
Abstract
Background:
The morphological features of the femoral condyles have recently attracted attention as a potential risk factor for knee injuries. However, little is known about whether the femoral condylar morphology is related to posterior cruciate ligament (PCL) injury.
Purpose:
To investigate whether the morphological characteristics of the femoral condyle are risk factors for isolated PCL rupture.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
From the patients who visited the outpatient clinic of our hospital between 2012 and 2022, we included 78 patients with isolated PCL ruptures and 78 age- and sex-matched controls with knee injury but no structural damage evident on magnetic resonance imaging (MRI). The following parameters were assessed using MRI: the lateral femoral condyle and medial femoral condyle height and depth ratio (LFC-H/D, MFC-H/D), notch width index, intercondylar notch angle, the lateral tibial plateau slope, and medial tibial plateau slope (MTPS), and medial tibial depth. Values were compared between these 2 groups using the independent t test and the Mann-Whitney U test. Univariate logistic regression analysis was subsequently performed to identify independent risk factors. Receiver operating characteristic curves were generated for the morphological indicators and the combination of risk factors.
Results:
Patients in the isolated PCL rupture group had significantly lower LFC-H/D (0.49 vs 0.52; P < .001) and MTPS (7.34 vs 8.81; P = .012) values compared with the control group. In sex-specific analyses, both male and female patients with isolated PCL rupture had a significantly lower LFC-H/D (female patients: 0.46 vs 0.52; P < .001; male patients: 0.51 vs 0.52; P = .035). In addition, male patients with PCL rupture had a smaller MTPS (6.74 mm vs 8.79 mm; P = .004). Univariate logistic regression analysis further validated LFC-H/D (odds ratio [OR], <0.001; P < .001) and MTPS (OR, 0.889; P = .014) as risk factors for isolated PCL rupture.
Conclusion:
A decreased LFC-H/D and a reduced MTPS were identified as risk factors for isolated PCL rupture. Sex-specific analysis further suggested that a decreased LFC-H/D was a risk factor for isolated PCL ruptures in both male and female patients, whereas a lower MTPS was a risk factor exclusively in male patients.
Keywords
The posterior cruciate ligament (PCL) is one of the most substantial intra-articular ligaments, playing a crucial role in maintaining normal knee joint biomechanics and functional ability.21,29 Isolated PCL injuries, with an incidence of 1.8 per 10,000 individuals, commonly occur due to traffic accidents or sports-related activities. 36 These injuries reduce knee stability and hinder activity, and raise long-term risks of osteoarthritis and meniscal tears.26,36 Identifying the relationship between morphological parameters and PCL injury is important, as it may aid in assessing an individual's susceptibility and guiding preventive strategies.
Recent attention has focused on the morphological attributes of the femoral condyles as a potential contributing factor to knee injuries.6,10,13,17,20,34,41 This increased interest arises from the recognition that femoral condylar morphology has a critical influence on tibiofemoral biomechanics.11,18 Some studies have reported that an increased lateral femoral condyle (LFC) depth, 34 or a more prominent anterior condyle compared with the flexion radius, 17 is associated with an elevated risk of anterior cruciate ligament (ACL) injury. Furthermore, the morphology of the LFC is correlated with knee joint laxity, multiple ACL reconstruction failures, and concomitant injuries of the anterolateral ligament in patients with ACL injuries.6,13,35
In studies related to the PCL, because of the low incidence of PCL rupture, investigations on the morphological attributes for PCL rupture are scarce, and little attention has been given to the morphology of the femoral condyles. Only Huang et al 20 studied the relationship between the morphology of the medial femoral condyle (MFC) and PCL tears. They concluded that increased asymmetry of medial and lateral slopes and the radius of the posterior circle of the MFC were associated with PCL tears. However, the accuracy of this conclusion may be compromised because of its susceptibility to variations in the size of the patient’s bone structure. As the femoral attachment site of the PCL is located on the MFC, a specific morphology is likely to affect the PCL by altering the knee kinematics. Thus, it remains unclear whether the morphology of the femoral condyles affects PCL rupture.
Therefore, the main objective of this study was to compare the bony morphology of the femoral condyles and the tibial plateau, specifically the femoral condyle height and depth ratio (H/D), between patients with isolated PCL rupture and control patients who sustained a knee injury but showed no structural damage on magnetic resonance imaging (MRI). We hypothesized that a decreased H/D of the femoral condyle would be associated with isolated PCL rupture.
