
Abstract
Background:
Coexisting medial impingement syndrome of the ankle (MIA) is often observed when planning surgical treatment for medial osteochondral lesion of the talus (OLT). To date, there is no clear consensus on the surgical indications for MIA in relation to medial OLT or on whether overtreatment or undertreatment is preferable.
Purpose:
To investigate when and how MIAs should be treated in patients with concomitant medial OLT.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
A total of 47 patients diagnosed with medial OLT and concomitant MIA were prospectively evaluated between January 2020 and June 2023. Patients were enrolled when they tested positive for the MIA provocation test (pain at the medial malleolus was exacerbated with ankle varus and dorsiflexion maneuvers) and randomly assigned to either the solitary medial OLT treatment group (group 1; n = 23 patients) or the simultaneous medial OLT and MIA treatment group (group 2; n = 24 patients). In group 2, osteophytes associated with MIA were addressed using a combined arthroscopic and miniopen approach along with the microfracture technique for medial OLT, whereas in group 1, only a solitary arthroscopic microfracture was performed. The minimum follow-up duration for inclusion in this study was 12 months.
Results:
The clinical parameters at the final follow-up significantly improved postoperatively in both groups, and the values at the final follow-up did not significantly differ between the 2 groups. However, the rate of pain elicitation during the MIA provocation test at the final follow-up was significantly greater in group 1 than in group 2 (72.2% vs 10.5%; P < .001). None of the patients had superficial/deep infections, operation-related neurovascular injuries, or revision surgery during the follow-up period.
Conclusion:
Although the results of our study alone cannot conclusively determine that surgical treatment is necessarily required for MIA concomitant with medial OLT, the significant postoperative reduction in pain elicited during the MIA provocation test was observed in patients who underwent simultaneous MIA resection. Considering the relatively less technically demanding nature of the surgical technique introduced in this study, we recommend proactive resection in patients with both MIA and medial OLT where pain is elicited during the MIA provocation test preoperatively.
Keywords
Medial impingement syndrome of the ankle (MIA) is defined as the “kissing lesion” between osteophytes on the dorsomedial side of the talar neck and front of the medial ankle mortise, making a huge anterior bony spur at the medial malleolus with a disease progression (Figure 1).7,10,11,13 MIA represents a less prevalent source of enduring ankle discomfort, often occurring alongside pure anterior impingement. 18 Similar to other impingement syndromes, the diagnosis of MIA primarily relies on clinical assessment, characterized by pain during ankle dorsiflexion and inversion, as these spurs can be correlated with localized hemorrhage, reactive synovitis, and eventual capsular or ligamentous scarring, along with localized chondral damage. 6 Physicians can detect MIA through standing ankle radiographs or varus stressed radiographs, oblique foot radiography,11,14 or magnetic resonance arthrography. 16

Radiographic appearance of the typical medial impingement syndrome of the ankle.
To date, there is no known information regarding the incidence and the proportion of patients diagnosed with MIA who require surgical intervention. In our clinical experience, we often encounter cases in which patients with medial osteochondral lesion of the talus (OLT) also exhibit MIA. 3 Although surgical treatment primarily focuses on addressing the medial OLT, it remains uncertain whether concomitant surgical intervention for MIA is necessary. Despite the observation of a considerable number of cases in which both conditions coexist, to the best of our knowledge, there is no consensus on whether and how to surgically address MIA in these patients. Therefore, this study aimed to investigate when and how to treat MIA in patients with concomitant medial OLT. To this end, we introduced our surgical treatment process and sought to test the hypothesis that there would be advantages in addressing MIA through concomitant surgery with medial OLT treatment compared with a selected control group.
Methods
Ethical Considerations
This study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the institutional ethics review committee. Written informed consent was obtained from all the enrolled patients.
Study Design and Patients
This prospective comparative study involved the consecutive enrollment of skeletally mature patients aged ≥18 years who had persistent medial side ankle pain unresponsive to nonoperative treatment (activity restriction, oral painkillers, or physical therapy) between January 2020 and June 2023. During the initial patient screening, only those suspected of having both medial OLT and MIA were primarily selected based on standing ankle radiographs and oblique foot radiographs. Medial OLT was defined as the presence of a radiolucent lesion or subchondral cyst in the medial talar gutter, while MIA was defined as the presence of a bony spur on the medial malleolus impinging on the medial aspect of the talus. In this process, to rule out the effect of advanced varus ankle arthritis on MIA, patients whose space between the medial malleolus and medial talar gutter was narrowed/obliterated or whose talar tilt was >2° on standing ankle anteroposterior radiographs were not selected. 4
Subsequently, patients were ultimately selected if magnetic resonance imaging (MRI) confirmed the presence of medial OLT and if medial ankle pain was further aggravated during the MIA provocation test. The MIA provocation test assessed whether pain at the medial malleolus was exacerbated by ankle varus and dorsiflexion maneuvers to elicit impingement.3,7,20 In addition, we assessed direct tenderness or localized pain on the bony spur of the medial malleolus at the impingement site.
