
Abstract
Background:
Osteochondral lesions of the talus (OLTs) most commonly occur in the posteromedial talar dome; however, there are no consensus guidelines on the appropriate approach to performing microfracture; that is, whether adequate visualization can be achieved solely through anterior ankle arthroscopy as well as the circumstances under which posterior ankle arthroscopy is required.
Purpose:
To ascertain whether (1) arthroscopic microfracture of posteromedial OLT can be accomplished solely through anterior ankle arthroscopy and (2) if there are specific conditions that may require posterior ankle arthroscopy.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
We retrospectively reviewed videos of patients who underwent primary arthroscopic microfractures for OLT on the posteromedial talar dome between January 2010 and June 2021. The enrolled patients were divided into 2 groups according to the direction of arthroscopy (anterior or posterior). Then, we focused on whether visualization of the posteromedial OLT was adequate through the anteromedial or anterolateral portal in the anterior ankle arthroscopy group (posteromedial or posterolateral portal in the posterior ankle arthroscopy group). Similarly, we assessed whether a sufficient microfracture technique was feasible during surgery.
Results:
A total of 79 patients were included in this study, among which 62 and 17 were assigned to the anterior and posterior ankle arthroscopy groups, respectively. Posteromedial OLTs were fully observed through the anteromedial portal in 79.0% of cases and better observed through the anterolateral portal (93.5%). Among the patients who underwent anterior ankle arthroscopy, only 4 (6.5%) experienced limited visualization, leading to an insufficient microfracture procedure. In 2 of these 4 patients, we observed challenges in advancing the arthroscopy and other devices owing to the narrow joint space, even with sufficient distraction, whereas the remaining 2 showed infeasibilities derived from the location extending posteriorly beyond the tibial plafond on preoperative magnetic resonance imaging. In contrast, microfracture of posteromedial OLT via posterior ankle arthroscopy was successfully performed in all patients.
Conclusion:
When surgically treating patients with posteromedial OLT, anterior ankle arthroscopy allowed for the successful performance of the microfracture procedure in most cases, unless there was a combined pathology necessitating surgical intervention on the posterior ankle. Posterior ankle arthroscopy can be selectively utilized only for far posteromedial OLT or in patients with narrow joint space, even with sufficient distraction.
Osteochondral lesion of the talus (OLT) is a common condition involving the talus’s articular cartilage and subchondral bone, associated with various ankle pathologies that complicate diagnosis and treatment. Symptoms derived from OLT vary from patient to patient and include pain, swelling, limited range of motion, and mechanical symptoms, such as locking and catching. Although numerous surgical procedures have been developed to address cases in which nonoperative treatment has failed3,14 (eg, bone marrow stimulation, osteochondral autograft or allograft, and autologous chondrocyte implantation), there are no consensus guidelines on the appropriate treatment. 10 However, due to its simplicity and minimal invasiveness, the arthroscopic microfracture technique is the most commonly performed for lesions <1.5 cm2, with consistently reported reliable clinical outcomes.4,6,12,22,23,27
In contrast to the traditional anatomic categorization of medial, central, and lateral divisions, 1 Elias et al 8 introduced the concept of 9 grid zones to provide a more detailed classification of OLT locations. Among these grid zones, a recent systematic review 26 revealed that most OLTs are in the posteromedial and centromedial zones. Our clinical experience is consistent with these previous findings. However, there are instances where OLT is located at the far posteromedial side (Figure 1). Before surgery, uncertainties may arise regarding the feasibility of addressing such cases using anterior ankle arthroscopy. While some previous studies have presented certain indicators for predicting anterior arthroscopic accessibility before surgery,11,24,25 there is limited research on these indicators in conjunction with actual clinical situations.

Osteochondral lesion located on the posteromedial talar dome. Note that the osteochondral lesion (arrows) was located posteromedially relative to the perpendicular line crossing the center of the joint.
Therefore, in this study, we aimed to investigate whether arthroscopic treatment of posteromedial OLT can be accomplished solely through anterior ankle arthroscopy and to compare postoperative outcomes between anterior and posterior ankle arthroscopy approaches. We hypothesized that specific conditions may prompt posterior ankle arthroscopy; under such circumstances, we assumed that the clinical outcomes of posterior ankle arthroscopy would be superior.
Methods
Ethical Considerations
This study was conducted per the principles of the Declaration of Helsinki. Written informed consent was obtained from all enrolled patients. The institution’s ethical review committee approved this study.
Patient Selection
First, we retrospectively collected the data of patients aged >15 years who underwent primary arthroscopic microfracture for symptomatic OLT on the medial talar dome between January 2010 and June 2021. We excluded those with the following criteria: (1) sustained ipsilateral ankle or talar fractures before OLT diagnosis and (2) systemic inflammatory disease (ie, rheumatoid arthritis or gout). Subsequently, based on the initial magnetic resonance imaging (MRI) review, those with OLT situated posterior to the center of the plafond were selected. To achieve this, patients with a minimal anterior sagittal location index (SLI) of >0.5 were included in the study. Furthermore, patients with postoperative follow-up of <24 months were excluded.