Methods
Study Population
This retrospective case-control study was conducted at our single center. All patients with a knee injury who visited the outpatient clinic of our hospital between 2012 and 2022 were eligible for inclusion. Three senior surgeons (W.L.S., G.Y., and Z.Y.P.) confirmed the diagnosis of PCL rupture and identified any additional injuries based on the patient’s history, physical examination results, and MRI findings. The inclusion criteria for the PCL rupture group were as follows: (1) traumatic PCL rupture (grade 3) 14 as defined by MRI; (2) positive posterior drawer test; and (3) received MRI images within 6 months after the injury. The exclusion criteria were as follows: (1) combined injuries to other knee ligaments (ACL, medial collateral ligament, lateral collateral ligament, or posterolateral corner grades of ≥2); (2) combined meniscal tears (Stoller 39 grade 3); (3) osteoarthritis Kellgren-Lawrence classification grades of ≥2; (4) combined knee fractures, including avulsion fractures; (5) previous surgeries on the affected limb; and (6) combined other pathological or congenital conditions that could potentially affect the anatomic morphology of the knee, such as patellofemoral pain or instability. A total of 1047 patients (739 male and 308 female patients) met the PCL rupture group inclusion criteria. After excluding patients with fractures (n = 241), among whom 58 had tibial avulsion fractures, other ligament injuries (n = 381), meniscal tears (n = 290), osteoarthritis (n = 34), previous surgeries on the affected limb (n = 16), and other conditions that could potentially affect the anatomic morphology of the knee (eg, patellofemoral instability and discoid meniscus, n = 7), a total of 78 patients were eligible for analysis (Figure 1).
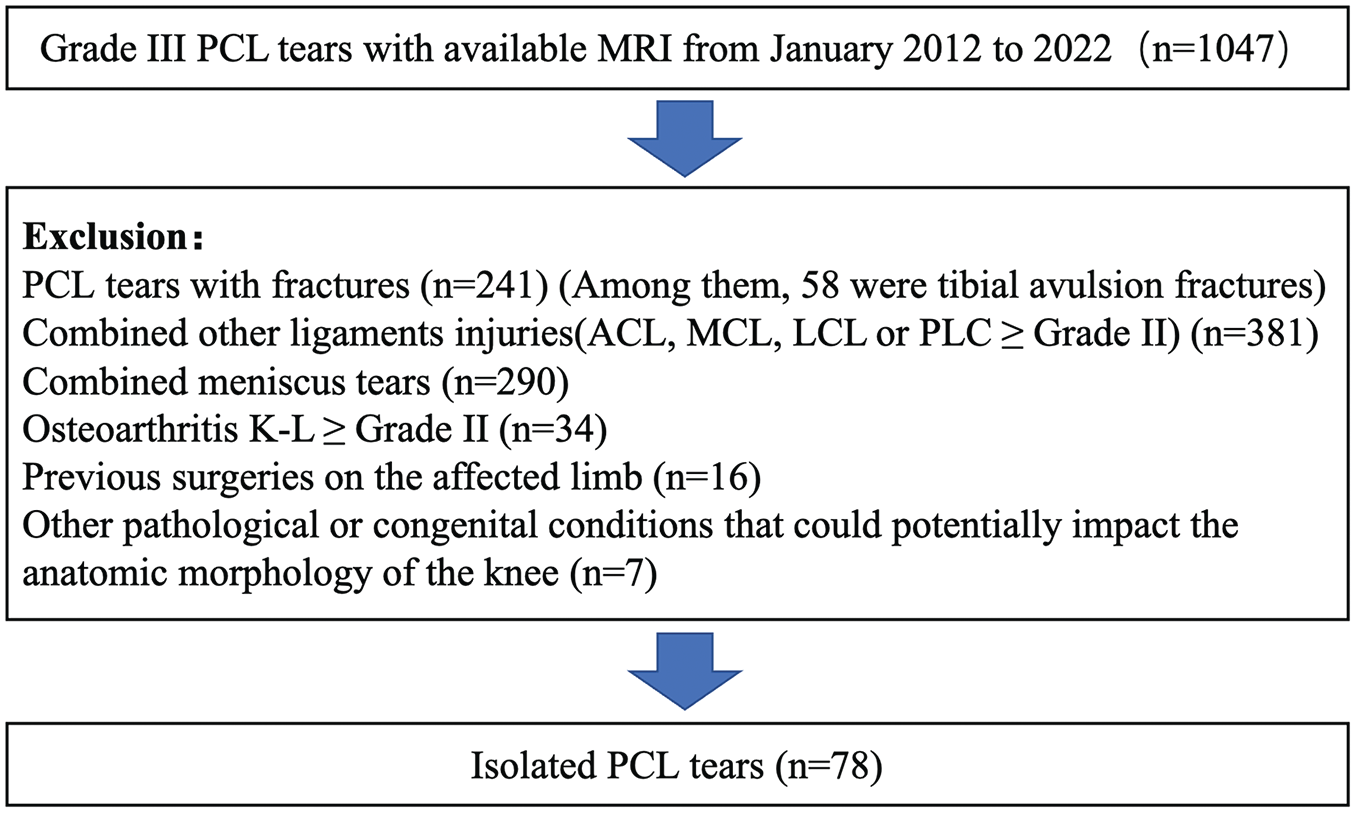
Flowchart of case selection in this study. ACL, anterior cruciate ligament; K-L, Kellgren-Lawrence; LCL, lateral collateral ligament; MCL, medial collateral ligament; MRI, magnetic resonance imaging; PCL, posterior cruciate ligament; PLC, posterolateral corner.
