
Abstract
Background:
The role of preoperative corticosteroid injections (CSIs) in rotator cuff repair (RCR) outcomes is controversial, with mixed evidence regarding their effect on tendon healing and postoperative recovery.
Purpose:
To control for potential variables that may affect tendon healing and to explore the effect of CSIs on tendon healing and the difference in the effect of injection frequency and time interval on outcomes.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This retrospective cohort study included 365 patients who underwent arthroscopic RCR between February 2021 and June 2023. Patients were categorized into CSI group (CSI group; n = 113) having a history of injections ≤1 year before surgery and control group (n = 252, 1 patient with bilateral shoulder involvement) without preoperative injections. Propensity score matching (PSM) was employed to reduce the effect of confounding variables, including age, body mass index, tear size, and biceps pathology, resulting in 113 matched pairs. Outcomes, including pain, shoulder function (Constant-Murley Score, Oxford Shoulder Score) were assessed at 3, 6, and 12 months postoperatively. Tendon integrity was evaluated using magnetic resonance imaging (MRI) ≥6 months postoperatively.
Results:
After PSM, baseline characteristics were balanced between the groups. At 3 months postoperatively, the CSI group exhibited significantly reduced active abduction and external rotation compared with the control group. Pain at night (visual analog scale, VAS) was also higher in the CSI group than the control group at 3 months (mean value 2.97 vs 2.31; P = .03). However, no significant differences in patient-reported outcome measures (PROMs) were observed between the 2 groups at any time point. MRI assessments of Sugaya grade at ≥6 months postoperatively revealed a higher retear rate in the CSI group compared with control (23.9% vs 8.8%; P = .02). Subgroup analysis indicated that patients who received 2 injections (OR, 3.25; 95% CI, 1.06–10.16; P = .04) or ≥ 3 injections (OR, 5.71; 95% CI, 1.87–18.28; P < .001) had a significantly higher risk of retear compared with the control group. Additionally, patients who received CSI between 3 and 6 months and <3 months before surgery also showed a significantly increased risk of retear compared with the control group (OR, 5.80; 95% CI, 2.07–17.40; P < .001 and OR, 7.25; 95% CI, 1.77–29.65; P = .01, respectively). Cross-effect analysis revealed that receiving ≥ 2 injections within ≤ 6 months before surgery was significantly associated with a higher postoperative retear risk (OR, 7.30; 95% CI, 2.83–20.76; P < .001).
Conclusion:
Preoperative CSIs, particularly when administered multiple times and within 6 months before surgery, are associated with a higher risk of retear after RCR. However, there is limited difference in range of motion and PROMs between the 2 groups.
Rotator cuff injuries are a common cause of shoulder pain and functional impairment, significantly affecting patients’ quality of life.2,10 Arthroscopic rotator cuff repair (RCR) has significantly improved the function of patients with rotator cuff injury, although retear is still an important clinical problem.1,2,18 Risk factors such as age, obesity, diabetes, tear size, degree of retraction, and muscle quality are thought to increase the incidence of retears.4,16,17,21,25,45 In addition to these patient-related characteristics, the effect of preoperative interventions, particularly corticosteroid injections (CSIs), has garnered increasing attention in recent years.8,10,33,39,43
Patients with rotator cuff tears are usually first treated with nonoperative therapies such as physical therapy (PT), nonsteroidal anti-inflammatory drugs, and/or steroid injections. 2 The utility of CSIs lies in their anti-inflammatory effects, which can alleviate pain and improve shoulder function.6,14,28 In clinical practice, CSI is frequently employed as a first-line nonoperative therapy for tendinopathy or mild rotator cuff tears, aiming to alleviate pain and improve function. 27 Research has demonstrated that CSI can significantly reduce pain in patients with rotator cuff tears within a 3-month period. 14 In spite of this, there are still many patients whose symptoms are not relieved or in fact worsen after receiving CSI, at which point patients seek surgical treatment. 2 The use of CSI in treating tendinopathy or rotator cuff disease remains controversial, with debates centered around its risks—such as tendon rupture and tissue damage—versus its benefits, including enhanced mechanical strength.9,11
As the understanding of tendinopathy deepens, concerns have been raised regarding the potential long-term deleterious effects of CSI on tendons.9,40 CSI may lead to decreased biomechanical properties of tendons, 44 altered tendon quality, 38 and deterioration of the osteotendinous junction, 26 according to previous laboratory studies. In addition, because cellular senescence is irreversible in the body, the effects of glucocorticoids on tendons may lead to long-term degenerative changes. 32 Several studies based on large databases have shown that receiving ≥ 2 injections and having an injection interval of < 6 months significantly increased the risk of reoperation following RCR.10,39,43 However, these studies lack detailed patient information, and reoperation rates do not adequately reflect tendon healing. Another study, by controlling for no injections in the 3 months before surgery, found no difference in function or structure in patients who underwent CSI 1 year before surgery at a mean follow-up of 3 years. 12 However, they had a small sample size and did not control for other confounding variables that could affect tendon healing. The influence of CSI on tendon structure and healing remains a topic of ongoing debate, with conflicting evidence in the literature. There is a notable lack of research investigating how the timing and frequency of preoperative CSI might influence functional recovery and tissue healing after RCR surgery.