Finally, the enrolled patients were divided into 2 groups according to the direction of arthroscopy (anterior or posterior).
Sagittal Location Index
We used a new parameter that can be measured on preoperative MRI to evaluate the position of the OLT relative to the entire tibial plafond area. To acquire homogeneous MRI images, each patient was instructed to lie supine, and the ankles were positioned neutral (dorsiflexed 90°) in the ankle coil with the knee extended (Figure 2A). A 3.0 Tesla MRI (SIGNA Architect; GE Healthcare) was performed with a slice thickness of 3.0 mm and a slice interval of 0.3 mm. In 1 patient, we measured the anterior and posterior SLIs on each T1- and T2-weighted sagittal image that presented a medial OLT (Figure 2B) using the length measurement function in the picture archiving and communication system M6 program (INFINITT Healthcare Platform). The anterior SLI was defined as the length from the anterior plafond to the anterior rim of the OLT divided by the plafond length. In contrast, the posterior SLI was defined as the length from the anterior plafond to the posterior rim of the OLT divided by the plafond length. The anterior or posterior rim of the OLT was defined as the most anterior or posterior margin at the cortical bone level, respectively. To determine the interobserver reliability and intraobserver reproducibility of anterior and posterior SLIs, intraclass correlation coefficients were used for data analysis, with parameters reviewed twice with a 2-month interval between readings. The statistical results of the interobserver reliability and intraobserver reproducibility are presented in Table 1.
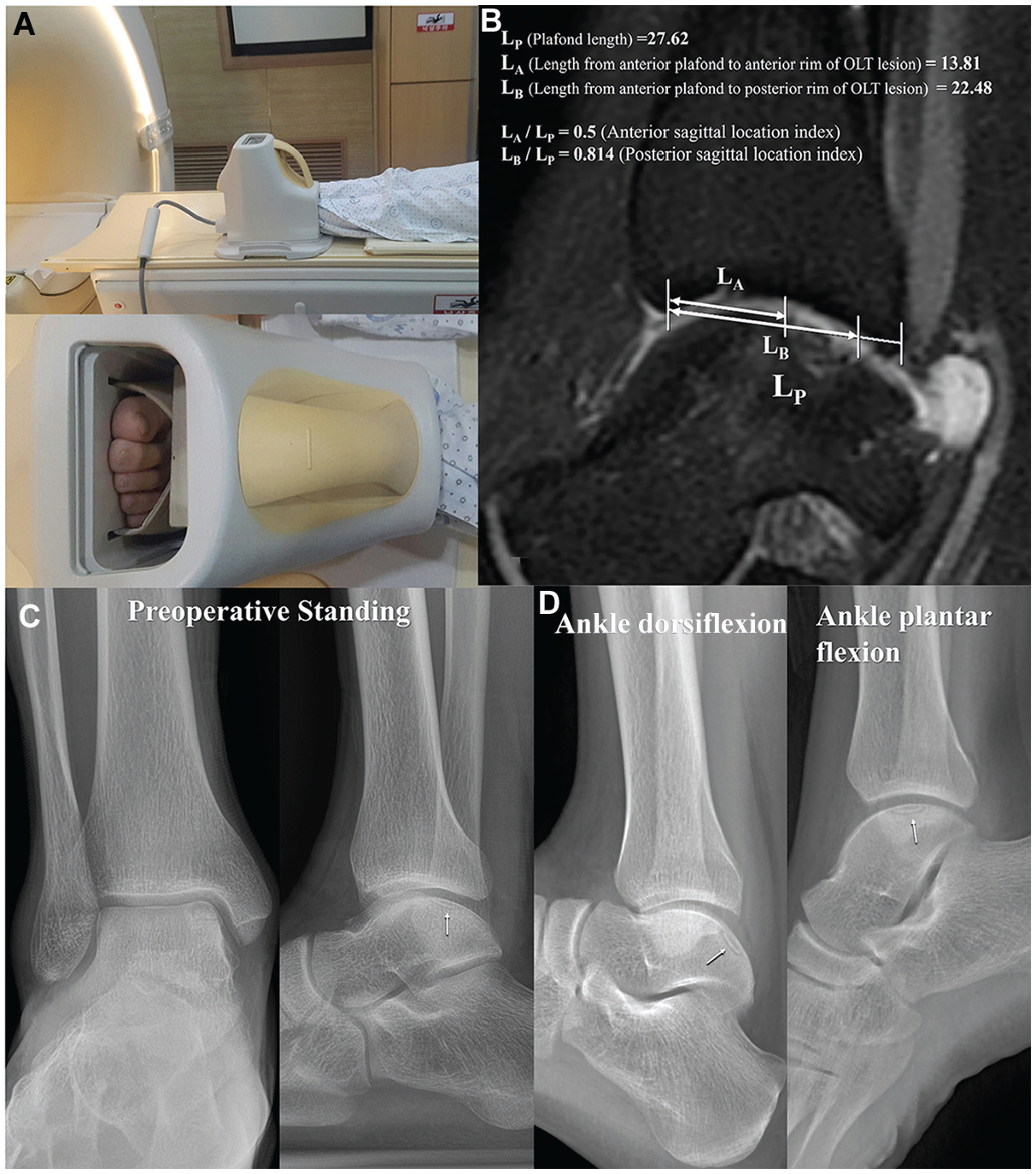
Preoperative imaging evaluations in all patients enrolled in our study. During magnetic resonance imaging, each patient was instructed to lie supine, and the ankles were positioned neutral in the ankle coil with knee extension (A). On a T2-weighted sagittal image, we measured the anterior and posterior SLI (B). The anterior SLI was defined as the length from the anterior plafond to the anterior rim of the OLT divided by the plafond length. In contrast, the posterior SLI was defined as the length from the anterior plafond to the posterior rim of the OLT divided by the plafond length. The anterior or posterior rim of the OLT was defined as the most anterior or posterior margin at the cortical bone level, respectively. Similarly, we evaluated standing ankle anteroposterior, lateral radiographs (C), full plantarflexion, and dorsiflexion radiographs to predict the feasibility of adequately observing a specific lesion during arthroscopy (D). OLT, osteochondral lesion of the talus.
