
Abstract
Background:
Early formation of muscle edema after rotator cuff injury has previously been demonstrated in an animal model.
Purpose:
To describe the same phenomenon in humans through analysis of rotator cuff muscle edema on magnetic resonance imaging/arthrography (MRI/MRA).
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Demographic, clinical, and radiological characteristics of patients with both a history of trauma and clear muscle edema of the rotator cuff were analyzed. Two groups were established based on the degree of concomitant fatty infiltration: (1) an acute group with little to no fatty infiltration of the rotator cuff muscle, and (2) an acute-on-chronic group with significant presence of fatty infiltration.
Results:
Of the 71 shoulders, 45 (63.4%) were identified as acute lesions and 26 (36.6%) as acute-on-chronic lesions. Patients in the acute group were younger (60 ± 11 years [range, 38-83 years] vs 68 ± 11 years [range, 52-90 years]; P = .006) and received earlier MRIs compared with patients in the acute-on-chronic group (23 ± 21 [range, 0-87) vs 42 ± 40 [range, 4-179]; P = .019). No other radiological characteristics studied—such as edema location, lesion type, tendon retraction, and other radiological signs—were able to distinguish the groups.
Conclusion:
Muscle edema of retraction helps to distinguish new traumatic rotator cuff injury from acute extensions of preexisting lesions via fatty infiltration and age at presentation. The difference in time between symptom onset and MRI/MRA is also a discriminating factor.
There are several known causes of muscle edema—including trauma, denervation, inflammation, neoplasia, and infection.4,15,17 Muscle edema is a phenomenon worth understanding because of its advantageous characteristic of early manifestation in disease. Indeed, while muscular atrophy and fatty infiltration occur in the subacute and chronic phases of rotator cuff lesions,9,24 muscle edema of the rotator cuff can reflect the acute and traumatic nature of an injury, its prognosis, and even dictate the timing of potential surgery. Its onset may mistakenly resemble fatty infiltration of the cuff muscles, 23 casting doubt on the repairability of certain lesions.
Apart from experimental animal studies, the description of muscle edema is scarce. This paucity of information concerning human muscle edema is due either to its uncommon nature or, more conceivably, to difficulties in obtaining timely and appropriate imaging of rotator cuff lesions. 14 Previous studies conducted on sheep have described the characteristics of a particular type of muscle edema aptly named “retraction edema” because of its association with the acute retraction of the rotator cuff tendon.12,22
This study aimed to analyze the different characteristics of patients with rotator cuff muscle edema on magnetic resonance imaging/arthrography (MRI/MRA). We hypothesized that muscular rotator cuff edema would typically appear in young patients, often after an adequate trauma, and would no longer be detectable after a few months. Additionally, it could also signal an acute extension of a preexisting lesion.
Methods
Study Design and Patient Selection
Patients >18 years seen by the senior author (A.L.) with a history of retracted (a condition where the tendon has pulled back or receded from its normal attachment site on the bone, creating a gap) traumatic full-thickness rotator cuff tear and muscle edema visible on MRI or MRA were considered for inclusion between December 2017 and February 2023. In our country, trauma is defined by strict medical (demographic, clinical, factorial, radiological, and intraoperative) criteria, based not on medical or patient judgment, but solely on a legal and neutral analysis of these criteria.13,18 The following 5 conditions must be satisfied: (1) the trauma must result from an external agent (cannot be self-inflicted); (2) be harmful; (3) sudden; (4) involuntary; and (5) extraordinary (cannot be part of a usual activity). 3 The exclusion criteria were as follows: (1) previous shoulder surgery; (2) chronic dislocation; (3) radiological signs of fracture of the glenoid or the greater or lesser tuberosities; (4) rotator cuff arthropathy with glenohumeral osteoarthritis and superior migration of the humeral head; (5) previous corticoid infiltration within 3 months; (6) immune system compromise; (7) pregnancy; (8) anticoagulation therapy; (9) tumor; (8) active infections; (10) proven suprascapular nerve lesion or Parsonage-Turner syndrome; (11) myositis (polymyositis and dermatomyositis); (12) psychiatric problems that precluded informed consent or inability to read or write; and (13) incomplete documentation.