The purposes of this study were to (1) control for the variables that may affect tendon healing and to explore (2) the effect of CSI on tendon healing and (3) the difference in the effect of injection frequency and time interval on outcomes. We hypothesize that multiple preoperative CSIs or those administered too close to the surgery may have an adverse effect on tendon repair.
Methods
Study Design
We prospectively collected data from 504 (1 patient with bilateral shoulder involvement) consecutive patients who were diagnosed with rotator cuff tears and underwent arthroscopic RCR at our institution between February 2021 and June 2023 (Figure 1). All patients provided informed consent, and the study was approved by the institutional review board of the Second Affiliated Hospital, Zhejiang University School of Medicine. Patients were included if they met the following criteria: (1) partial-thickness rotator cuff tear or full-thickness tear <5 cm; (2) age 18 to 80 years, regardless of sex; and (3) preoperative and postoperative magnetic resonance imaging (MRI) available for ≥6 months. Exclusion criteria were (1) massive rotator cuff tear ≥5 cm; (2) fractures of the greater tuberosity of the humerus, clavicular fractures, or glenoid bony structural damage; (3) history of previous surgery on the ipsilateral shoulder; and (4) CSI performed by other clinics or hospitals.

Patients enrollment flowchart. CSI, corticosteroid injection.
Records of outpatient treatment history were obtained from our clinical system. We retrospectively examined patients who received CSI preoperatively. Preoperative CSI was defined as any outpatient subacromial injection administered ≤1 year before surgery at our institution, with no injections performed at other facilities. We recorded the number of injections within the year before surgery and the interval from the most recent injection to the surgery date. Patients were categorized into 2 groups based on the presence or absence of preoperative CSI ≤1 year before surgery: the CSI group and the control group.
Subacromial Injection
After outpatient evaluation, patients were directed toward either structured PT or subacromial injections with PT based on their symptoms and the severity of the tear first. Generally, patients with mild tears (partial tears or tear size ≤1 cm) or tendinopathy and significant pain were more likely to receive subacromial injections, while those with less severe symptoms were prioritized for structured PT. For patients with larger tears, surgery was the primary choice; however, those experiencing significant pain that affected their daily life were administered a single subacromial injection during the waiting period before surgery. All subacromial injections were performed by an orthopaedic surgeon (D.R.) using a combination of 7 mg betamethasone, 2 mL 2% lidocaine. The injections were administered via the posterior approach under the acromion. After the injection, patients were observed in the outpatient clinic for 20 minutes to monitor any adverse reactions. Patients receiving CSI were scheduled for a second steroid injection ≥4 weeks apart if needed. The main factors for a second injection were concurrent frozen shoulder, inadequate symptom relief, and lack of immediate surgical options.
Identify Confounding Variables and Propensity Score Matching
To account for potential confounding factors affecting the outcomes beyond preoperative CSI, we employed logistic regression to identify other variables that might influence prognosis. Propensity score matching (PSM) was then used to control for these confounders. PSM is a statistical method used to control bias and achieve pseudorandomization in retrospective observational studies by balancing covariates between groups. 3 We identified key prognostic factors—age, body mass index (BMI), tear size, degree of tendon retraction, and long head of the biceps tendon (LHBT) pathology—and performed 1:1 matching with the control group based on the propensity scores. The propensity scores were estimated using multiple logistic regression with CSI as the dependent variable. The model included age, BMI, tear size, and LHBT pathology as covariates. Nearest Neighbor Matching, the most common matching algorithm, is used for patients in the matching treatment group whose propensity score distance is closest to the patients in the matching treatment group. 15 The standard algorithm is generally “greedy” matching. Greedy matching was conducted with a caliper width of 0.2 SD. The balance between groups was assessed using absolute standardized differences, with all values after matching being <0.1 (Supplemental Table S1). PSM was conducted using R Version 4.3.1 (RStudio) with the MatchIt R package.
