
Abstract
Introduction
Hospital readmissions after elective shoulder arthroplasty represent a costly burden to the health-care system due to the rising demand for this procedure. Nevertheless, the reasons for readmissions remain inconclusive. Therefore, the main purposes of the current investigation were to determine (1) the readmission rates within 90 days after shoulder arthroplasty, (2) the reasons behind those readmissions, and (3) the characteristics of readmitted patients.
Methods
A retrospective review was performed on 184 patients who underwent total shoulder arthroplasty (TSA) or reverse shoulder arthroplasty (RSA) performed by a single surgeon at a single institution between 2010 and 2016. The readmissions that occurred within 90 days after surgery and their reasons were noted. Patient characteristics were compared between readmitted and non-readmitted patients.
Results
Overall, 7.1% of patients were readmitted within 90 days after shoulder arthroplasty. However, patients with a previous surgery on the same shoulder of the TSA or RSA had a higher rate (13.5%) than patients without a previous surgery (5.4%). Readmission rates for TSA and RSA were virtually identical. Most readmissions were due to surgical (69.2%) rather than medical complications (30.8%). The most common reasons for readmission were surgical-site infection and deep vein thrombosis. There were no statistically significant differences between the baseline patient characteristics of readmitted and non-readmitted patients. However, the proportion of males (69.2%) was more than twice the one of females (30.8%) among readmitted patients.
Conclusion
The readmission rate within 90 days after surgery was relatively low among patients who underwent either a TSA or RSA at our institution. Surgically related causes were largely responsible for readmissions.
Keywords
Introduction
In the United States, there has been an exponential growth in the number of shoulder arthroplasties, from 28,000 performed between 2000 and 2008 to approximately 100,000 in 2015.1,2 In addition to morbidity and mortality rates, the readmission rate within 90 days after surgery is currently considered an important indicator of quality of care.1–6 Given the rise in the number of shoulder arthroplasties being performed, readmissions have become increasingly important and deserve a closer evaluation as a relevant quality and cost parameter.
Postsurgical, unplanned hospital readmissions represent a burden on both, the patient and the health-care system. In 2004, 30-day readmissions of Medicare patients represented a total cost of $17.4 billion in unnecessary expenses. 6 Decreasing the number of readmissions has been a major issue highlighted for value-based care as illustrated in bundle payments and Comprehensive Care for Joint Replacement payment models. Unplanned readmissions might not only reflect on patient safety and quality but also create additional expenses for the hospital while decreasing patient satisfaction.1,3,7
As the population ages and the use of shoulder arthroplasty expands, it could be reasonable to expect that medical and surgical complications leading to readmissions would rise. Westermann et al. found that medical complications accounted for more than 50% of readmissions. 2 Various studies have analyzed the data surrounding 90-day unplanned readmissions following shoulder surgery and their correlation to various risk factors.1–3,5,8 Matsen et al. 1 reported that patients with increased age and medical comorbidities were at higher risk of readmission. Further studies have indicated that procedure type also plays a role in readmission rates.9–11 Postoperative readmission rates after shoulder surgery have not been well studied, 12 and the reasons for readmissions remain inconclusive. As a result, the purposes of this study were to determine (1) the readmission rates within 90 days after shoulder arthroplasty, (2) the reasons for readmissions, and (3) the characteristics of those patients who were readmitted.
Materials and Methods
A retrospective review was performed on 184 patients with Medicare and/or other insurers who underwent either total shoulder arthroplasty (TSA) (n = 57) or reverse shoulder arthroplasty (RSA) (n = 127) performed by a single orthopedic surgeon at a single institution between 2010 and 2016. Current Procedural Terminology codes were used to identify cases, and all medical charts were reviewed to identify all patients who were readmitted within 90 days after TSA or RSA surgery. The readmission rates and the reasons for readmissions were recorded and analyzed on the entire cohort of patients (n = 184) and on a subgroup of patients who had a previous surgery before the TSA or RSA (n = 37/184, 20%). The reasons for readmissions were categorized into either medical complications (ie, pulmonary edema or pneumonia) or surgical complications such as surgical-site infection (SSI) or deep vein thrombosis (DVT). Patient characteristics were compared between readmitted and non-readmitted patients. Demographic characteristics evaluated, included age at procedure, gender (male/female), body mass index (BMI), American Society of Anesthesiologist (ASA) physical status classification system, smoking status, preoperative diagnosis, procedure type, length of stay (LOS), intraoperative blood loss, operating room (OR) time, and the presence or not of a previous surgery on the affected shoulder.
Statistical Analysis
Descriptive statistics were employed to determine 90-day readmission rates and the causes of readmission in the entire cohort of patients and in the 2 subgroups based on whether they had or not a previous surgery on the same side. Variables such as age, BMI, LOS, or intraoperative blood loss were compared between readmitted and non-readmitted patients making use of independent-sample t tests. Categorical variables such as gender, ASA, smoking status, preoperative diagnosis, the presence of a previous surgery on the operated shoulder, or arthroplasty type were compared using Pearson χ2 test or Fisher’s exact test using SPSS software (IBM Corporation, Armonk, New York). Statistical significance was set at P ≤ .05.
Results
Overall, the entire cohort consisted of 98 females (54.3%) and 86 males (46.7%) with a mean age of 71.7 years (range, 44–97). Nearly all of our patients were either ASA class II (48.9%) or ASA class III (50%) with a mean BMI of 29.8 kg/m2. In our series, a preoperative diagnosis of osteoarthritis was the most common indication for shoulder arthroplasty (51.1%) followed by rotator cuff arthropathy (36.4%) and fractures (11.4%).
The overall readmission rate after shoulder arthroplasty in our study was 7.1% with a trend toward a higher rate (13.5%) in the subgroup of patients who had a previous surgery on the affected shoulder when compared to those patients who did not have a previous surgery (5.4%) (P = .14) (Tables 1 and 2). When readmission rates were broken down by procedure type, we found that there was no significant difference between TSA (7.0%) and RSA (7.1%) (Table 3). Most readmissions were due to surgical complications (69.2%) rather than medical complications (30.8%) (Tables 4 and 5).
Prior Surgery on Affected Shoulder (Breakdown of Procedures) (n = 37).