An initial analysis revealed that muscle edema can present itself in 2 ways: (1) isolated or (2) accompanied by fatty infiltration. Having previously established edema as an acute phenomenon with early manifestation,12,23 we were able to conclude that traumatic lesion of the rotator cuff may indeed coexist with degenerative lesions and that these lesions may be considered as acute-on-chronic. Thus, the included patients were divided into 2 groups based on the fatty infiltration stages as determined by MRI/MRA. Those with muscle edema and concomitant low-grade fatty infiltration (Goutallier stages 0 to 2; n = 54 patients, acute group) were compared with those with muscle edema and high-grade fatty infiltration (Goutallier stages 3 and 4; n = 22 patients, acute-on-chronic group). 10 The latter corresponds to an acute extension of a chronic lesion associated with an adequate (hurtful) trauma.
Institutional Review Board
Data were extracted from a prospective rotator cuff database (Follow Health), the use of which had been previously approved (Association des 5édecins du canton de Genève et société médicale #12-26). All patients have been included in various research protocols approved by the local ethical committee (CCER 2015-15 trial registration number NCT02725346; CCER 2016-00818 trial registration number NCT02943005; 2019-02076 trial registration number NCT04321005) 2 and provided written informed consent for their participation and the use of their data and images for research and publishing purposes.
Study Variables
The primary outcome was the different characteristics of rotator cuff muscle edema in humans on MRI/MRA in a specialized consultation. Secondary outcomes included the time between trauma and the date of MRI/MRA, as well as the presence of fatty infiltration. In addition, the following baseline characteristics were assessed: age, sex, shoulder side, limb dominance, and shoulder active range of motion (ROM). Patient-reported outcome measures included the pretreatment Constant score, the Single Assessment Numeric Evaluation (SANE), and the pain score.
Clinical Examination
Patient’s ROM was recorded preoperatively by independent evaluators who were not part of the present study, under the supervision of the senior author (A.L.), ensuring the reproducibility of the results. Active anterior elevation and external rotation in 0° of abduction were assessed with a goniometer in the upright position. Internal rotation behind the back was estimated to the nearest spinal level and noted on a 20-level scale ranging from 0 points (thigh) to 19 points (T1 thoracic spine). Pseudoparalysis was defined 7 as an active scapular plane abduction below 45°, and pseudoparesis as an active scapular plane abduction between 45° to 90°.
Radiological Evaluation
The images were reviewed by both a musculoskeletal radiologist (F.C.K.) and 2 fellowship-trained shoulder surgeons (J.Z. and A.G.), noting the localization of edema seen on T2 images. Muscle edema was defined as hyperintense signals of the affected muscle on T2-weighted MRI sequences. Massive full-thickness rotator cuff lesions were classified according to the Collin classification. 5 Musculotendinous retraction was evaluated with the Patte classification, 19 applied on sequences in the frontal plane: stage 0, no retraction; stage 1, proximal stump near the bony insertion; stage 2, the proximal stump at the level of the humeral head; and stage 3, proximal stump at the level of or more proximal to the glenoid. Fatty infiltration of the rotator cuff muscles were reviewed with MRI/MRA in T1 images, using the 5-stage grading system according to Goutallier et al 10 : grade 0, no fatty deposit; grade 1, some fatty streaks; grade 2, more muscle than fat; grade 3, as much muscle as fat; and grade 4, less muscle than fat. The presence of a distal thickening of the supraspinatus tendon (cobra sign) and a ruptured supraspinatus tendon stump on the greater tuberosity was analyzed. 8
Statistical Analysis
The Shapiro-Wilk test was used to check the normality of distributions. Descriptive statistics were presented in terms of means, standard deviations, medians, and ranges. For normally distributed quantitative data, the significance of intergroup differences was determined using the unpaired Student t test. Conversely, for non-normally distributed quantitative data, the significance of intergroup differences was determined using the Wilcoxon rank-sum test. A chi-squared test was used to determine the significance of intergroup sex differences. Statistical analyses were performed using R Version 3.6.2 (R Foundation for Statistical Computing). P < .05 was considered statistically significant.