Surgical Technique and Rehabilitation
All surgeries were performed by a senior author (W.S.) with the patient positioned at a 70° incline in the beach-chair position under general anesthesia. A systematic exploration of the subacromial space, rotator cuff interval, glenohumeral joint, biceps tendon, and condition of the rotator cuff was conducted. For biceps tendon injuries or pathology, the decision between tenotomy and tenodesis was made based on the patient's age and daily activity level. The thickness of the rotator cuff tear (partial-thickness tear or full-thickness tear) was observed arthroscopically. The decision to use either single-row or double-row repair technique was guided by the extent of tendon retraction and the tear pattern. Subacromial decompression was performed to create a flat acromion when there was an indication of bone spurs or wear on the undersurface of the acromion. Postoperatively, the arm was immobilized in a sling. Pendulum exercises and hand movements were initiated on the first day after surgery. Passive forward flexion stretching began at 2 weeks. The sling was removed at 4 weeks postoperatively, and passive range of motion (ROM) exercises were resumed. Active-assisted exercises were permitted after 12 weeks. Patients were followed up in the outpatient clinic at 4, 8, and 12 weeks postoperatively, with the rehabilitation plan adjusted as needed based on their recovery progress.
Data Collection and Evaluation
Clinical Data
Preoperatively, baseline demographic data, shoulder ROM, pain levels, and functional scores were collected from each patient. Follow-up assessments were conducted during outpatient visits at 3, 6, and 12 months postoperatively. ROM, including forward flexion, abduction, internal rotation, and external rotation, was measured with a goniometer while the patient was seated. Pain levels were evaluated using the visual analog scale (VAS) (0-10, where 0 indicates no pain and 10 indicates severe pain) during rest, sleep, and activity. Shoulder function was assessed using the Constant-Murley score 7 (CMS) and the Oxford Shoulder Score 30 (OSS). The assessment of ROM and muscle strength was conducted by a trained clinical assistant who was blinded to the patients’ medical history. Pain scores and functional scores were self-reported by the patients.
Radiological Data
Preoperatively, all patients underwent MRI to assess the condition of the shoulder. The width of the rotator cuff tear was measured based on the method as described, defined as the maximal width on the oblique sagittal view. 20 Retraction grading was classified according to the Patte classification 31 as follows: grade 1, retraction to the footprint; grade 2, retraction to the humeral head; and grade 3, retraction to the glenoid level. Muscle atrophy on the oblique sagittal view was also assessed based on the description by Warner et al. 41 Postoperative MRI was routinely performed at our institution ≥6 months after surgery to evaluate tendon integrity and assess for retear. Retears were defined as Sugaya grades 4 to 5 according to the criteria described by Sugaya et al. 36 Additionally, muscle atrophy, rotator cuff tendon signal, and retear type were evaluated. The tendon signal-to-noise ratio22,23 (SNQ) was measured in 2 regions: proximal (SNQ-p; at the musculotendinous junction and above the humeral head) and distal (SNQ-d; at the suture anchor repair site, with background signal measured at the supraclavicular region). Retear types 5 were classified as type 1 (occurring at the tendon-bone interface) and type 2 (occurring medially within the tendon). Radiographic evaluations were performed by 2 orthopaedic surgeons (D.R. and H.L.) who were blinded to the patients’ clinical information, with the exception of essential imaging parameters required for the assessment.
Statistical Analysis
Before performing PSM, t tests were used to analyze continuous variables between the 2 groups, and chi-square tests were used for categorical variables. Binary logistic regression was employed to assess the effect of different variables on the outcomes, aiming to identify potential confounders. After PSM, paired t tests were used to analyze continuous variables between the 2 groups, and McNemar test was used for categorical variables.
Intergroup variable analysis and logistic regression were performed in R Version 4.3.1 (RStudio). Statistical significance was set at P < .05. It was determined that a minimum of 94 patients would be required to detect a 20% difference in retear rates (from 15% to 35%) with a statistical significance level of P < .05 and a statistical power set at 0.90. Due to the multiple time point follow-up design, some time points had incomplete data. The specific details are provided in Supplementary Table S2. Because the proportion of missing data did not exceed 8%, we retained the original data without exclusion to maximize data utilization.