Readmission Rates in the Entire Cohort and in the 2 Subgroups.

Readmission Rates by Procedure Type.

Reasons for Readmission Within 90 Days After Surgery (Entire Cohort).

Abbreviation: DVT, deep vein thrombosis.
Reasons for Readmissions Within 90 Days After Surgery in the 2 Subgroups.
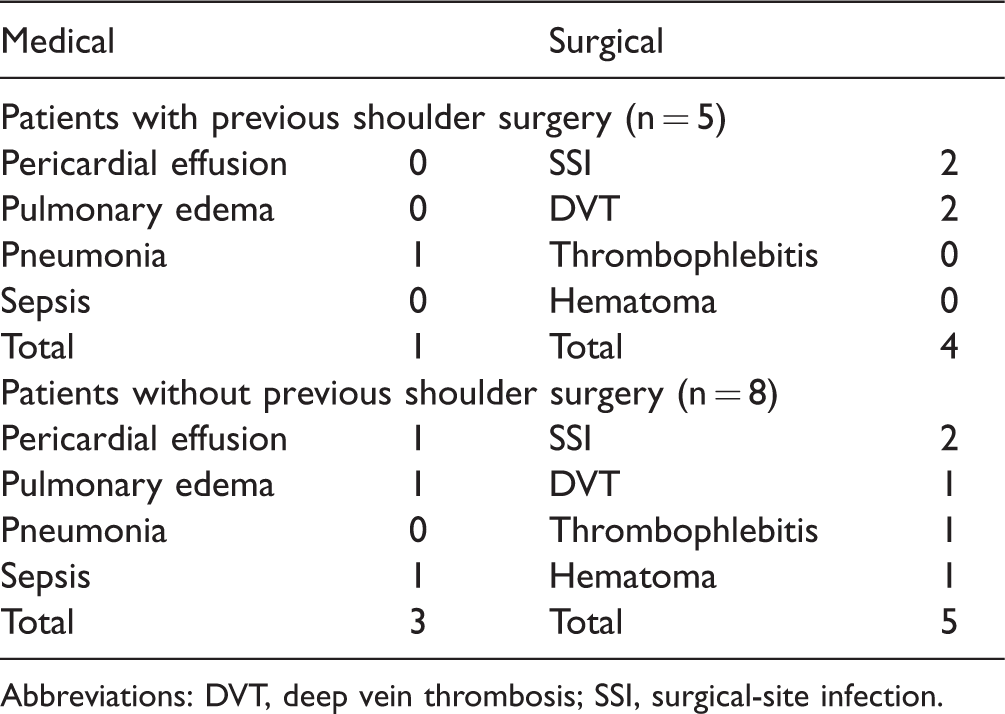
Abbreviations: DVT, deep vein thrombosis; SSI, surgical-site infection.
SSI was the most common reason for readmission (30.8%) followed by DVT (23.1%). The medical causes of readmissions were evenly divided between pulmonary edema, pericardial effusion, pneumonia, and sepsis (each, n = 1) (Table 4).
Baseline Demographics and Patient Characteristics.

