rotation shoulder position in a SmartSling (Ossur) for 4 weeks. At 4 weeks postoperatively, the sling was discontinued, and passive forward flexion was allowed, with a gradual progression of forward flexion from 90° to 150°. Active range of motion of the shoulder and a progressive strengthening program started at 6 weeks postoperatively. All patients attended physical therapy at the same military physical therapy group and followed the same postoperative rehabilitation protocol. 5 Return to unrestricted activity, including push-up and bench press activities, was allowed as early as 6 months postoperatively, pending the observation of a negative posterior apprehensive test result and the patient’s reporting a subjective readiness to return to full active duty.
Statistical Analysis
Statistical analyses were performed using SPSS Statistics Version 25.0 (IBM). Continuous data were described by mean and standard deviation. A paired t test was used to compare pre- and postoperative data. Chi-square analysis was used to evaluate categorical variables. Statistical significance was set at P < .05 in all cases.
Results
The study included 30 patients who underwent arthroscopic repair of a type VIII SLAP lesion between January 2011 and June 2015. All 30 (100%) were male, with a mean age of 31.43 ± 7.67 years. The mean time from injury to surgery was 17.70 ± 18.65 months, and the mean follow-up time was 96.60 ± 10.91 months. The mechanism of injury was sporting activity in 11 patients, military activity in 8, fall in 3, motor vehicle accident in 1, and nonspecific injury in 7. Table 1 summarizes the demographic and surgical characteristics of the study population.
Study Population Characteristics (30 Patients, 30 Shoulders)
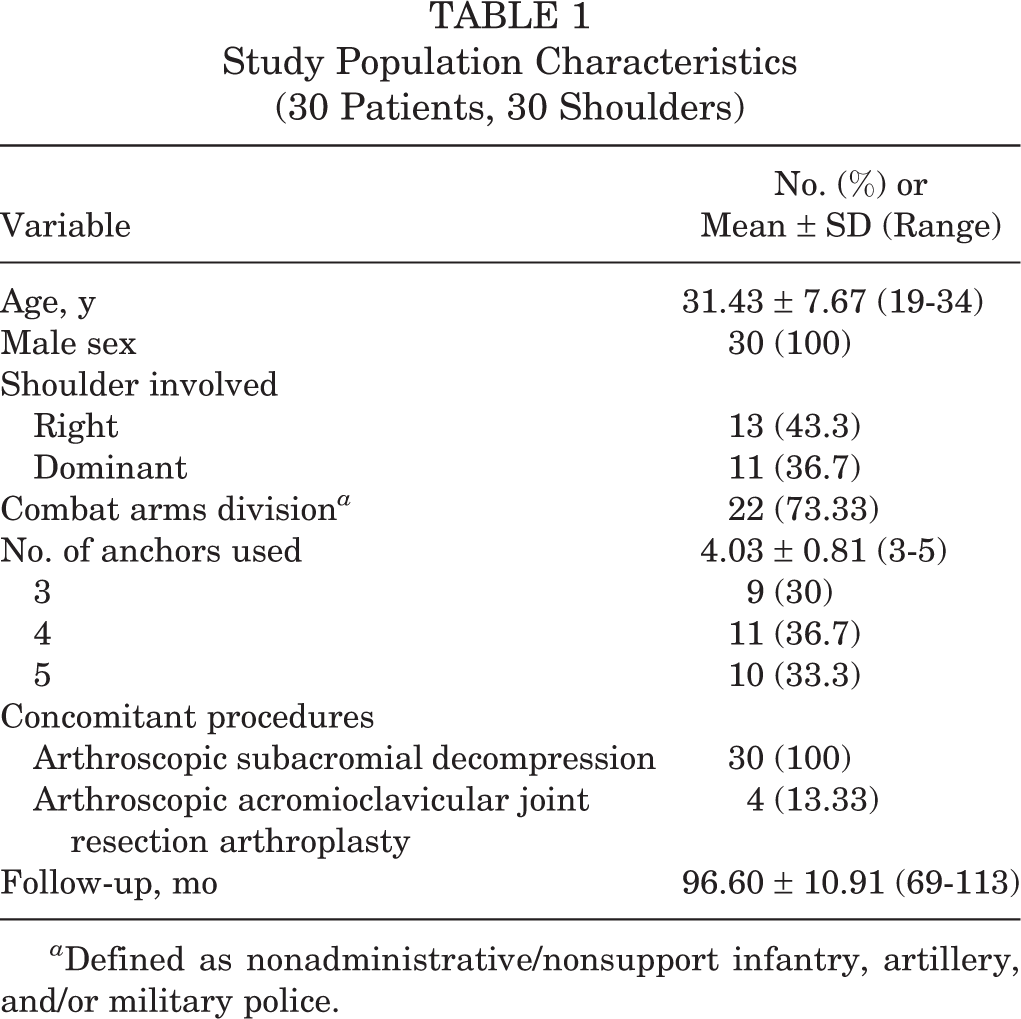
a Defined as nonadministrative/nonsupport infantry, artillery, and/or military police.