Results
Baseline Characteristics and PSM
Before PSM, the control group (n = 253) and the CSI group (n = 113) showed significant differences in key variables. Specifically, the control group demonstrated a larger tear size (14.49 mm vs. 12.20 mm; P = .046), a higher proportion of patients with trauma history (49.8% vs. 35.4%; P = .01), and lower visual analog scale scores both at rest (2.05 vs. 2.43; P = .006) and during activity (3.87 vs. 4.33; P = .005) compared to the CSI group. To identify other factors that may influence retear, univariate logistic regression showed that BMI, age, tear size, tear type, tendon retraction grade, and lesion of the biceps were potential confounding variables (Figure 2). After PSM, in each group, 113 patients were matched for the analysis. Besides, the baseline characteristics were well-balanced between the 2 groups, with no significant differences in age, BMI, tear size, lesion of the biceps (all standardized difference <.01) (Figure 3), ensuring that the subsequent comparisons were not biased by these factors (Table 1). The mean number of injections was 1.92 ± 1.04 times and the mean injection interval was 6.10 ± 2.70 months. This matching process confirmed that the groups were comparable, allowing a more accurate assessment of the effect of CSI on postoperative outcomes.

Forest plot displays the odds ratios (ORs) with 95% CI for various factors influencing the retear. Each row corresponds to a different variable, with the sample size (N), OR, confidence interval, and P value provided. The blue squares represent the point estimates of the ORs, and the horizontal lines denote the confidence intervals. If the confidence interval of a variable does not cross the null hypothesis line (1.0), it indicates statistical significance. An OR >1.0 suggests that the factor may be a risk factor for the outcome, while an OR value <1.0 suggests that the factor may be a protective factor. Factors such as age, tear size, tear type, Patte classification, and biopsy type show significant associations with the outcome, as indicated by their ORs and P values. BMI, body mass index.