After the completion of the initial inclusion screening, the following exclusion criteria were applied to finalize patient selection: (1) patients with systemic inflammatory diseases, such as rheumatoid arthritis or gout; (2) a history of bony or soft tissue trauma that could potentially influence ankle or foot alignment; or (3) a history of surgery at the same anatomic site. The patients were then randomly assigned to either the solitary medial OLT treatment group (group 1) or the simultaneous medial OLT and MIA treatment group (group 2) using the Research Randomizer tool (http://www.randomizer.org). In the final study cohort, only patients who completed a postoperative follow-up of ≥12 months were included among those initially enrolled.
Sample Size Calculation
The appropriate sample size for this study was determined using a formula for calculating the sample size in a comparison between the 2 groups when the endpoint involved quantitative data. The power of the study was set at 80%, and the significance level was set at .05. The primary endpoint selected for sample size determination was the postoperative Foot and Ankle Ability Measure-Activities of Daily Living (FAAM-ADL) score in group 2 compared with that in group 1. To calculate the sample size, we referenced a previous study that focused on the factors affecting MIA symptoms. 3 In light of this, we opted for an effect size of 15 points and a standard deviation of 13.7. Based on these parameters, the calculated sample size was 16. To account for potential patient attrition during the follow-up period, a dropout rate of 10% was allowed. Consequently, a minimum of 18 patients were required in each group.
Surgical Treatment of Concurrent MIA and Medial OLT
A single orthopaedic surgeon (J.Y.C.) performed all surgical procedures under general or spinal anesthesia. A pneumatic tourniquet was applied to the proximal thigh after the patient was placed in a supine position. Standard anteromedial and anterolateral portals were made, and an arthroscopic examination of the ankle joint was performed to confirm the presence of osteophytes at the anterior aspect of the medial ankle mortise and medial malleolus and dorsomedial aspect of the talar neck. In addition, the examination assessed whether these osteophytes caused impingement during ankle varus and dorsiflexion maneuvers. The presence of a medial OLT was also evaluated. Subsequently, arthroscopic synovectomy was performed in all cases, followed by burring of each spur on the dorsomedial aspect of the talar neck and anteromedial ankle mortise, along with a microfracture technique for medial OLT. Our surgical principle for arthroscopic microfracture was similar to that of the conventional technique, involving the removal of all unstable osteochondral fragments and the creation of holes at regular intervals (3-4 mm) on the subchondral surface using an awl. Afterward, the medial portal incision was longitudinally extended 2 cm distally. The spur at the most distal medial malleolus around the attachment site of the deltoid ligament was removed using an osteotome under fluoroscopic guidance, with careful attention paid to minimize the deltoid ligament injury. If arthroscopic removal of the osteophytes at the anteromedial ankle mortise (distal tibia) was deemed insufficient, additional resection was performed. In cases of concomitant lateral ligament repair, the procedure was performed after completing ankle arthroscopy and miniopen medial osteophyte resection. Lateral ligament repair was performed in cases of recurrent sprains, subjective instability, after os subfibulare excision, or when an anterior talofibular ligament injury was confirmed on preoperative MRI. The surgical procedure is schematically illustrated in Figure 2. In the solitary medial OLT treatment group, bony spurs on the anterior aspect of the medial ankle mortise, the medial malleolus, and the dorsomedial talar neck were not resected.