The Statistics for Interobserver Reliability and Intraobserver Reproducibility for the 79 Cases a
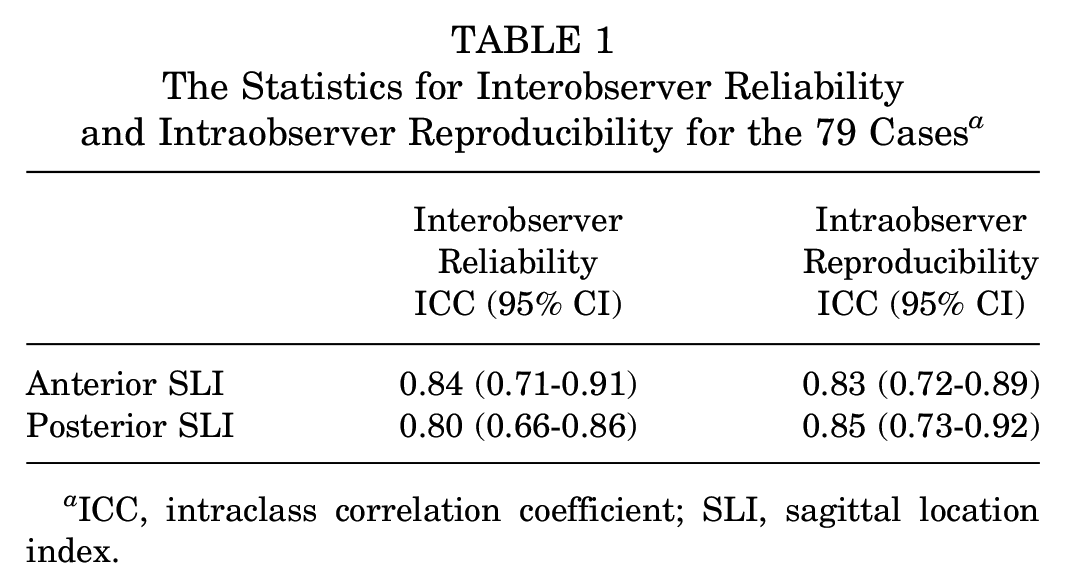
ICC, intraclass correlation coefficient; SLI, sagittal location index.
Preoperative Radiographic Evaluation, Operative Technique, and Aftercare
Preoperative standing ankle anteroposterior and lateral view radiographs were obtained in all patients (Figure 2C). To predict the feasibility of adequately observing a specific lesion during arthroscopy, additional preoperative full plantarflexion and dorsiflexion radiographs were obtained (Figure 2D).2,11 In the preoperative full plantarflexion radiograph, the distance between the anterior margin of the OLT and the anterior margin of the plafond was evaluated, while the dorsiflexion radiographs were utilized to determine whether the posterior margin of the OLT extended beyond the posterior aspect of the plafond.
Two surgeons (J.Y.C and J.S.S) performed all surgeries, and the direction of the scope (anterior or posterior) was determined based on the surgeon’s preference, with reference to anterior and posterior SLI and concomitant pathology. Under general or spinal anesthesia, a pneumatic tourniquet was inflated on the distal thigh with the patient in the supine (anterior ankle arthroscopy) or prone (posterior ankle arthroscopy) position. Ankle joint distraction was performed using a conventional (Figure 3A) or manual (Figure 3B) noninvasive distraction device, based on the surgeon’s preference. In posterior ankle arthroscopy, only the dorsiflexed posture was applied without distractions. Our surgical principle for arthroscopic microfracture was similar to that of the conventional technique, involving the removal of all unstable osteochondral fragments and the creation of holes at regular intervals (3-4 mm) on the subchondral surface using an awl. Standard arthroscopy was 2.7 mm, 30°, and it was sometimes changed to 2.7 mm, 70°, to observe the far posteromedial area. The surgeon captured photographs of all essential procedures and recorded videos during the surgery.