Simultaneously, we included a control group consisting of 78 patients, matched by age and sex to the PCL rupture group. These patients visited the clinic because of knee injuries; however, they did not exhibit any structural damage, such as ligament injuries or meniscal tears, on MRI. The following were the exclusion criteria: (1) physical examination or MRI evidence of ligamentous injury or meniscal tears; (2) osteoarthritis Kellgren-Lawrence grades of ≥2; (3) combined knee fracture, including avulsion fractures; (4) previous surgeries on the affected limb; (5) combined with other pathological or congenital conditions that could potentially effect the anatomic morphology of the knee.
MRI Measurements
All patients were examined using a 1.5-T MRI (Discovery 750; GE Medical Systems), which included sagittal, coronal, and axial sequences containing both T1- and T2-weighted phases. The scan parameters included the following: echo time, 25 to 30 msec; repetition time, 2000 to 3000 msec; and slice thickness, 4 mm with no gap. The images were obtained from our hospital’s Picture Archiving and Communication System. All MRI examinations were conducted with the leg extended in a neutral position, following standard knee MRI protocols. Patients were provided clear and standardized instructions regarding leg positioning to maintain consistency across scans. Furthermore, during the review and measurement of MRI parameters, any cases in which abnormal leg positioning or lower image quality compromised the accuracy of bony structure measurements or introduced significant errors were manually excluded, thereby further reducing bias.
Two experienced orthopedists (C.L.W. and Y.X.Z.), each with >8 years of clinical experience and unaware of the study’s purpose, used Osirix software (an open-source medical imaging software for MacOS; OsiriX) for measurements. If the 2 observers recorded different values, the mean of the 2 values was used. Each observer repeated all measurements after an interval of 1 month, and the inter- and intraobserver reliability results were evaluated using the intraclass correlation coefficient (ICC).
The MFC H/D and LFC H/D were measured according to the method described by Grassi et al 13 (Figure 2B). First, to define the anatomic axis of the femur, the axis tool was aligned with the anterior and posterior cortices of the longest measurable segment of the distal femoral diaphysis as displayed on the MRI and recorded in all sagittal slices (Figure 2A). The MFC-H/D and LFC-H/D were measured on the sagittal slice at the mediolateral centers of the MFC and LFC. After identifying the most posterior portion of the subchondral bone of the femoral condyle with an axial reference, a tangent line parallel to the femoral axis was drawn (line a). The distance between the tangent line and the femoral axis, measured along the perpendicular line (line c), was defined as the depth of the femoral condyle. At the most distal part of the subchondral bone of the femoral condyle, a tangential line was drawn perpendicular to the femoral axis (line b), and the distance between line c and line b was defined as the height of the femoral condyle. The ratios of femoral condyle height and depth were calculated as height/depth. Values approaching 1 approximated a spherical shape, while values approaching 0 approximated a more elliptical shape.

Measurements of the MFC-H/D, LFC-H/D, MTPS, LTPS, and MTD.
The method outlined by Grassi et al 13 was used to estimate the MTPS and lateral tibial plateau slope (LTPS) (Figure 2C). First, the tibial axis was identified in a manner similar to the femoral axis. A segment of the tibial diaphysis, as long as possible, was selected below the tibial tubercle. The axis tool was then fitted to both the anterior and posterior cortices of the tibia, and the resulting tibial axis was recorded in all sagittal slices (Figure 2A). The MTPS and LTPS were measured on the sagittal slice of the mediolateral centers of the medial and lateral tibial plateau. The line connecting the most proximal points of the anterior and posterior margins of the subchondral bone of the tibial plateau is defined as the tangent line (line a). The MTPS and LTPS were the angles between line a and line b (the line perpendicular to the anatomic axis of the tibia).
The medial tibial depth (MTD) was measured on the same plane as the MTPS according to Hashemi et al 15 (Figure 2D). The identical tangent tibial line as seen in the MTPS was depicted (line a), and then a parallel line was traced tangentially to the nadir of the concavity (line b), indicating the lowest point of the subchondral bone. The vertical distance between line a and line b was defined as the MTD.
The measurement of the notch width index (NWI) was based on the method described by Alentorn-Geli et al 1 and Liu et al 27 (Figure 3, A and B). The NWI, which was defined as the ratio of the notch width to the femoral condylar width, was measured in both the coronal and axial planes. For the coronal plane, a tangent was drawn at the distal end of the femoral condyles, while for the axial plane, a tangent was drawn at the posterior end of the femoral condyles. A perpendicular line is then extended through the apex of the intercondylar notch. Furthermore, at the upper one-third of the intercondylar depth, the notch width and the femoral condylar width were measured parallel to the tangent line. The NWI is the ratio of the intercondylar notch width to the femoral condylar width.

Measurements of the NWI and the INA.
The INA was also measured in both the axial and coronal planes, following the method described by Liu et al 27 (Figure 3, A and B). The INA was measured between 2 lines drawn from the highest point of the femoral notch to the medial and lateral edges of the intercondylar notch.