All 30 patients were active duty military at the time of surgery: 22 (73.33%) were soldiers in a combat arms military occupation specialty, and 8 were noncombat arms. Combat arms was defined as nonadministrative, nonsupport infantry, artillery, or military police. Eighteen patients served as infantry, 3 as artillery, and 1 as military police. Of the 8 patients who were noncombat arms, 2 were mechanics, 2 were food service, 1 was a computer technician, 1 was a driver, 1 was a firefighter, and 1 worked in logistics.
Regarding complications, there were no infections or nerve injuries. One patient had recurrent posteroinferior instability, 1 had a nonhealing tear, and 1 reported persistent postoperative stiffness. Altogether, the complication rate was 10%. Of the 3 patients with postoperative complications, 2 were combat arms (infantry), and the third was an armored vehicle mechanic. Only the patient with the nonhealing tear progressed to further surgery. Overall, 90% of patients remained on active duty military service and were able to return to preinjury levels of work and recreational activity.
There were significant improvements in all patient-reported outcome measures from presurgery to final follow-up (P < .0001 for all) (Table 2). There was no significant change in forward flexion, external rotation, or internal rotation between pre- and postoperative measurements. Outcome measures did not vary between patients with and without a history of trauma (Table 3).
Pre- and Postoperative Measurements a

a Values are presented as mean ± SD. Bold P values indicate statistically significant difference between pre- and postoperative (P < .05). ASES, American Shoulder and Elbow Surgeons; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale.
Outcome Measures Between Traumatic and Nontraumatic Etiologies a

a Data are reported as mean ± SD. ASES, American Shoulder and Elbow Surgeons; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale.
Discussion
The findings of this study supported our hypothesis. Arthroscopic repair of type VIII SLAP lesions in active duty military patients aged <35 years produced favorable outcomes in the majority of soldiers at midterm follow-up. Overall, 90% of patients were able to maintain active military service and had returned to preinjury levels of work and recreational activity, and only a single patient required a secondary surgical procedure.
Our results suggest that outcomes after arthroscopic repair of type VIII SLAP tears may contrast with the outcomes after repair of type II SLAP tears. While arthroscopic repair and biceps tenodesis have been used to treat type II lesions, there is growing evidence that biceps tenodesis produces higher rates of patient satisfaction and return to preinjury levels of activity, especially when performed in patients >35 years old. 7,8,11,12,15,21 As a result of these findings, the rate of performing biceps tenodesis by orthopaedic surgeons has far surpassed that of SLAP repair. 8 There is still debate, however, regarding the preferred method of treatment of SLAP type II tears in patients aged <35 years. In our practice, we prefer combined repair and tenodesis for SLAP VIII lesions for the following indications: (1) patient age >35 years, (2) a history of anterior shoulder pain in addition to physical examination findings of point tenderness over the bicipital groove and positive Speed test result, and (3) intraoperative findings of biceps tendinitis (positive lipstick sign) or partial tear of the long biceps tendon.
The patients in this study did not meet any of these criteria; therefore, we favored arthroscopic repair in this cohort. While further studies are needed to definitively establish the optimal surgical technique for management of type VIII lesions in patients <35 years old, our results demonstrate excellent functional outcomes at midterm follow-up with repair, which is comparable with published results after tenodesis for type II tears.
Our results are of particular interest given the high-demand active duty patient population comprising our study cohort. Members of the military experience a higher incidence of SLAP tears as well as posterior capsulolabral tears when compared with the civilian population. 3,4,14,31,33 This has been hypothesized to be due to the repetitive strenuous activity required by many military roles, with the high level of antecedent trauma reported by these patients. 14 Furthermore, it has been shown that active duty military patients experience higher rates of unsatisfactory outcomes after treatment of type II SLAP lesions when compared with civilian patients, likely attributable to the high physical demands endemic to this population, as well as the considerable amount of overhead shoulder use often required for active duty service. 3,10,22,27 Therefore, it is logical to assume that this trend would hold true after the treatment of type VIII lesions. In this study, arthroscopic repair of type VIII SLAP lesions provided significant improvement in pain and function. While failure rates after type II SLAP repair have been as high as 36.8% among military patients, 23 only 10% of our patients reported complications, with just 1 patient requiring a secondary surgical procedure. These findings are in line with a 2018 study by Fourman et al, 9 who cited decreased pain and increased function after repair of type VIII lesions in throwing athletes, another demographic that historically faces poor outcomes after operative management of SLAP lesions.