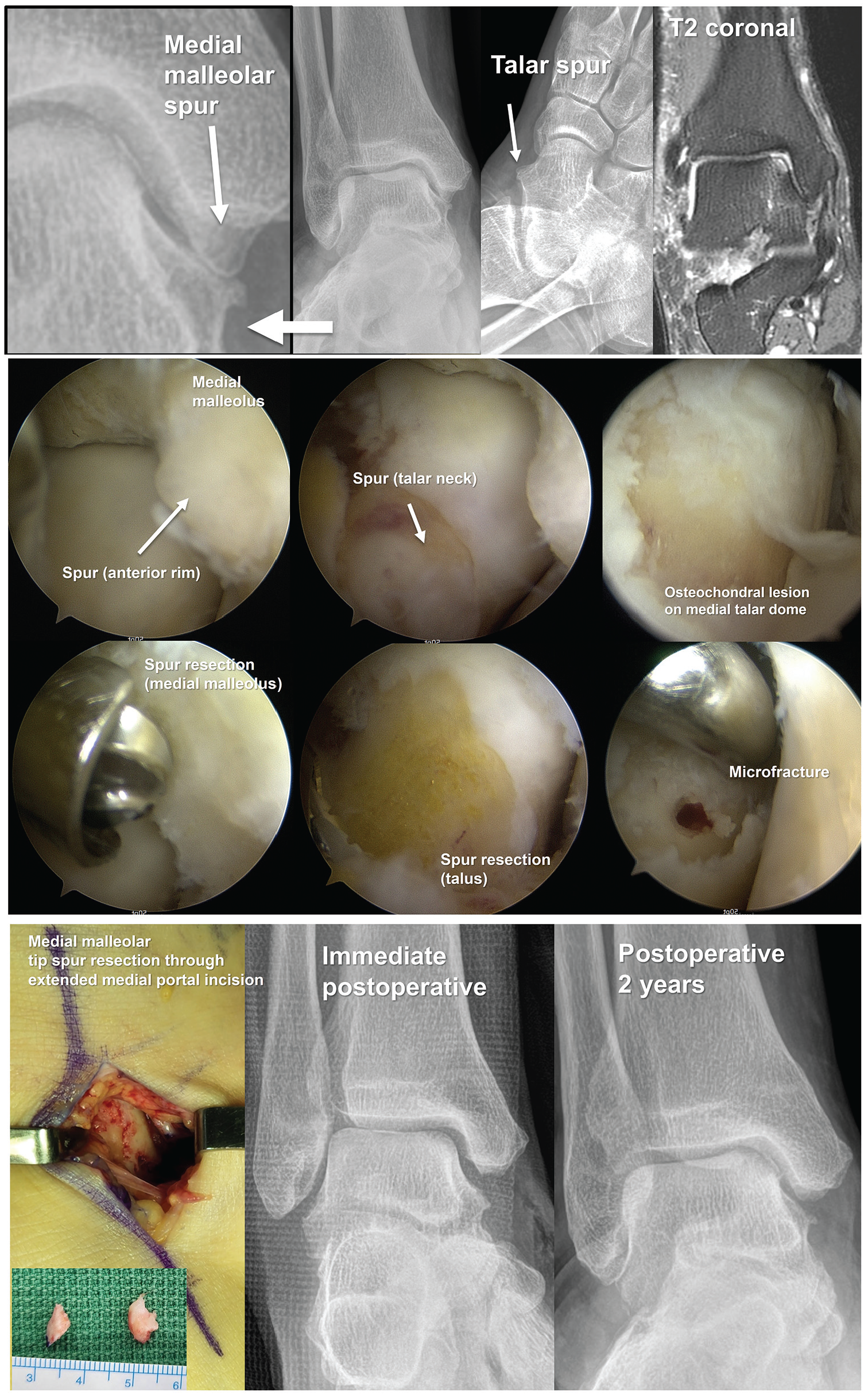
Our surgical procedure for the simultaneous treatment of medial osteochondral lesion of the talus and medial impingement syndrome of the ankle.
Postoperatively, in cases performed without lateral ligament repair, a short leg splint was applied and maintained for 4 postoperative weeks. Weightbearing was restricted during the initial postoperative week, with partial weightbearing permitted using crutches or canes for the subsequent 3 weeks. Full weightbearing without a splint was permitted starting at postoperative week 5, with sports activities allowed at 3 months postoperatively. For patients who underwent lateral ligament repair, postoperative management included nonweightbearing and immobilization in a below-knee cast for 6 weeks. Gradual weightbearing, along with peroneal muscle strengthening exercises and proprioceptive training, was initiated over the subsequent 6 weeks. Return to sports activities was permitted 12 weeks after surgery.
First, arthroscopic synovectomy was performed, followed by burring of each spur and a microfracture technique for medial OLT. Subsequently, the medial portal incision was longitudinally extended 2 cm distally. The spur at the medial malleolar tip around the attachment site of the deltoid ligament was removed using an osteotome under fluoroscopic guidance, with careful attention paid to minimizing deltoid ligament injury.