Two modes of distraction for anterior ankle arthroscopy. The surgeon stood behind the patient using a conventional distraction device (A). In the manual distraction technique (B), the surgeon applied a distraction to the joint by leaning backward.
A short-leg splint was applied and maintained for the first postoperative week. Weightbearing was prohibited during the first postoperative week, and partial weightbearing was permitted with crutches or canes for the following 3 weeks. Full weightbearing without a splint was allowed from postoperative week 5, and sports activities were allowed at 3 months postoperatively.
Assessments
By reviewing the medical records, patient data, including age at the time of surgery, sex, affected side (right or left), body mass index (BMI), and degree of preoperative passive ankle dorsiflexion and plantarflexion, were collected. Furthermore, surgical details, including operative time, mode of distraction, and combined operation, were investigated. As mentioned above, we evaluated anterior and posterior SLIs on sagittal MRI images. Among the values from the respective images in a single patient, we chose the minimal value for the anterior SLI and the maximal value for the posterior SLI.
Subsequently, the arthroscopic videos of all enrolled patients were evaluated by 2 experienced orthopaedic surgeons who were not involved in the surgeries (J.H.L. and K.W.P.). They reached a consensus on whether visualization of the most posterior margin of the posteromedial OLT was enabled through the anteromedial or anterolateral portal in the anterior ankle arthroscopy group (posteromedial or posterolateral portal in the posterior ankle arthroscopy group). Similarly, they evaluated whether the awl could reach closer to the anterior or posterior margin of the OLT, determining the feasibility of performing an adequate microfracture technique.
Finally, objective clinical measures were assessed using the Foot and Ankle Ability Measure (FAAM) and its Activities of Daily Living (ADL) and Sports subscales16,21 preoperatively and at the final follow-up. In addition, postoperative complications and secondary operations during the follow-up period were also investigated.