Abbreviations: ASA, American Society of Anesthesiologist; BMI, body mass index; OR, operating room.
aMean ± standard deviation.
bNumber of cases (percentages) within non-readmitted and readmitted groups.
Discussion
The readmission rate after shoulder arthroplasty is currently considered an important indicator of quality of care.1–6 However, this parameter has not been extensively studied. 12 A closer evaluation of readmissions as a relevant quality parameter is warranted. In our study, the readmission rates within 90 days after shoulder arthroplasty, the reasons behind those readmissions, and the specific characteristics of readmitted patients were studied.
The overall readmission rate within 90 days after primary shoulder arthroplasty was 7%, regardless of risk factors. We reviewed age, gender, and BMI. None of these specific demographic factors contributed to readmissions. In general, our low rate was consistent with the literature. Mahoney et al. and Schairer et al. showed that 90-day readmission rates were as high as 5.9% and 7.3%, respectively.6,11 However, in our series, the proportion of males (69.2%) was more than twice the one of females (30.8%) among readmitted patients. Westermann et al. 2 did not find gender to be significantly associated with readmissions (P = .8) even though in that investigation males represented only 42% of readmitted patients. Of note, we found a slightly higher readmission rate (13.5%) among patients who had a surgery on the same shoulder prior to the TSA or RSA.
Interestingly, our data also showed that readmission rates did not differ by procedure type (TSA vs RSA), which is not consistent with previous reports. Typically, the literature has shown that there are higher complication rates and readmissions for RSA. Our results suggest that perhaps with advances in indications and techniques, we may be decreasing the rate of postoperative complications. Schairer et al. 6 found a higher 90-day readmission rate for RSA (11.2%) when compared to TSA (6.0%). Mahoney et al. 11 showed that the highest 90-day readmission rates occurred after hemiarthroplasty (8.8%) followed by RSA (6.6%) and TSA (4.5%).
Concerning the reasons for readmissions, we found that most were due to surgical rather than medical complications. Westermann et al. 2 found that medical complications accounted for more than 50% of readmissions after TSA. Schairer et al. 6 showed that medical reasons contributed to 82% of all readmissions while surgical complications only accounted for 18% of them. A breakdown of their surgical readmissions showed that SSIs was the most common cause (4.8%) followed by dislocation (4.6%). Although other studies have highlighted medical complications contributing to readmissions, our results suggest that a focus on preventable surgical complications may also benefit the hospital and the patient.
Our investigation should be viewed in light of certain limitations. Since our data only included patients readmitted to our institution, we were unable to identify patients who after discharge may have been readmitted to other hospitals. Notwithstanding, due to the short period of follow-up (90 days), we think that the probability of those occurrences is very low. The current investigation was performed in a single center; and consequently, geographic and/or demographic factors could have skewed our results. However, our institution is located in South Florida (a melting pot in the states) and takes care of a population with diverse racial, ethnic, and socioeconomic background. Our sample size is relatively small; nonetheless, all data collected were obtained from direct chart review in stark contrast to studies with larger sample sizes that rely exclusively on data provided by administrative databases. We had excellent granularity in each one of the cases studied. Finally, limited information was available on details of the previous surgery in our medical records.
In conclusion, our data suggest that the readmission rate within 90 days after primary TSA or RSA is relatively low. No demographic risk factor appears to contribute to readmissions in this population. Surgically related causes such as SSI and DVT are largely responsible for readmissions. Perhaps, focus on these preventable postoperative complications may decrease readmissions even further. Further investigations on readmission rates should be performed before hospitals can be graded on readmission rates as a good indicator of quality of care in shoulder arthroplasty.
Footnotes
Ethical Approval
This study was approved by Cleveland Clinic Institutional Review Board (FLA 17-006).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Vani Sabesan is a paid consultant for Arthrex, Inc.; Gregory Gilot is a paid consultant for DJO and receives royalties from Cayenne and Exactech. All the other authors disclose no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Vani Sabesan receives research support from Exactech, Inc.