Statistics
All analyses were performed using SPSS Statistics Version 29.0.1.0 (IBM Corp) and the G*Power program (Version 3.1.9.6). The alpha level was set at .05 for determining statistical significance. An a priori sample size calculation was conducted with an α error of 5%, a β error of 95%, and an expected effect size of 0.588 based on preliminary results. The calculation estimated that, to achieve a power of 0.95, a total of 77 patients per group would need to be included in the study. We used a 2-way random effects model to calculate the intra- and interobserver ICC. The normality of the data was assessed using either the Shapiro-Wilk test or the Kolmogorov-Smirnov test based on the sample size (Supplementary Tables S1 and S2), and the homogeneity of variance was evaluated using the Levene test. Continuous demographic variables between the 2 groups were compared using an independent t test, while categorical variables were analyzed using the chi-square test. Depending on the normality of the data, an independent t test or the Mann-Whitney U test was used to compare the mean differences in morphological characteristics. In addition, univariate logistic regressions were performed to analyze the hazard ratios for exposure for each morphological characteristic. The receiver operating characteristic curves were subsequently generated for the morphological indicators as well as the combined risk factors.
Ethical Considerations
The study received approval from the institutional review board of our hospital and was conducted in accordance with the ethical principles outlined in the 1964 Declaration of Helsinki and its subsequent revisions.
Results
Patient Characteristics
There were 78 patients in the PCL rupture group and 78 in the control group. In the PCL rupture group, 35 patients sustained injuries during sports, 37 patients were injured in vehicular accidents, and 6 patients were injured by falls; among these, 12 patients experienced noncontact injuries and 66 patients sustained contact injuries. Each group consisted of 23 women and 55 men. There were no significant differences in age, body mass index, and limb side between the 2 groups (Table 1). Although the distribution of sex ratios in the PCL populations we analyzed was uneven, they were similar to those reported in previous literature, 20,40,27
Demographic Characteristics of PCL Rupture and Control Groups a

Data are reported as mean degrees ± SD. BMI, body mass index; PCL, posterior cruciate ligament.
Independent t test.
Chi-square test.
MRI Measurements
The LFC-H/D was significantly smaller in the PCL rupture group (0.49 ± 0.05; P < .001) than in the control group (0.52 ± 0.04) (Figure 4A). The MTPS was also significantly smaller in the PCL rupture group (7.34°± 4.24°; P = .012) than in the control group (8.81°± 2.71°) (Figure 4B). No significant disparity was detected between the 2 groups for the MFC-H/D, axial NWI, axial INA, coronal NWI, coronal INA, LTPS, and MTD (Table 2).