The figure illustrates the covariate balance assessment, comparing standardized mean differences of covariates before (unadjusted) and after (adjusted) matching. The x-axis represents the magnitude of standardized mean differences, and the y-axis lists the covariate names. Red dots indicate unadjusted samples, and blue dots represent adjusted samples after matching. The results show that, after matching, the standardized mean differences for most covariates are significantly reduced and approach zero, indicating that the matching process effectively balanced the covariate distributions between groups and minimized potential confounding bias. BMI, body mass index; Biceps_0, without intervention; Biceps_1, tenodesis; Biceps_2, tenotomy.
Preoperative Comparison Between CSI and Control Groups Before and After Propensity Score Matching a
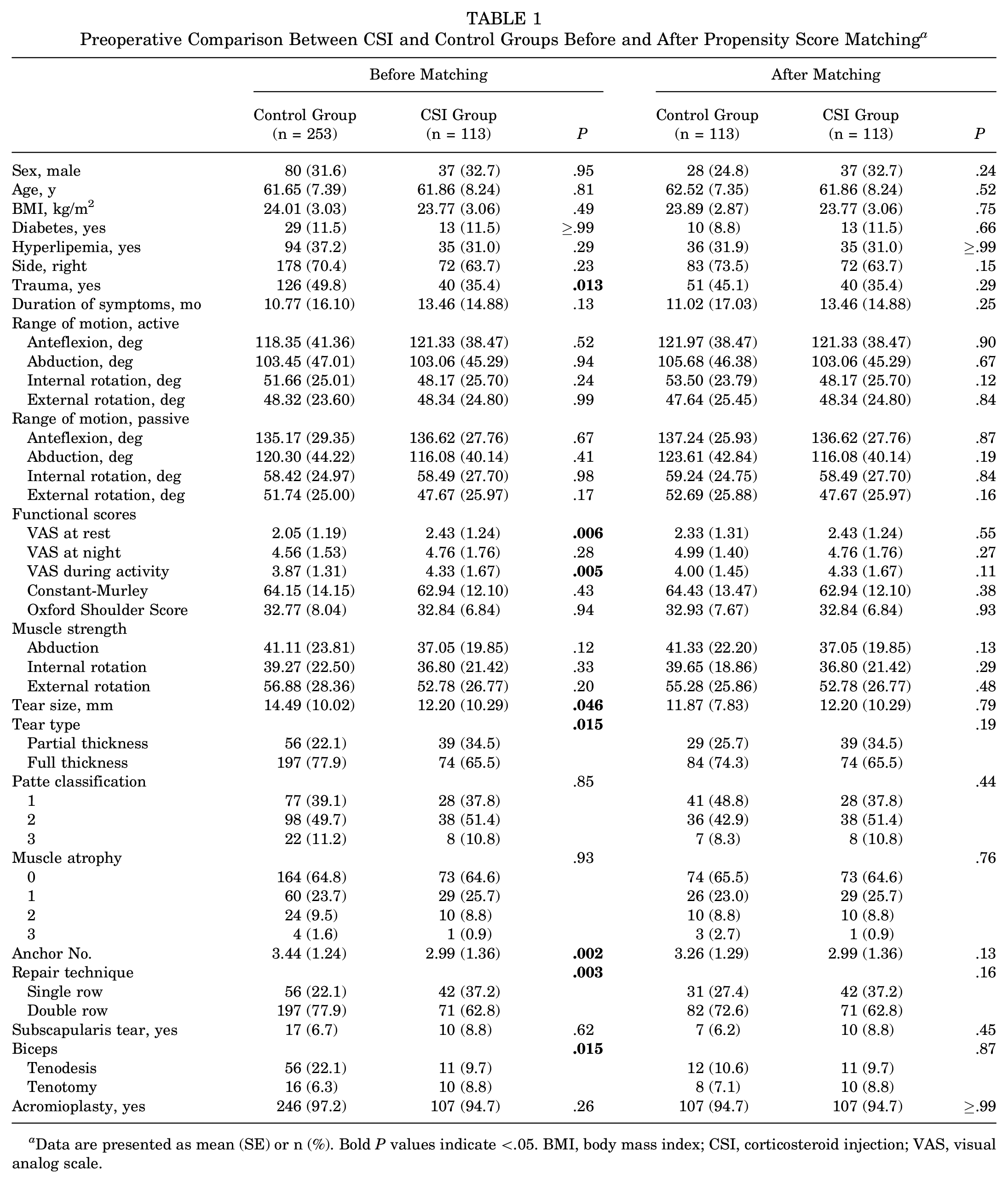
Data are presented as mean (SE) or n (%). Bold P values indicate <.05. BMI, body mass index; CSI, corticosteroid injection; VAS, visual analog scale.
Functional Outcomes and Pain
At 3 months postoperatively (Table 2), the CSI group exhibited significantly lower active abduction (101.04° vs 118.18°; P = .03) and external rotation (40.74° vs 49.27°; P = .02) compared with the control group. Pain levels, measured by the VAS at night, were also higher in the CSI group than the control group at 3 months (2.97 vs 2.31; P = .03). By 6 months (Table 2), the difference in external rotation between the CSI group and control group persisted (48.10° vs 54.07°; P = .048), but other functional differences began to diminish. At 12 months (Table 2), no significant differences were observed in ROM or functional scores (CMS, OSS) between the groups, indicating a convergence in functional recovery over time. The baseline characteristics of patients stratified by CSI frequency and timing are shown in Supplementary Tables S3 and S4, respectively.
Clinical Outcomes for 2 Matched Groups a
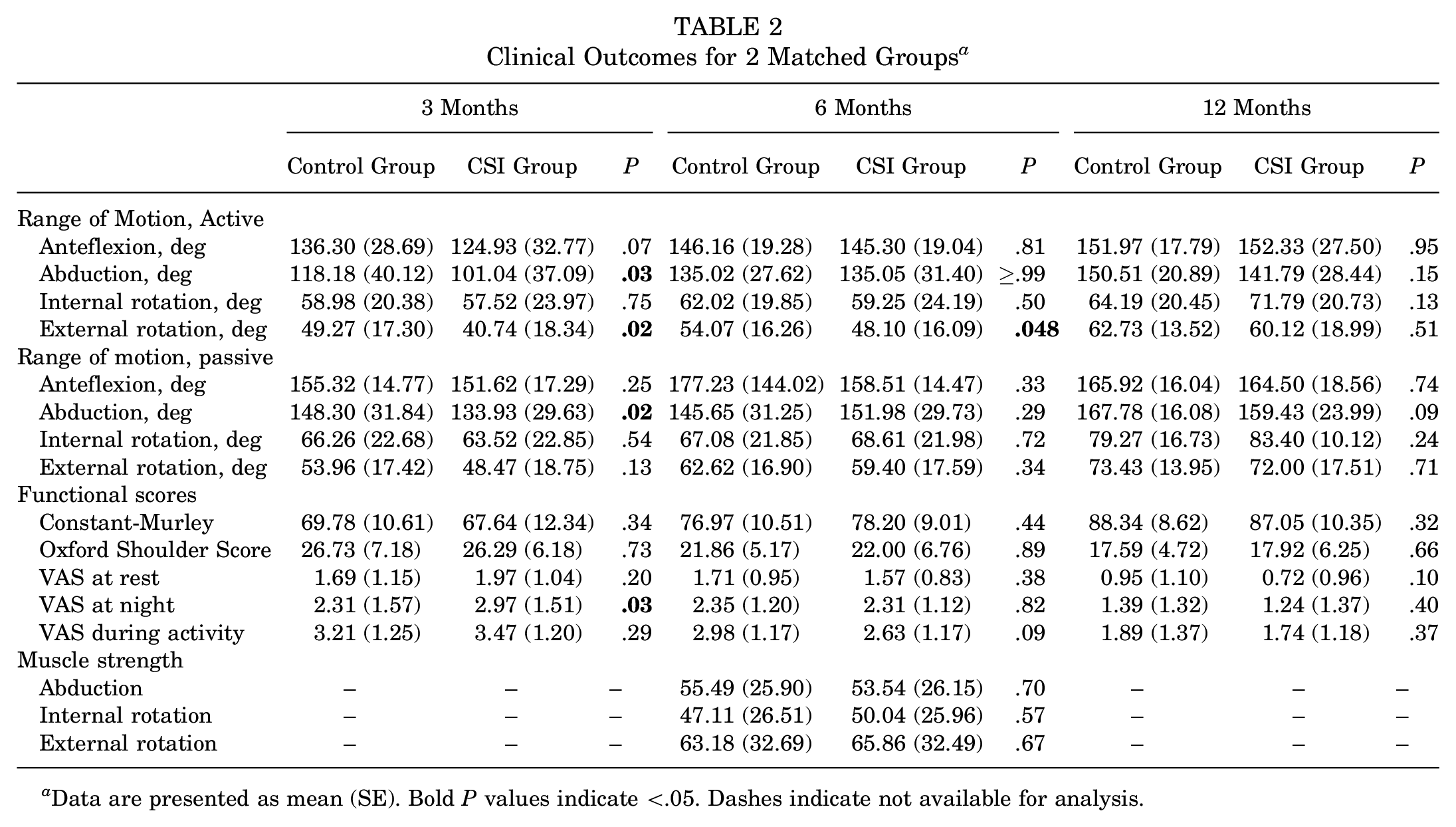
Data are presented as mean (SE). Bold P values indicate <.05. Dashes indicate not available for analysis.
MRI Findings
MRI evaluations (Table 3) conducted ≥6 months postoperatively revealed a significantly higher retear rate in the CSI group compared with the control group (23.9% vs 8.8%; P = .02). Retears in the CSI group were more frequently classified as Sugaya grade 4 or 5, reflecting worse tendon healing. There was no significant difference in muscle atrophy between the 2 groups (P > .05). In addition, there was no significant difference in tendon signal between the 2 groups for patients without retearing (Sugaya grades 1-3) (mean ± SE SNQ-d: 20.60 ± 11.24 vs 20.95 ± 9.69, P = .84; SNQ-p: 13.97 ± 7.68 vs. 14.42 ± 7.47, P = .71). No difference in tear pattern was found in patients with retear (type 1/type 2: 40.0%/60.0% vs 40.7%/59.3%; P = .97).