Results
A total of 90 shoulders satisfied the inclusion criteria in the time frame selected, and 19 (2.1%) were excluded for concomitant pathologies (arthrosis and fracture) and an absence of traumatic event upon re-review (Figure 1). The final cohort was composed of 71 shoulders, of which 45 (63.4%) were identified as acute lesions (Figure 2) and 26 (36.6%) as acute-on-chronic lesions (Figure 3).

A flow chart of study recruitment. Groups were differentiated based on fatty infiltration stage according to Goutallier et al 10 .
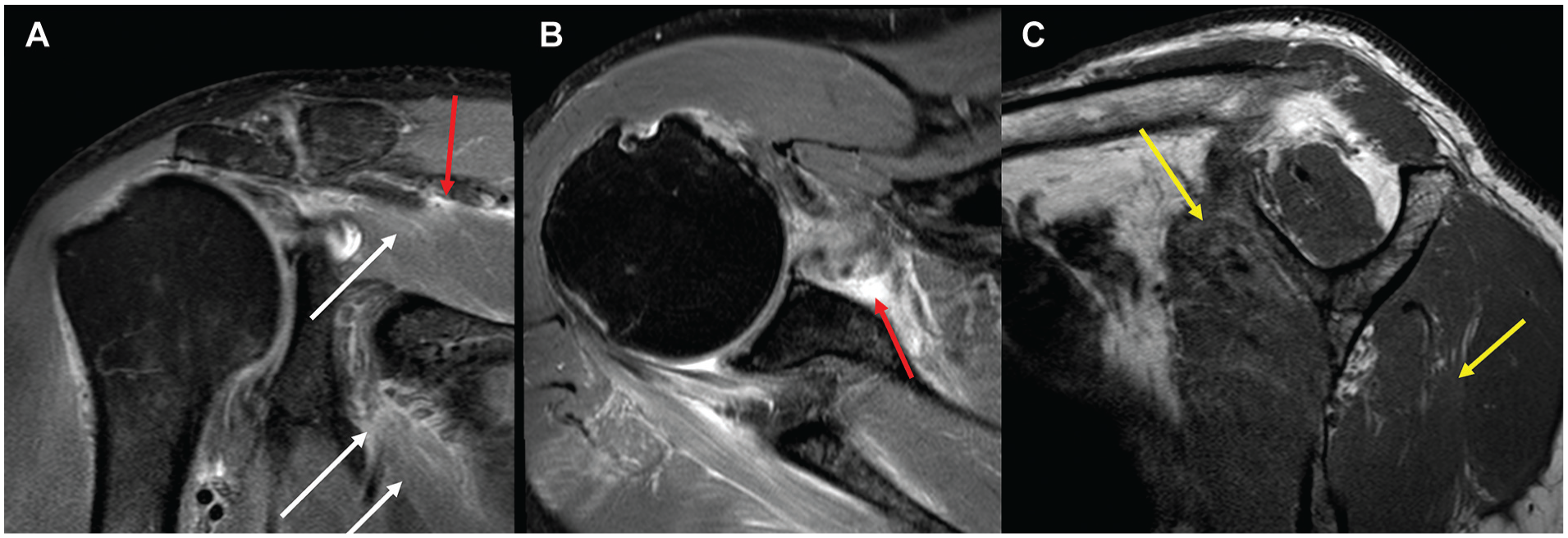
MRI was performed 1 day after a motor vehicle accident in a 60-year-old male without preexisting symptomatology, showing the immediate onset of a pseudoparalytic shoulder. T2-weighted fat-saturated MRI in the (A) coronal and (B) axial views demonstrates muscular (white arrow) and perimuscular (red arrow) edema in the supraspinatus and infraspinatus. (C) The sagittal view of the T1-weighted MRI does not reveal fatty infiltration. However, the “ground glass” appearance in the upper subscapularis and lower infraspinatus muscles, with a blurred aspect and a slightly hyperintense signal (yellow arrows), suggests pseudo-fatty infiltration. MRI, magnetic resonance imaging.