Tukey box and whisker plots demonstrated the differences in measured parameters of the 2 groups. Line, median; box, interquartile range; *P < .05; **P < .01; ***P < .001; ****P < .0001. The whiskers indicate the minimum and maximum values. The line within the box indicates the median, and the top and bottom of the box indicate the interquartile range. LFC-H/D, lateral femoral condyle height/depth ratio; MTD, medial tibial depth; MTPS, medial tibial plateau slope; NWI, notch width index.
Morphological Characteristics of PCL Rupture and Control Groups a
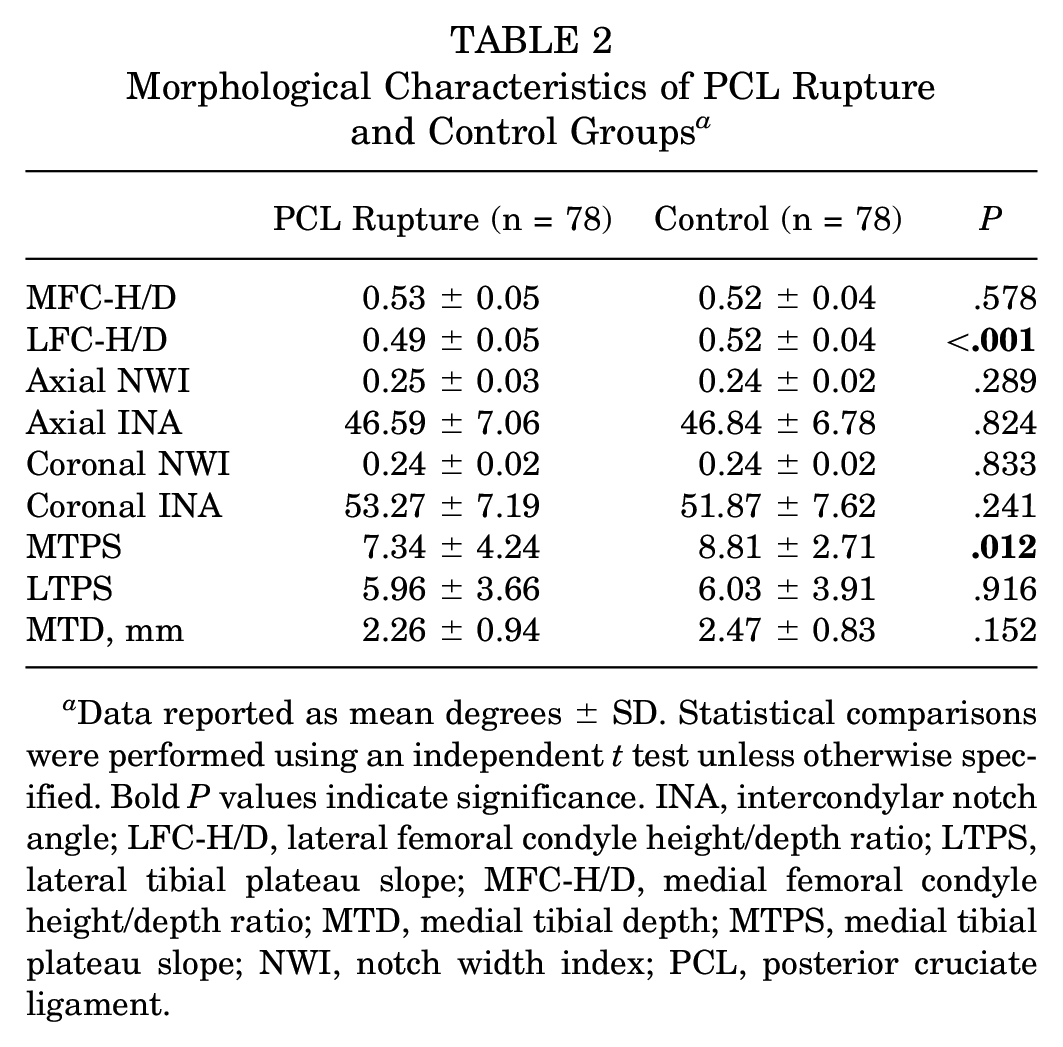
Data reported as mean degrees ± SD. Statistical comparisons were performed using an independent t test unless otherwise specified. Bold P values indicate significance. INA, intercondylar notch angle; LFC-H/D, lateral femoral condyle height/depth ratio; LTPS, lateral tibial plateau slope; MFC-H/D, medial femoral condyle height/depth ratio; MTD, medial tibial depth; MTPS, medial tibial plateau slope; NWI, notch width index; PCL, posterior cruciate ligament.
Sex-specific subgroup analysis revealed that in female patients, the LFC-H/D was significantly smaller in the PCL rupture group (0.46 ± 0.04; P < .001) compared with the control group (0.52 ± 0.03 mm) (Figure 4C). In male patients, the LFC-H/D was also significantly smaller in the PCL rupture group (0.51 ± 0.04; P = .035) compared with the control group (0.52 ± 0.04 mm) (Figure 4D). Unlike in female patients, the MTPS of male patients was significantly smaller in the PCL rupture group (6.74°± 4.27°; P = .004) compared with the control group (8.79°± 2.81°) (Figure 4E and Table 3).
Morphological Characteristics of Female and Male Subgroups a

Data reported as mean degrees ± SD. Bold P values indicate significance. Statistical comparisons were performed using an independent t test unless otherwise specified. INA, intercondylar notch angle; LFC-H/D, lateral femoral condyle height/depth ratio; LTPS, lateral tibial plateau slope; MFC-H/D, medial femoral condyle height/depth ratio; MTPS, medial tibial plateau slope; MTD, medial tibial depth; NWI, notch width index; PCL, posterior cruciate ligament.
In addition, subgroup analysis based on the injury mechanism in isolated PCL-injured knees revealed that the LFC-H/D (0.47 ± 0.04 vs 0.50 ± 0.05; P = .041) (Figure 4F), axial NWI (0.23 ± 0.03 vs 0.25 ± 0.03; P = .028) (Figure 4G), and MTD (1.69 ± 0.83 vs 2.36 ± 0.94; P = .021) (Figure 4H) were significantly smaller in the noncontact injury group compared with the contact injury group (Table 4).