MRI Findings for Tendon Integrity and Quality a

Data are presented as mean (SE) or n (%). CSI, corticosteroid injection; MRI, magnetic resonance imaging; SNQ, signal-to-noise ratio.
The denominator here is the number of patients with retear, specifically 10 in the control group and 27 in the CSI group.
Subgroup Analysis
Subgroup analysis revealed a significant dose-response relationship between the frequency and timing of preoperative CSI and tendon retear rates. Patients receiving 2 injections had a higher retear rate compared with the control group (23.68% vs 8.85%; odds ratio [OR], 3.246; P = .04), while those with ≥3 injections had the highest retear rate (37.04% vs. 8.85%; OR, 5.705; P < .001) (Table 4). Timing also mattered: injections within 3 to 6 months before surgery increased retear rates (36.84% vs 8.85%; OR, 5.796; P < .001), and those within 3 months led to a dramatically higher rate (41.18% vs 8.85%; OR, 7.245; P = .01). However, cross-analysis of timing and frequency revealed that only patients who received multiple injections and had a surgery-to-injection interval of <6 months exhibited a significantly higher retear rate compared with controls (40.82% vs 8.85%; OR, 7.303; P < .001).
Risk of Retear Stratified by Frequency and Period of Preoperative Injections a

Bold P values indicate < .05.
Group 0, no injections at all; group 1, injection performed >6 months before surgery, with 1 injection; group 2, 1 injection, but interval between injection and surgery was ≤6 months; group 3, injection performed >6 months before surgery, but with >1 injection; group 4, >1 injection, and interval between injection and surgery was <6 months.
Discussion
By controlling for a number of potential risk variables, this study found that preoperative CSI may have an adverse effect on postoperative tendon healing. To control for other variables that could affect tendon healing, we employed PSM to balance preoperative and intraoperative differences. The results showed that the CSI group experienced slightly more pain, as well as slower recovery in abduction and external rotation at 3 months postoperatively, with reduced external rotation still evident at 6 months, although these differences were no longer observed at 12 months. Additionally, the CSI group had a significantly higher retear rate, with subgroup analysis indicating that receiving ≥2 injections and having an injection interval of <6 months significantly increased the risk of retear.