While it is notable that the findings of this study demonstrated lower complication rates and better functional outcomes when compared with isolated SLAP II repairs in military patients, SLAP II and SLAP VIII injuries are inherently different pathologies, and it is not implausible that the ideal surgical management of SLAP VIII tears may differ from those of SLAP II lesions. However, more research is needed to establish the optimal treatment of type VIII lesions. Furthermore, the mean length of time between injury and surgical intervention was nearly 1.5 years. Extended periods between symptom onset and treatment are common in military populations as the result of variables such as transfer between bases, deployment, and other military job requirements. 32 It is important to note that all 30 patients had positive impingement test results (Neer, Hawkins) on preoperative physical examination. Despite extended intervals between the onset of symptoms and surgical treatment, nearly all patients reported favorable functional outcomes at latest follow-up. Together, these findings support arthroscopic repair as a viable treatment option for type VIII SLAP lesions, even in patient populations that are prone to unsatisfactory outcomes.
There is conflicting evidence regarding the association between postoperative rotator cuff tears and the use of a transcuff portal. Several studies have demonstrated favorable outcomes after arthroscopic SLAP repair using the trans–rotator cuff portal. 13,18 –20,25 However, Stephenson et al 30 reported increased risk of iatrogenic rotator cuff tears after the use of an improperly placed transcuff portal. Postoperatively, none of our patients had clinical or subjective findings indicative of iatrogenic rotator cuff injury, suggesting that the use of this portal is safe when performing repair of type VIII SLAP lesions in an active duty military population.
While the minimal clinically important difference (MCID), substantial clinical benefit (SCB), and Patient Acceptable Symptom State (PASS) thresholds have not been defined for these patient-reported outcome measures after arthroscopic repair of type VIII SLAP lesions, these values have been defined for biceps tenodesis, another procedure that may be used to operatively manage SLAP lesions. 24 All patients achieved the MCID for the ASES and SANE. Additionally, all 30 patients achieved the SCB for the SANE, and 29 (96.67%) met the SCB on the ASES. Last, 29 (96.67%) patients met the PASS for the SANE and ASES (Table 4).
Patients Meeting the MCID, SCB, and PASS a
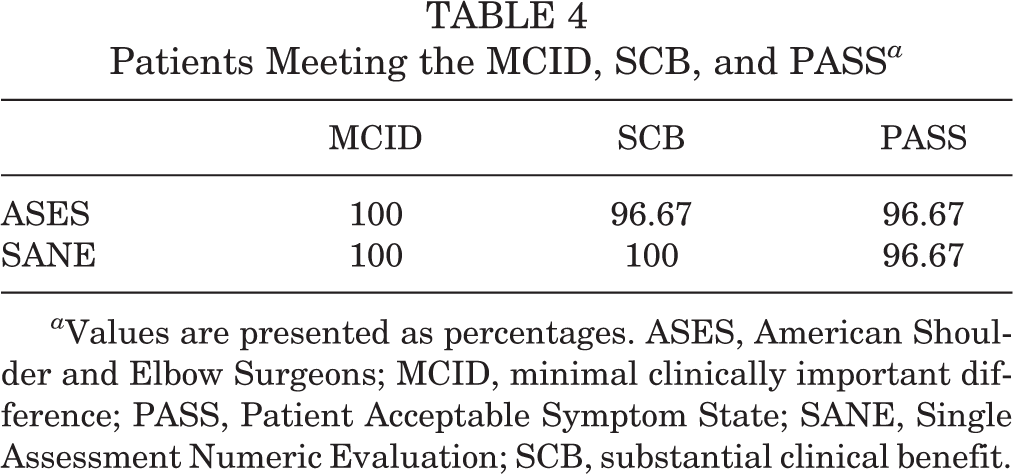
a Values are presented as percentages. ASES, American Shoulder and Elbow Surgeons; MCID, minimal clinically important difference; PASS, Patient Acceptable Symptom State; SANE, Single Assessment Numeric Evaluation; SCB, substantial clinical benefit.
Limitations
Our study was not without limitations. The retrospective nature of our investigation and limited sample size represent potential sources of bias. Additionally, our study cohort was composed entirely of active duty male servicemembers, potentially limiting the generalizability of our findings to the broader population. Last, we utilized MCID, SCB, and PASS thresholds validated for biceps tenodesis in our analysis, as these thresholds have not been established for arthroscopic SLAP repair. However, we believe that given the similar nature of these 2 procedures, it is reasonable to extrapolate these values for arthroscopic SLAP repair.
Conclusion
The results of this study demonstrated favorable outcomes for a majority of patients after arthroscopic repair of type VIII SLAP lesions at midterm follow-up, supporting repair as a viable treatment option for type VIII SLAP tears in this patient population.
Footnotes
Final revision submitted February 21, 2022; accepted February 25, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.C.D. has received hospitality payments from Stryker. N.P. has received hospitality payments from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Carson-Carthage institutional review board (2021-7).