Assessments
Descriptive data—including patient age at the time of surgery, sex, affected side, body mass index (BMI), smoking status, and duration of symptom manifestation—were collected. Through physical examination performed by the operating surgeon during each outpatient clinic visit, we measured the degree of passive ankle range of motion (ROM) (dorsiflexion, plantar flexion, inversion, and eversion) and conducted an MIA provocation test to confirm whether pain was elicited. In addition, surgical procedure-related information—such as operative time, type of anesthesia, and concomitant procedures—was documented. Moreover, the size of medial OLT observed directly via arthroscopy was investigated; this was defined as the product of the longest horizontal and vertical dimensions measured during surgery.
Functional outcomes were assessed preoperatively and at the final follow-up (approximately 1 year postoperatively) using the visual analog scale (VAS) (0, no pain to 10, maximal pain) and FAAM subscale scores for ADL and Sports.12,15,17 The FAAM scores ranged from 0 to 84 and 0 to 32 for the ADL and Sports subscales, respectively. These evaluations were based on self-administered questionnaires completed by the patients. The postoperative complications that occurred during the follow-up period were also documented.
Statistical Analyses
The means and standard deviations of all dependent parameters were calculated using SPSS Statistics Version 21 for Windows (IBM Corp). Data normality was assessed using the Shapiro-Wilk test. Numeric parameters between the 2 groups were compared using the Mann-Whitney U test, whereas proportional parameters were compared using the Fisher exact test. The Wilcoxon signed-rank test was used to compare the pre- and postoperative clinicoradiographic parameters. Statistical significance was defined as P < .05 for all analyses.
Results
Patient Characteristics
Initially, 80 patients were enrolled, of whom 20 did not meet the inclusion criteria (17 had no pain elicited during the MIA provocation test, and 3 were found to have ankle arthritis on standing ankle radiographs). Moreover, 5 patients were excluded because of the exclusion criteria (4 patients with systemic inflammatory diseases and 1 patient with a history of trauma at the affected ankle), and 1 patient declined to participate. Thus, a total of 54 patients were included in the study, with 27 patients allocated to each group (groups 1 and 2). After excluding dropouts during the follow-up, the final analysis included 23 patients in group 1 and 24 patients in group 2. The patient selection algorithm is illustrated in Figure 3.

Patient selection algorithm.
Patients’ characteristics are presented in Table 1. The mean age for all patients at the time of surgery was in the early 50s, with a higher proportion of men. The mean BMI was 25.3 kg/m2. The mean duration of symptom manifestation was 4.8 months. With the numbers available, no significant differences were detected in any of the demographic and clinical parameters between the 2 groups (P > .05).
Patient Characteristics a

Values are presented as mean ± SD, mean ± SD (range), or n (%). P values indicate the statistical comparison between the 2 groups. ADL, activities of daily living; BMI, body mass index; FAAM, Foot and Ankle Ability Measure; Preop, preoperative; VAS, visual analog scale.
Initially, 70 patients were enrolled, with 27 patients allocated to each group. After excluding dropouts during the follow-up, the final analysis included 23 patients in group 1 and 24 patients in group 2.
Comparison Between the 2 Groups Based on Concomitant Treatment of MIA
The results of the comparison between the 2 groups based on the additional MIA treatment are summarized in Table 2. The operative time was significantly longer in group 2 than in group 1 (P = .023). Concomitant procedures—including the modified Broström procedure, os subfibulare excision, and anterior osteophyte resection—were performed at similar rates in both groups.