Evaluation of outcomes after rotator cuff injury is mainly divided into patient-reported functional outcomes and structural outcomes determined by MRI. CSI is believed to alleviate pain and improve function in rotator cuff disease. A systematic review of randomized trials comparing corticosteroid injections with other injectable therapies for tendinopathy concluded that while there is robust evidence supporting the short-term efficacy of CSI, its benefits diminish in the medium to long term relative to other treatments. 6 Despite the clinical benefits observed in some patients, which may even preclude the need for surgical intervention, a subset of patients experiences no significant improvement after CSI, ultimately requiring surgery. It is possible that symptom relief from CSI gave patients a false sense of full recovery, prompting increased shoulder activity and loading, which may have led to symptom recurrence or disease progression once the corticosteroid effects waned. As the understanding of tendinopathy deepens, concerns have been raised regarding the potential long-term deleterious effects of CSI on tendons.9,40 This raises a critical question: does preoperative CSI influence functional outcomes and structural healing in patients who undergo RCR? The primary therapeutic goal of CSI in rotator cuff injuries is to relieve pain and improve function, but it may also have implications for tendon structure and cellular function.11,28,32,34 While many patients in our clinical practice experienced significant pain relief after CSI, some showed disease progression or symptom recurrence, ultimately necessitating surgery. Postoperative outcomes in these patients indicated inferior short-term shoulder ROM and higher pain levels compared with the control group. Nevertheless, these differences (at 3 months postoperatively, the CSI group showed 17° less abduction, 9° less external rotation, and 0.66 points higher nighttime VAS compared with the control group; at 6 months postoperatively, the CSI group showed 6° less external rotation) may not reflect clinically significant functional differences. According to previous studies, 37 a VAS difference of >1.4 points is required to reach the minimal clinically important difference, suggesting that the observed minor differences are unlikely to indicate meaningful functional recovery, especially given the absence of differences in functional scores (CMS and OSS). The question of whether CSI affects mid- to long-term functional recovery after RCR remains to be explored in future studies.
On the other hand, structural outcomes are also important indicators of average RCR outcomes, and previous studies have shown the potential negative effects of corticosteroids on tendon healing, but lack control for other potential factors. Numerous studies have focused on reducing retear rates after RCR, and factors influencing tendon healing have been extensively investigated.2,4,24,35,42 As a degenerative condition, rotator cuff tears are closely associated with age, with older patients being more susceptible to both occurrence of rotator cuff tears and postoperative retear.2,27 Moreover, metabolic conditions such as diabetes4,35 and obesity 42 are recognized as important factors affecting tendon healing. Patient-specific structural characteristics, such as tear size, tendon retraction, and muscle quality, may also influence tendon healing outcomes after RCR. 2 Before evaluating the effects of CSI on tendon healing, it is essential to control confounding variables. In our cohort, regression analysis identified older age, higher BMI, tear type, greater tear width, significant tendon retraction, and pathology of the LHBT as risk factors for retear, consistent with previous findings in the literature. Given the significant positive correlation between tear width, tear type, and tendon retraction, we employed PSM to control for age, BMI, tear width, and LHBT pathology.
The timing and frequency of CSI may be key factors affecting tendon healing. A systematic review investigating the use and efficacy of corticosteroid injections for various sports injuries identified tendon and fascial ruptures as the most commonly reported complications. 29 Additionally, 2 large-scale database studies explored the relationship between the frequency and timing of preoperative steroid injections and the rate of reoperation after RCR. The findings indicated that a single injection with an interval of >6 months before surgery did not significantly affect reoperation rates, while multiple injections or shorter intervals significantly increased the risk of retear.10,19 However, one must consider the inherent limitations of large database studies, such as the inability to control for specific preoperative surgical details and disease severity. A recent meta-analysis aimed at identifying risk factors for retear confirmed that CSI is a significant risk factor, independent of injection frequency and timing. 8 On the other hand, another study suggested that patients who underwent surgery ≤3 months of CSI did not exhibit significant differences in postoperative function or structural integrity compared with those who did not receive CSI. 12 However, it is important to note that this study included only 31 patients with preoperative CSI and did not account for other variables that could potentially affect tendon healing. To accurately assess the effect of CSI, it is crucial to control factors that might influence tendon healing and conduct more detailed subgroup analyses. Our study concludes that patients receiving preoperative CSI exhibit poorer structural integrity, although no significant differences in functional outcomes at final follow-up were observed. This finding aligns with previous concerns that CSI might have a detrimental effect on tendon healing.10,13 Despite the occurrence of retears, clinical function may not be immediately compromised by structural differences, necessitating longer follow-up to assess the potential for increased reoperation rates. Subgroup analysis revealed that single injection and/or surgery interval >6 months was not associated with differences compared with the control group, whereas multiple injections and/or <6-month intervals significantly elevated the risk of retear. Nevertheless, the cross–subgroup analysis of timing and frequency revealed a distinct pattern: only patients who received multiple CSIs and had injections administered ≤6 months before surgery demonstrated a significantly increased risk of retear. However, to our knowledge, no previous studies have concurrently analyzed the combined effects of injection timing and frequency, despite existing evidence suggesting that either factor alone may contribute to adverse structural outcomes.10,43 Further in vitro studies may be warranted to elucidate the potential mechanisms underlying this phenomenon. When considering surgical intervention for patients with rotator cuff injuries or deteriorating tendinopathy treated nonoperatively with CSI, clinicians should not only assess disease severity but also weigh the potential adverse effects of preoperative CSI.