Statistical Analysis
All dependent parameters’ means and standard deviations were calculated using SPSS Version 21 (IBM Corp). Data normality was tested using the Kolmogorov–Smirnov test. Continuous parameters between the anterior and posterior arthroscopy groups were compared using the Mann-Whitney U test, and a chi-square test was used to compare proportional parameters (sex, mode of distraction, feasibility of sufficient microfracture, and postoperative complications). Furthermore, the same statistical analysis was conducted among patients in the anterior ankle arthroscopy group, comparing those who exhibited adequate visualization with those who showed limited visualization. Statistical significance was set at P < .05 in all analyses.
Additionally, we calculated an appropriate effect size for the Mann-Whitney U test using the formula
Results
Characteristics of Total Patients According to the Direction of Arthroscopy
The patient selection algorithm is illustrated in Figure 4. A total of 79 patients were included in this study, with 62 and 17 assigned to the anterior and posterior ankle arthroscopy groups, respectively. For all patients, the mean anterior and posterior SLIs were 0.539 and 0.892, respectively, with a maximum posterior SLI of 1.107, indicating that the posteromedial OLT exceeded the posterior margin of the tibial plafond. Between the 2 groups, age at the time of surgery was significantly greater in the anterior ankle arthroscopy group (P = .001). However, the ratio of women, BMI, preoperative passive ankle range of motion, anterior and posterior SLI on preoperative MRI, and preoperative FAAM scores did not vary between the 2 groups (P > .05). Detailed data are summarized in Table 2.
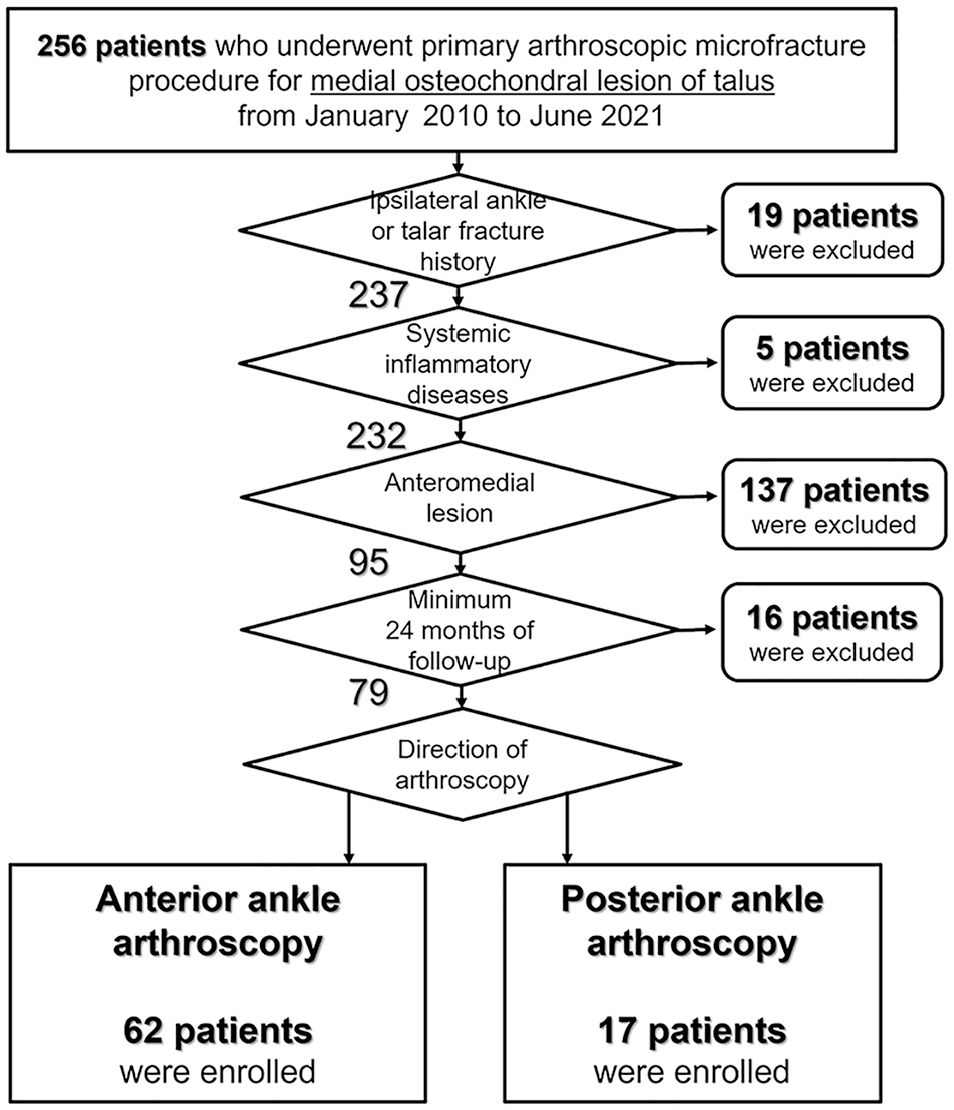
Patient Selection Algorithm.
Patient Characteristics According to the Direction of Arthroscopy a
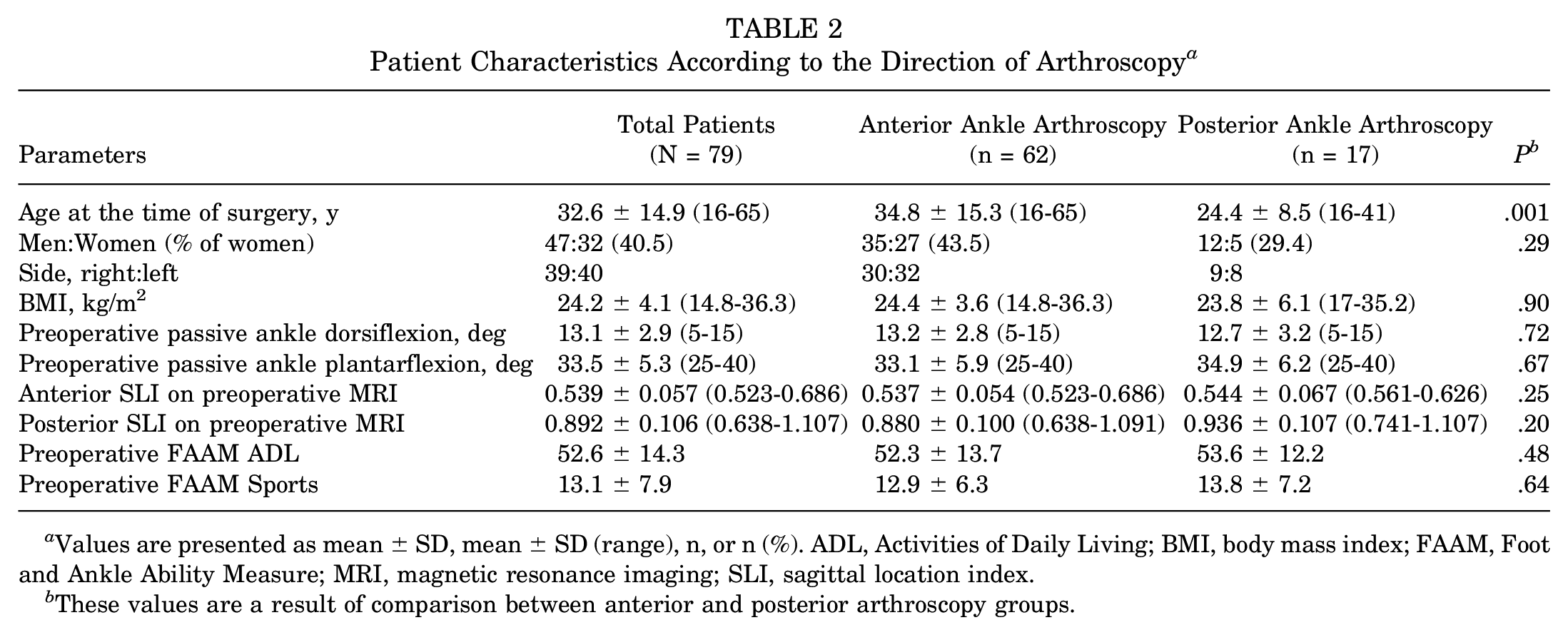
Values are presented as mean ± SD, mean ± SD (range), n, or n (%). ADL, Activities of Daily Living; BMI, body mass index; FAAM, Foot and Ankle Ability Measure; MRI, magnetic resonance imaging; SLI, sagittal location index.