Comparison of Surgery-Related Parameters and Outcomes Between the 2 Groups Based on the Additional MIA Treatment a
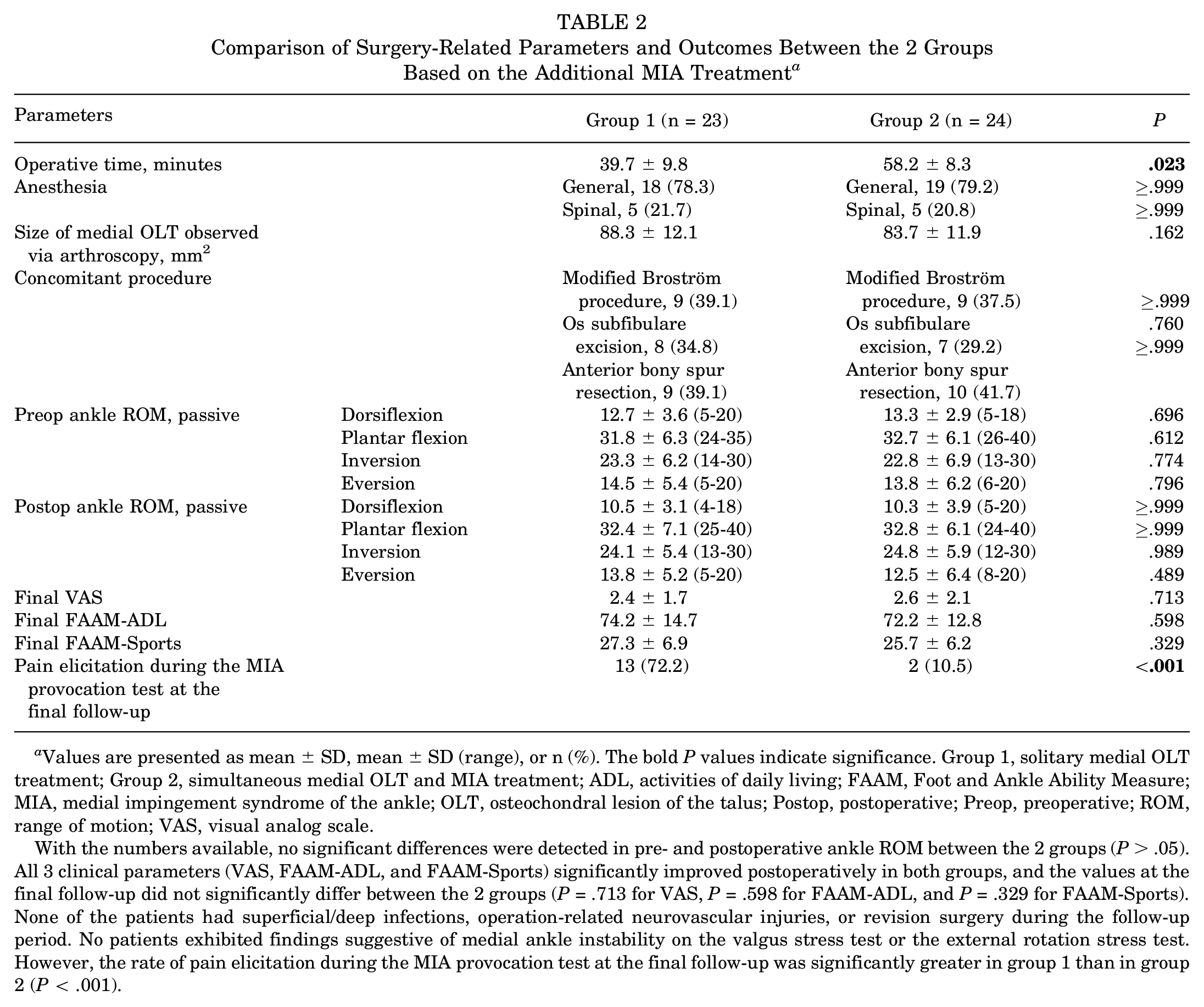
Values are presented as mean ± SD, mean ± SD (range), or n (%). The bold P values indicate significance. Group 1, solitary medial OLT treatment; Group 2, simultaneous medial OLT and MIA treatment; ADL, activities of daily living; FAAM, Foot and Ankle Ability Measure; MIA, medial impingement syndrome of the ankle; OLT, osteochondral lesion of the talus; Postop, postoperative; Preop, preoperative; ROM, range of motion; VAS, visual analog scale.
With the numbers available, no significant differences were detected in pre- and postoperative ankle ROM between the 2 groups (P > .05). All 3 clinical parameters (VAS, FAAM-ADL, and FAAM-Sports) significantly improved postoperatively in both groups, and the values at the final follow-up did not significantly differ between the 2 groups (P = .713 for VAS, P = .598 for FAAM-ADL, and P = .329 for FAAM-Sports). None of the patients had superficial/deep infections, operation-related neurovascular injuries, or revision surgery during the follow-up period. No patients exhibited findings suggestive of medial ankle instability on the valgus stress test or the external rotation stress test. However, the rate of pain elicitation during the MIA provocation test at the final follow-up was significantly greater in group 1 than in group 2 (P < .001).
Discussion
Our study revealed no significant differences in clinical outcomes between solitary medial OLT treatment and simultaneous medial OLT and MIA treatment (removal of various osteophytes associated with MIA) in patients with symptomatic MIA accompanied by medial OLT. However, pain and discomfort might be provoked during specific ankle motions and maneuvers even beyond 1 year postoperatively, although there was no significant difference in clinical outcomes when concomitant MIA was left untreated.