The effects of corticosteroids on tendons are not solely limited to structural integrity; potential alterations in cellular function and the local microenvironment should also be considered. To investigate these potential changes, we utilized MRI to assess tissue structure indirectly, measuring tendon integrity, muscle status, tendon signal values, and retear types. As described by Cho et al, 5 type 1 retear, occurring at the tendon-anchor suture site, may reflect tendon-bone healing. However, in our study, no significant differences in retear types were observed between the groups, possibly due to the low retear rate in the control group. Tendon signal values can reflect tendon quality, with higher signal values potentially indicating pathological states or poor healing. 23 By using the SNQ, we minimized background signal interference when measuring tendon signals at the tendon-bone junction and the superior humeral head to explore potential differences in tendon quality related to CSI. 22 Our results showed no significant differences in tendon signal values between the 2 groups, which may suggest that microenvironmental or molecular changes are not accurately reflected by MRI signal values. Additionally, no differences in muscle quality were observed between the groups. Further research is needed to explore how CSI influences tendon structure and tissue healing.
Limitations
Several limitations should be acknowledged. First, due to the retrospective design of this study, certain variables such as psychosocial factors, economic status, and occupational type and so on were not included in the analysis. Future studies are needed to comprehensively evaluate these factors. Second, although we conducted follow-ups for ≥6 months postoperatively for imaging, this duration may not be sufficient to capture all long-term changes related to tendon healing, particularly in detecting chronic retears. Additionally, the sample size and single-center design may limit the generalizability of our findings, especially across different patient populations and clinical settings. To address the potential variability in injection methods, it is important to note that the timing of each injection may vary among patients due to differences in their clinical symptoms. This variability in preoperative injection intervals could introduce bias into the results. Although each matched group included 113 patients, subgroup analyses inevitably involved smaller sample sizes, potentially limiting the statistical power to detect differences accurately. Finally, while MRI is the standard method for assessing tendon integrity, it has inherent subjectivity and technical limitations, which could affect the evaluation of retear rates. Future prospective multicenter studies with larger sample sizes are needed to further validate these findings and improve preoperative management strategies.
Conclusion
In conclusion, this study found that preoperative corticosteroid injections, particularly multiple injections and those ≤6 months before surgery, significantly increase the risk of tendon retear after RCR. These findings highlight the need for careful timing and limitation of injections in patients considering surgery after failed nonoperative treatment. Clinicians should weigh the benefits of symptomatic relief against the potential risks when planning surgical interventions.
Supplemental Material
sj-docx-1-ojs-10.1177_23259671251360366 – Supplemental material for Multiple Injections and Injections ≤6 Month Injections Before Rotator Cuff Repair May Increase the Risk of Retear: A Propensity Score–Matched Study
Supplemental material, sj-docx-1-ojs-10.1177_23259671251360366 for Multiple Injections and Injections ≤6 Month Injections Before Rotator Cuff Repair May Increase the Risk of Retear: A Propensity Score–Matched Study by Xinji Wang, Hengzhi Liu, Canlong Wang, Dengfeng Ruan and Weiliang Shen in Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgements
We thank our clinical assistant, Ma Jing, for her outstanding contributions to data collection and patient evaluation.
Final revision submitted April 12, 2025; accepted April 23, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by the NSFC grants (No. 82372376), Zhejiang Lingyan project (No. 2024C03207), Zhejiang Provincial Program for the Cultivation of High-Level Innovative Health Talents, Dr Li Dak Sum & Yip Yio Chin Regeneration Medicine Foundation, and the Key R&D Program of Zhejiang (No. 2024C03077). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Second Affiliated Hospital, Zhejiang University School of Medicine (approval No. 2020LSYD080).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.