Morphological Characteristics of Contact and Noncontact Isolated PCL Injury a
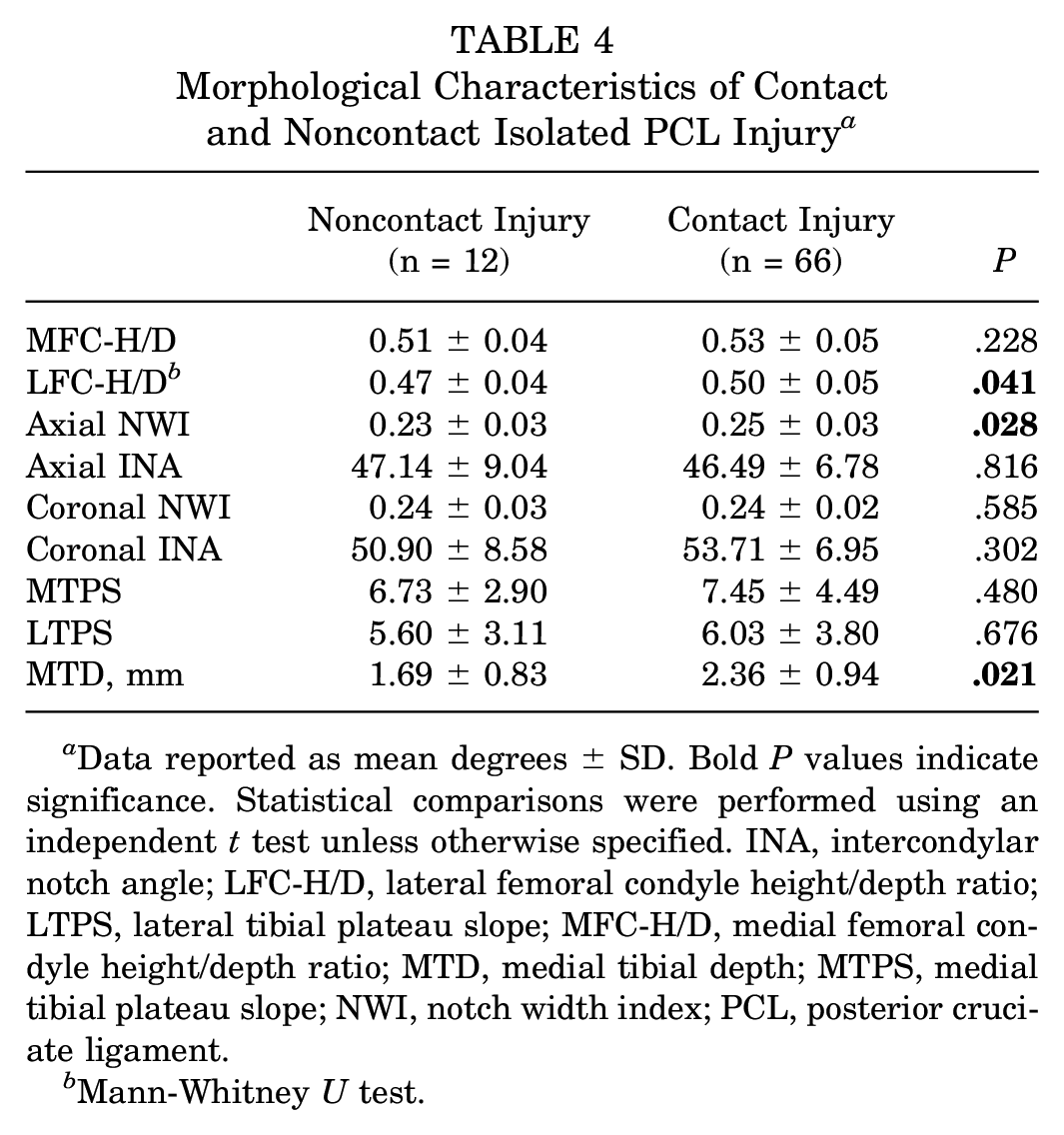
Data reported as mean degrees ± SD. Bold P values indicate significance. Statistical comparisons were performed using an independent t test unless otherwise specified. INA, intercondylar notch angle; LFC-H/D, lateral femoral condyle height/depth ratio; LTPS, lateral tibial plateau slope; MFC-H/D, medial femoral condyle height/depth ratio; MTD, medial tibial depth; MTPS, medial tibial plateau slope; NWI, notch width index; PCL, posterior cruciate ligament.
Mann-Whitney U test.
The univariate logistic regression analysis revealed 2 significant independent predictors for isolated PCL rupture: LFC-H/D (odds ratio [OR], <0.001; P < .001) and MTPS (OR, 0.889; P = .014). For female patients, only the LFC-H/D (OR, <0.001; P < .001) was identified as an independent factor for isolated PCL rupture. In male patients, the LFC-H/D (OR, <0.001; P = .039) and the MTPS (OR, 0.851; P = .006) were identified as independent factors for isolated PCL rupture (Table 5).
Logistic Regression Analysis for Predictor Variables a

Bold P values indicate significance (P < .05). LFC-H/D, lateral femoral condyle height/depth ratio; MTPS, medial tibial plateau slope; OR, odds ratio.
The area under the curve (AUC) of the LFC-H/D and the MTPS was 0.676 (95% CI, 0.592-0.76) and 0.629 (95% CI, 0.54-0.718), respectively (Figure 5, A and B). The AUC for the combination of LFC-H/D and MTPS was 0.698 (95% CI, 0.615-0.78) (Figure 5C).

ROC curve of the (A) LFC-H/D, (B) MTPS, and (C) the combination of the risk factors. AUC, area under the curve; LFC-H/D, lateral femoral condyle height/depth ratio; MTPS, medial tibial plateau slope; ROC, receiver operating characteristic.
The interobserver reliability of the LFC-H/D was determined to be 0.89 (95% CI, 0.78-0.94), while the intraobserver reliability was found to be 0.94 (95% CI, 0.86-0.98). The other measurements showed a minimum interobserver reliability of 0.83 and an intraobserver reliability of 0.88 (Table 6).