Regarding the relationship between MIA and medial OLT, Choi et al 3 suggested that a high incidence of medial OLT (81.6%) was observed in nonathletic patients with symptomatic MIA. In their study, the definition of symptoms was set similarly to ours, focusing on whether pain was elicited during the MIA provocation test. However, it is essential to acknowledge that the MIA provocation test used in this study has significant limitations. Our findings indicate that the MIA provocation test may have too high sensitivity and too low specificity for determining the necessity of surgery and for assessing postoperative recovery. It was encouraging that only 10.5% of patients who underwent simultaneous surgery for medial OLT and MIA experienced pain during the MIA provocation test at the final follow-up. However, the fact that 27.8% of patients who did not undergo MIA resection also did not experience pain during the MIA provocation test at the final follow-up raises concerns about the reliability of this test. This result also suggests that the medial OLT may contribute to the mechanism by which pain is induced during the MIA provocation test. Therefore, accurate determination of the surgical indication for MIA requires new approaches, such as administering lidocaine at the impingement site to see if pain is alleviated, or utilizing another imaging modality, such as single photon emission computed tomography (CT) or Tc-methylene diphosphonate bone scans.
In our clinical experience, we observed several outpatients with MIA without concurrent pain at the affected site. Moreover, the presentation of MIA symptoms demonstrated considerable variability among patients, even when the osteophyte sizes were substantial. MIA was first reported by Mosier-La Clair et al 13 as impingement of the anterior tibiotalar fascicle of the deltoid ligament on the talus, and only a few relevant studies have been reported to date.2,3,7,9-11,13,14,16,19,20 Generally, MIA may be caused by recurrent ankle inversional and rotational injuries, leading to recurrent abnormal impaction and damage to the deltoid ligament.7,10 Zhang et al 20 and Koh et al 9 have reported a high incidence of MIA associated with chronic lateral ankle instability by suggesting approximately 20% of the study cohort underwent concurrent surgery for lateral ankle instability. More recently, Choi et al 3 also mentioned that 62.4% of nonathletes with MIA had a history of recurrent sprains. Similarly, in our study, the modified Broström procedure was performed in 38.3% of patients (18 out of 47 patients). In addition, we also consider the possibility that persistent ankle varus instability may have played a role in inducing pain elicited during the MIA provocation test at the final follow-up in 10.5% of a group with a simultaneous medial OLT and MIA surgery.
Regarding surgical procedures for MIA, a resection of both the talar and medial malleolar osteophytes using either open arthrotomy 19 or arthroscopy 14 has been established as the prevailing treatment approach. Murawski and Kennedy 14 reported that arthroscopic resection of the MIA yielded excellent functional outcomes and minimal complications. The primary surgical objective should be the adequate removal of osteophytes, as the pain arises from the impingement of these osteophytes. Based on our experience, osteophytes at the talar neck and anteromedial ankle mortise could be easily removed arthroscopically; however, those at the distal part of medial malleolus were more challenging to handle because the presence of the deltoid ligament may hinder precise exposure of the osteophyte, potentially resulting in inadequate resection through arthroscopy or excessive deltoid ligament injury. Hence, a crucial technical recommendation utilized in our surgical procedure involves employing a miniopen approach for the excision of osteophytes at the area at distal medial malleolar area, ensuring a clear view to reduce surgical time and minimize unnecessary damage to the deltoid ligament.
Limitations
This study has several limitations, including a relatively short mean follow-up duration of approximately 1 year postoperatively and a small sample size in each group. Furthermore, we were unable to quantify the size of MIA. While quantifying MIA could provide evidence for accurate surgical indications, there are no published methods for quantifying the size of MIA to date. However, weightbearing CT1,5,8 is expected to significantly aid in the quantification of MIA, and it is necessary to address the relationship between quantitative measurements of MIA and surgical indications in future studies.
Conclusion
The results of our study alone cannot conclusively determine that surgical treatment is required for MIA concomitant with medial OLT. However, the significant postoperative reduction in pain elicited during the MIA provocation test in patients who underwent simultaneous MIA resection and the relatively less technically demanding nature of the surgical technique introduced in this study support recommending proactive resection in patients with both MIA and medial OLT where pain is elicited during the MIA provocation test preoperatively.
Footnotes
Final revision submitted April 7, 2025; accepted April 23, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Inje University Ilsan Paik Hospital (2023-06-015).