MRI at 56 days after a fall on stairs in a 63-year-old female. (A) Coronal view of T2-weighted fat-saturated MRI showing edema of retraction in the infraspinatus muscle (white arrow). (B) The sagittal view of the T1-weighted MRI shows fatty infiltration (yellow arrow). MRI, magnetic resonance imaging.
The 2 groups were compared concerning demographic, clinical, and radiological characteristics. The groups presented similar characteristics, aside from the age of presentation. The acute group included significantly younger patients (Table 1). Analysis also revealed that the time between symptom onset and MRI/MRA was shorter in the acute group (Table 1). No other radiological parameters studied—such as edema location, lesion type, tendon retraction, and other radiological signs—were able to distinguish the groups.
Patient Characteristics a

AFF, active forward flexion; SANE, Single Assessment Numeric Evaluation; SSP, supraspinatus.
The interobserver agreement for fatty infiltration evaluation was moderate to almost perfect for the supraspinatus and infraspinatus, and almost perfect for the subscapularis and the teres minor (Table 2).
Interobserver Agreement for Fatty Infiltration Evaluation a

The Gwet AC can be interpreted as follows: 0-0.2 indicates poor agreement; 0.3-0.4 indicates fair agreement; 0.5-0.6 indicates moderate agreement; 0.7-0.8 indicates strong agreement; and >0.8 indicates almost perfect agreement. ISP, Infraspinatus; SSC, Subscapularis; SSP, Supraspinatus; TM, Teres minor.
Discussion
Although muscle edema of retraction in sheep has already been described, no other study has, to our knowledge, precisely addressed this phenomenon in humans. Pogorzelski et al 20 proposed standardizing the association of terms “acute” and “traumatic” to differentiate these from “acute-on-chronic” lesions. 22 Our study provides new insights by describing the characteristics of rotator cuff muscle edema in humans, emphasizing the difference between purely acute and acute-on-chronic lesions. The key discoveries included (1) a clear distinction between acute edema and acute-on-chronic edema; (2) significantly younger age at presentation for the former; and (3) significantly earlier MRI scans in the acute group, confirming our hypothesis. All other parameters studied were presented similarly between the 2 groups. Based on these findings, we recommend that physicians consider the likelihood of new trauma in their patients despite concomitant signs of degenerative rotator cuff lesions on imaging. Furthermore, one should not consider traumatic rotator cuff lesions as purely a disease of the young.
A surprising result of our study was that the mean age of edema presentation in the acute group was 60 years. Traditionally, traumatic rotator cuff tears appear in younger patients. Guevara-Alvarez et al 11 found a mean age of 53 years in a large cohort of 302 patients with traumatic rotator cuff tears. Indeed, traumatic lesions are not necessarily limited to the young. Acute-on-chronic type of lesions appeared in older patients at a mean age of 68 years in the present study. Rubin 21 describes the clinical manifestation of acute-on-chronic tears as pain and weakness of long duration exacerbated by a recent injury and a classic “pop” sensation. He suggests that the surgeon may consider operating sooner on patients whose torn cuffs contain an acute component, as these may be easier to mobilize. Although age may be used as a guiding factor in discriminating between the 2 types of lesions, older age should consequently not be used to exclude a lesion of traumatic origin.