Inter- and Intraobserver Reliability Analysis a
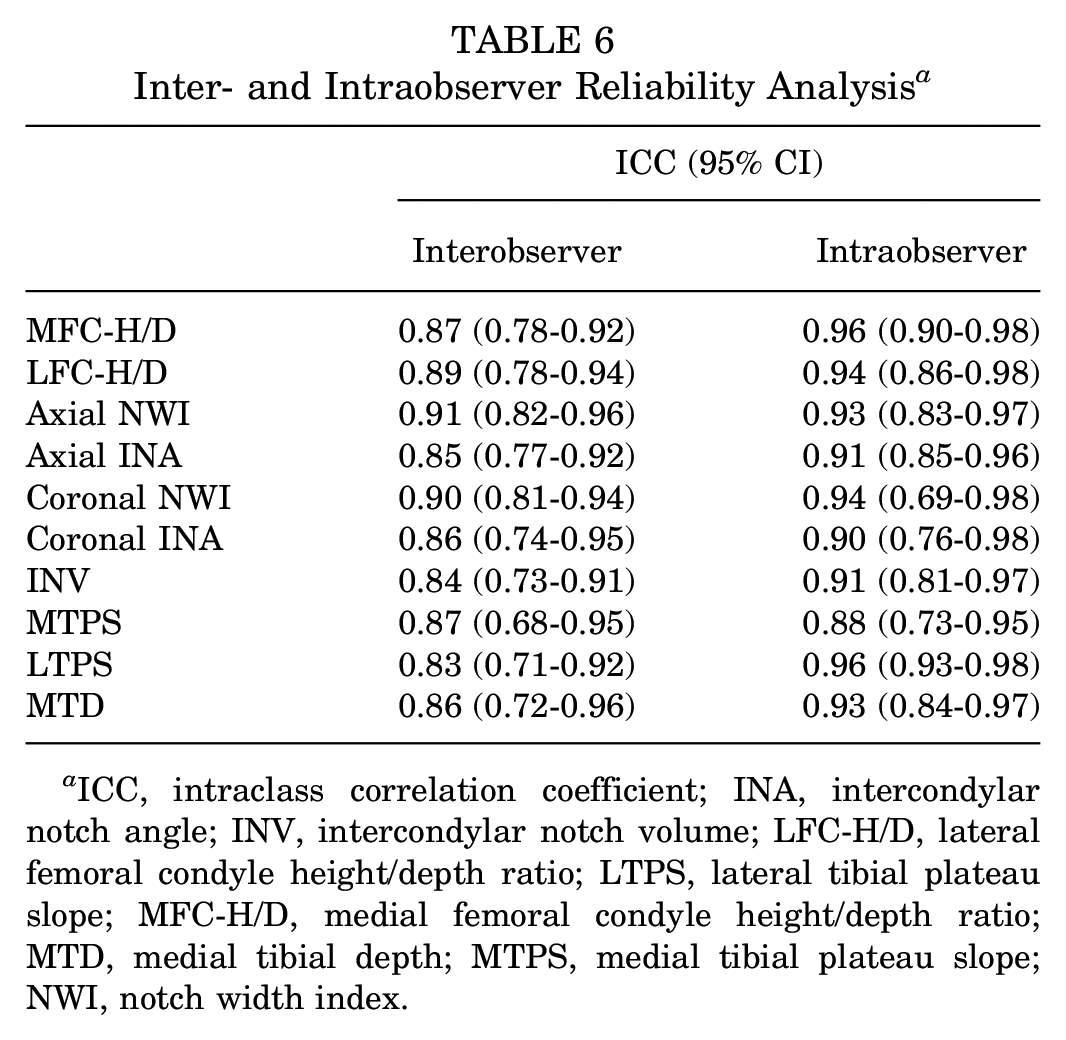
ICC, intraclass correlation coefficient; INA, intercondylar notch angle; INV, intercondylar notch volume; LFC-H/D, lateral femoral condyle height/depth ratio; LTPS, lateral tibial plateau slope; MFC-H/D, medial femoral condyle height/depth ratio; MTD, medial tibial depth; MTPS, medial tibial plateau slope; NWI, notch width index.
Discussion
The main finding of this study was the correlation between a decreased LFC-H/D and the occurrence of an isolated PCL rupture. The decreased MTPS was identified as another independent risk factor for isolated PCL rupture. In addition, sex-specific distinctions were noted, with the MTPS not being a risk factor for women.
The LFC-H/D is a measurement parameter that depicts distal femoral morphology, with a smaller LFC-H/D indicating a more elliptical shape of the LFC. 13 The distal morphology of the femur, particularly the LFC, has been demonstrated to have a significant effect on knee joint kinematics and rotational stability.11,18,35 Regarding its role in PCL injuries, Huang et al 20 investigated the relationship between the shape of the MFC and PCL injuries by measuring the posterior circle and inferior circle of the MFC; however, they did not study the morphology of the LFC.