These values are a result of comparison between anterior and posterior arthroscopy groups.
Operative Data Comparison Between Anterior and Posterior Ankle Arthroscopy
Comparing the anterior and posterior ankle arthroscopy groups (Table 3), the operative time was significantly longer in the posterior ankle arthroscopy group (42.38 vs 33.84 minutes; P = .001).
Operative Data Comparison Between the Patients According to the Direction of Ankle Arthroscopy a

Values are presented as mean ± SD, mean ± SD (range), or n (%). ADL, Activities of Daily Living; FAAM, Foot and Ankle Ability Measure; MBP, modified Broström procedure; OLT, osteochondral lesion of the talus.
Regarding visualization of medial OLT via anterior ankle arthroscopy, posteromedial OLT could be fully observed through the anteromedial portal in 79.0% of cases and better observed through the anterolateral portal (93.5%) (Figure 5). Among the patients who underwent anterior ankle arthroscopy, only 4 (6.5%) experienced limited visualization, leading to an insufficient microfracture procedure; therefore, additional posterior ankle arthroscopy was required. In contrast, microfracture via posterior ankle arthroscopy was notably successfully performed in all patients (100%). A posteromedial OLT was observed through the posterolateral portal in all patients (100%). However, the posteromedial portal provided limited visualization in 29.4% of the patients because of the flexor hallucis longus tendon and neurovascular bundle.
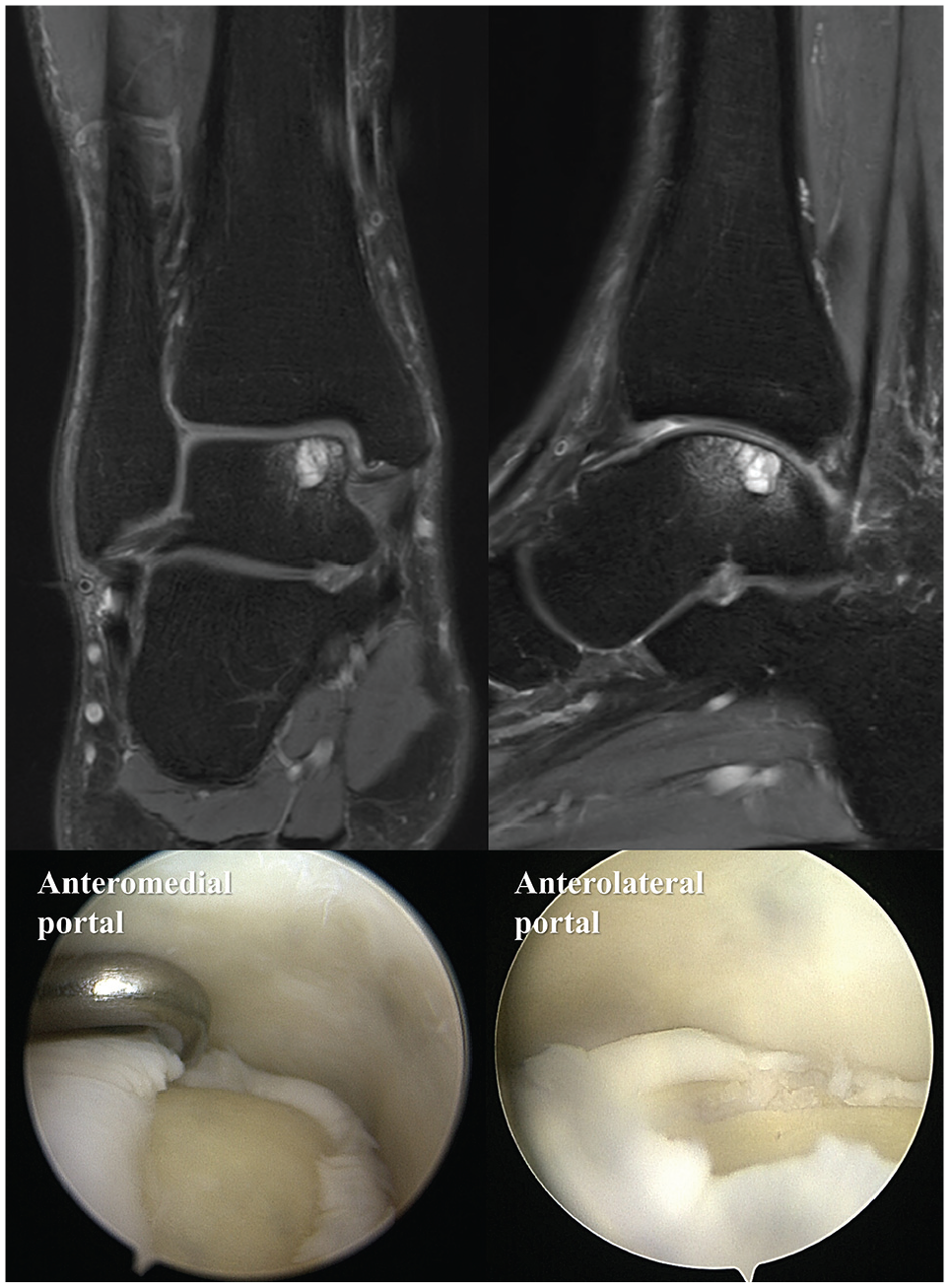
Differences in arthroscopic visualization for posteromedial osteochondral lesions of the talus based on portals during anterior ankle arthroscopy. In most cases, the posterior margin of the posteromedial OLT was better observed through the anterolateral portal than through the anteromedial portal.