The time between symptom onset and MRI is shorter among patients with acute lesions, who received MRIs, on average, 23 days after symptom onset. Patients with acute-on-chronic lesions received MRIs, on average, 42 days after symptom onset. This difference existed regardless of patient characteristics, lesion grade, and symptoms. Previous studies on sheep have shown the early appearance of muscle edema after rotator cuff trauma, reaching a plateau after 3 to 4 weeks. 12 Corresponding histological analysis has shown early muscle fiber degeneration after an acute lesion. It has therefore been suggested that surgery should ideally be performed within the first 21 days after the injury. 22 Pogorzelski et al 20 propose imaging within the first 2 weeks after the initial trauma to detect a truly acute rotator cuff lesion. Surgery is recommended within 8 weeks, after which a decrease of most growth factors and cytokines has been demonstrated.
The previous literature did not confirm that the presence of a remaining tendon stump at the greater tuberosity is a sign of an acute traumatic tear.8,16 Alben et al 1 have, on the contrary, reported a case of distal infraspinatus tendon stump on the greater tuberosity in an isolated, atraumatic tear of the rotator cuff. The present study found a stump in 47% of acute tears and 35% of acute-on-chronic tears, a higher proportion than reported by Furrer et al. 8 The cobra sign, introduced by Furrer et al as a “buckling back” of the torn rotator cuff tendon in the context of trauma, was confirmed in our study to be specific to traumatic rotator cuff lesions, although with low sensitivity.
The clinical relevance of this study concerns disease causality and its implications for prognosis, timing of potential surgery, and even accident insurance coverage. The presence of a degenerative rotator cuff lesion on imaging should not be the basis used to exclude trauma. Loew et al 15 conducted a study to discriminate acute from chronic rotator cuff lesions. Our study, however, explores the possibility of differentiating acute lesions from an acute aggravation of a preexisting, degenerative lesion. We observed that the main difference between the 2 groups was in the age of presentation and the time between the onset of symptoms and the MRI. No other characteristics studied were able to discriminate one group from the other.
Limitations
The study presents some limitations. Electroneuromyography was not performed to exclude neurogenic (or denervation) edema. However, the prevalence of suprascapular nerve injury in the case of a massive rotator cuff tear is rare. 6 Denervation edema has also been shown to have a different presentation from edema of traumatic origin. 23 A second limitation of our study was that Dixon sequences, necessary for finer analysis of edema, were not always available. Without these sequences, edema may be confused with pseudo-fatty infiltration, as both appear as hyperintense signals on T1 and T2 sequences. 23 The third limitation is that muscular edema of retraction is likely to be underreported. Most patients with a history of trauma do not have edema on MRI. It must, however, be noted that MRIs are most frequently done months after the trauma date, whereas the peak appearance after trauma is between 3 and 4 weeks. 12 Physicians must thus be aware that an absence of edema on MRI is not conclusive of an absence of trauma.
Conclusion
Muscle edema of retraction helps to distinguish new rotator cuff injury from acute extensions of preexisting lesions via 2 discriminating factors. The first is that new rotator cuff lesions present in younger populations with edema in the absence or near absence of fatty infiltration. Muscle edema present in the context of more severe fatty infiltration is more readily found in older populations and is likely due to an acute extension of a preexisting lesion. Second, patients with acute lesions of the rotator cuff or traumatic rotator cuff lesions should consult earlier.
Footnotes
Acknowledgements
The authors thank the LaTour (Leading Advancements in Therapeutic and Outcome-based Research) group for their support.
Final revision submitted February 20, 2025; accepted April 21, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the Foundation for Research and Teaching in Orthopaedics, Sports Medicine, Trauma, and Imaging in the Musculoskeletal System (FORE) (grant ID, FORE 2024-8). A.L. is a paid consultant for Arthrex, Stryker, Medacta, and Enovis; has received royalties from Stryker and Medacta; is the co-founder of FORE, Med4Cast, The HIVE, and BeeMed; owns stock options in Medacta and Follow Health; and is on the board of the French Arthroscopic Society. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was obtained for this study (CCER 2015-15 trial registration number NCT02725346; CCER 2016-00818 trial registration number NCT02943005; 2019-02076 trial registration number NCT04321005).