The final FAAM ADL and Sports scores did not vary between the 2 groups (P = .68 and P = .82). Persistent postoperative pain requiring a second-look examination or further surgery was observed in 8.1% (anterior) and 5.9% (posterior) of cases (P = .76). Among these cases, a singular occurrence was noted in the anterior ankle arthroscopy group, where pain improved after surgery but recurred after >1 year postoperatively. Subsequently, a secondary operation through posterior ankle arthroscopy was performed in the second year after the initial procedure. After the secondary operation, the postoperative condition was marked by significant pain alleviation.
None of the patients had superficial or deep infections or operation-related neurovascular injuries. The effect size calculation for the difference in FAAM ADL between the 2 groups was 0.617, implying a greater than medium effect size (>0.5).
Characteristics of the Patients With Limited Visualization During the Anterior Ankle Arthroscopy
Although the number of patients with limited visualization during the anterior ankle arthroscopy was limited to 4 of 62 (6.5%) (Table 4), these patients showed a statistically higher proportion of women and higher BMI than patients with adequate visualization (all, P < .05). Furthermore, the anterior SLIs between the 2 groups differed insignificantly (P = .18); however, the posterior SLI was significantly greater in the limited visualization group (P = .001). The posterior SLI in the limited visualization group approached a minimum value close to 1 (0.933), and its mean value exceeded 1 (1.003).
Comparison Between Patients With Adequate Visualization and Those With Limited Visualization During Anterior Ankle Arthroscopy a

Values are presented as mean ± SD (range) or n (%). BMI, body mass index; MRI, magnetic resonance imaging; SLI, sagittal location index.
In 2 arthroscopic videos of the patients with limited visualization, we observed challenges in advancing the arthroscopy and other devices owing to the narrow joint space that did not widen even with sufficient distraction. The remaining 2 videos showed infeasibilities derived from far posterior locations (Figure 6).

Concomitant posterior ankle arthroscopic microfracture after anterior ankle arthroscopy. In the 4 patients who underwent anterior ankle arthroscopic microfracture, additional posterior ankle arthroscopy was required because of limited visualization and insufficient microfracture procedures.
Discussion
Our data suggest that most OLTs on the posteromedial talar dome can be treated using anterior ankle arthroscopic microfracture. To demonstrate this, we have introduced a novel concept called SLI, which could be measured on preoperative MRI and have found that in most cases with an SLI of <1, anterior ankle arthroscopy exhibited insignificant concerns. However, as the location of the lesion shifts further to the posterior margin of the tibial plafond on preoperative MRI (SLI > 1), or the joint space is narrow even with sufficient distraction, an increased likelihood of restricted visibility during anterior ankle arthroscopy is inferred. Although the cases included in this study were limited, satisfactory visualization was achieved for posteromedial OLT using posterior ankle arthroscopy, enabling adequate microfracture procedures. Nevertheless, while 93.5% of posteromedial OLTs were fully visualized through the anterolateral portal during anterior ankle arthroscopy, it is important to note that some lesions treated via the posterior arthroscopy may not have been sufficiently addressed with the anterior arthroscopy alone, potentially resulting in a higher proportion of “inaccessible” lesions than the reported 93.5%. The objective clinical outcomes assessed using the FAAM score showed insignificant differences between anterior and posterior arthroscopy.
The reason for not addressing the approach to posterolateral OLT in our study lies in the excessively higher prevalence of posteromedial OLT. 26 Similarly, because the syndesmotic ligament connects the distal tibia and fibula, a gap derived from this flexible structure enables an approach to posterolateral OLT compared with the posteromedial side. Moreover, sufficient visibility of the posterolateral OLT can be achieved using ankle joint plantarflexion and varus-tilting maneuvers. In contrast, in posteromedial OLT, the medial ankle joint space is relatively narrow, and unless a deltoid ligament insufficiency is present, achieving valgus tilting of the talus is not easy, complicating space acquisition. For the same anatomic reasons, using the anterolateral portal to access the posteromedial OLT provides a more posteromedial approach, enabling greater space for arthroscopic maneuvers.
Two methods have been used traditionally to achieve visibility during anterior ankle arthroscopy: distraction and dorsiflexion. de Leeuw et al 5 have asserted that adopting a slightly dorsiflexed position during anterior ankle arthroscopy reduces the risk of neurovascular bundle damage compared with distraction. However, the dorsiflexion technique is limited to addressing lesions on the anterior side and may be unsuitable for treating central- or posterior-side lesions. 27 Regarding posteromedial OLT, combining the distraction technique with an assistant maximizing ankle plantarflexion can enhance visualization and facilitate a smoother surgical procedure. Distraction assists in expanding the intra-articular space, whereas plantarflexion facilitated by the assistant exposes the posterior and medial aspects of the joint. Similarly, a cadaveric study by Hirtler et al 11 reported that adopting the maximal plantarflexion position aids in accessing the posterior side of the ankle during anterior ankle arthroscopy. Furthermore, they demonstrated that distraction does not benefit posterior ankle arthroscopy. Our perspective is consistent with these findings. Therefore, for posterior ankle arthroscopy, we performed surgeries using only the dorsiflexed posture without distraction. This approach proved effective in achieving visualization of the posteromedial OLT, demonstrating no concerns with visibility.
To anticipate changes in lesion visibility based on ankle movement preoperatively, obtaining ankle full dorsiflexion and plantarflexion radiographs could be helpful.2,11 This might aid cases where the lesion is clearly observed on radiographs; however, according to our experience, in many patients, lesions were not distinctly visible on radiographs, even with plantar- or dorsiflexion, limiting their utility as reference material. Although the majority of patients included in this study did not exhibit preoperative limitations in ankle range of motion, restricted ankle range of motion, particularly in plantarflexion, can present significant challenges in accessing far posteromedial OLT. In addition, we introduced the SLI concept to address this limitation, which could be a consistent and accurate metric for all patients. However, this approach assumes that the ankle position is neutrally maintained (at dorsiflexed 90°) during MRI; thus, it cannot be used in patients where the ankle position cannot be neutral. Moreover, the current slice thickness (3.0 mm) and slice interval (0.3 mm) might cause OLT to be positioned further posteriorly between the images. Future advancements in MRI technology could mitigate these limitations.
Some previous studies have advocated the concept of better visualization through posterior ankle arthroscopy for OLT on the posterior half of the talar dome.13,15,17,20 Although we agree with this notion, we found that the surgical treatment of posteromedial OLT lesions via posterior ankle arthroscopy is technically more challenging than anterior ankle arthroscopy. Particularly on the posteromedial side, where the flexor hallucis longus tendon is observed during posterior ankle arthroscopy, the neurovascular bundle located more medially than the tendon complicates access to OLTs. 28 Additionally, the posterior intermalleolar ligament (IML) becomes tense during ankle dorsiflexion,7,9,18,19 further limiting access to the lesion through the posteromedial portal. The IML has diverse anatomic variations from a thick string to a band with broad medial and apical lateral parts. 18 Based on our surgical experience, addressing posteromedial OLT through posterior ankle arthroscopy often requires a partial resection of the IML at the medial malleolar attachment site. This step was required to access the lesion, and no postoperative complications from this resection were observed (Figure 7). Furthermore, although there were no cases of preoperative ankle dorsiflexion limitation in the patients included in this study, Achilles tendon lengthening or gastrocnemius recession may be necessary before performing posterior ankle arthroscopy in patients with limited ankle dorsiflexion.

Posterior intermalleolar ligament during the posterior ankle arthroscopy. Based on our surgical experience, addressing posteromedial osteochondral lesions of talus using posterior ankle arthroscopy often requires partial resection of the posterior intermalleolar ligament (asterisk) at the medial malleolar attachment site.
Limitations
The limitations of this study include its retrospective design and the disparity in the patient numbers between the anterior and posterior ankle arthroscopy groups. Moreover, there is a potential risk of selection bias, as the direction of arthroscopy was determined by the surgeon’s preference. Notably, even subtle variations in arthroscopic portal placement could significantly change the arthroscopic field of view. However, our study is the first to investigate the correlation between the MRI-based location of posteromedial OLT and its actual visualization during arthroscopy and the feasibility of performing microfracture.
Conclusion
When surgically treating patients with posteromedial OLT, anterior ankle arthroscopy allowed for the successful performance of the microfracture procedure in most cases, unless there was a combined pathology necessitating surgical intervention on the posterior ankle. However, where the OLT extended posteriorly beyond the tibial plafond on preoperative MRI, transitioning to posterior ankle arthroscopy should be considered to address the potential insufficiencies associated with anterior ankle arthroscopy. Caution is advised in patients with inherently narrow joint space, even with sufficient distraction, or limited preoperative ankle range of motion. Because posterior ankle arthroscopic microfracture can yield clinical outcomes similar to those of anterior ankle arthroscopic microfracture, it can be selectively considered when required.
Footnotes
Final revision submitted October 11, 2024; accepted November 11, 2024.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Inje University Ilsan Paik Hospital (No. 2023-09-003).