Our research identified that a reduced LFC-H/D was associated with an increased risk of isolated PCL rupture, and the LFC-H/D was significantly lower in the noncontact injury group compared with the contact injury group. Potential mechanisms underlying these associations may include alterations in tibiofemoral contact dynamics, increased strain on the PCL, and changes in muscle contraction forces.11,12,34
During knee extension, if the LFC-H/D is smaller, the flatter distal portion of the LFC will make contact with the lateral tibial plateau, which facilitates sliding rather than rolling of the LFC. 10 Moreover, a smaller LFC-H/D, indicating a more elliptical and nonisometric LFC, reduces the contact area between the femoral condyle and the tibia, thereby increasing the tendency for knee joint instability. 35 As one of the primary ligaments responsible for maintaining knee stability, the PCL is at significantly higher risk of injury under these conditions. 22
The PCL originates from the lateral aspect of the MFC and inserts into the central posterior aspect of the tibial plateau. 43 Physiologically, the length of the PCL increases during knee flexion.24,43 In this position, a relatively deeper femoral condyle increases the distance between the femoral and tibial insertion sites, further elongating the PCL. Excessive tension on the PCL during flexion potentially increases the risk of PCL injury. 20
Previous literature7,30 reported that the gastrocnemius muscle pulls the tibia posteriorly, and its contraction can increase PCL strain at flexion angles of >30°. The lateral head of the gastrocnemius muscle originates above the lateral condyle of the femur and descends, passing over the LFC. 4 Consequently, changes in the morphology of the LFC can potentially alter the force vector of the gastrocnemius muscle, increasing the posterior force exerted on the tibia during muscle contraction. 12 Specifically, an elliptical LFC may cause the gastrocnemius muscle to curve more posteriorly at its femoral origin, enhancing the posterior vector force on the tibia as it extends downward to insert into the calcaneus.
Our study did not find an association between the MFC-H/D and isolated PCL rupture, which may be attributed to the distinct functional roles of the LFC and the MFC during tibiofemoral joint movement. 11 The MFC can be considered as a sphere, forming a ball-and-socket-like joint with the medial tibia, primarily facilitating flexion and longitudinal rotation, with minimal translation. The LFC not only allows flexion but also permits anterior-posterior sliding. 11 Considering that the primary function of the PCL is to restrain posterior tibial displacement relative to the femur, 29 any kinematic abnormalities resulting from the morphological abnormalities of the LFC are more likely to contribute to PCL injury. To a certain extent, this explained the findings of Huang et al, 20 which indicated that the ratio of the radius of the posterior and inferior MFC circles did not exhibit a significant correlation with PCL injury.
Similar to the findings of Li et al, 25 and Huang et al, 20 this study also found that a smaller MTPS was a risk factor for isolated PCL rupture. A flatter medial tibial plateau can restrict the anterior inclination of the tibia, leading to increased force on the PCL. 38 However, in female patients, there was only a tendency for MTPS without significant differences, which was consistent with the findings of Huang et al, 20 probably because of variations in physiological anatomical structures and injury mechanisms between sexes.19,32 Furthermore, our study found no significant differences in MTD between the isolated PCL rupture group and the control group. This result contrasts with the findings of Huang et al, 20 which may be attributed to the higher proportion of contact injuries in our injury group. The external forces associated with contact injuries might be sufficient to override the limiting capacity of the medial tibial plateau. 20 Our subgroup analysis also confirmed that the MTD was significantly higher in the contact injury group compared with the noncontact injury group.
The study did not find a correlation between intercondylar notch morphology and isolated PCL rupture. This finding aligned with the conclusions of Liu et al, 27 who reported that patients with PCL rupture did not show a stenotic intercondylar notch. Similarly, van Kuijk et al 40 also found no significant difference in NWI between the PCL injury group and the control group. However, our findings differed from those of Huang et al, 20 who found that decreased coronal NWI was associated with an increased incidence of PCL intrasubstance tearing and tibial avulsion fractures. This discrepancy may be due to different inclusion criteria between the 2 studies; our experimental group included patients with isolated PCL injuries and excluded those with concomitant meniscal injuries, whereas their study included patients with associated meniscal injuries. Notably, meniscal injuries themselves have been reported to be associated with lower NWI values, possibly because of a smaller intercondylar notch increasing the risks of impingement on the posterior root of the medial meniscus.2,42 The reason why the morphology of the intercondylar notch is associated with ACL injuries but not with PCL injuries may be attributed to the differing anatomic positions and courses of the 2 ligaments within the notch.16,29 The influence of notch impingement on the risk of PCL rupture during knee flexion may be relatively minor.29,43
This study examined the relationship between the morphology of the LFC and PCL injury. The measure used in this study, namely, the femoral condyle H/D ratio, effectively quantified the morphology of the femoral condyle. Because of its ratio-based nature, the femoral condyle was less susceptible to the influence of the patient’s bone structure size. In addition, the inclusion of 78 isolated PCL injuries from 1047 patients with PCL injury, which excluded the confounding effects of fractures and other injuries, ensured the reliability of the conclusions drawn in this study.
By identifying high-risk patients based on the risk factors found in our study, clinicians can customize early interventions to reduce the risk of injury. For those with a smaller LFC-H/D, it is advisable to implement early quadriceps strengthening exercises, proprioceptive training, and the use of knee braces or other orthotic devices to enhance knee joint stability.5,28,33 For athletes, targeted training in sports techniques and posture can help maintain proper alignment during knee flexion activities like squatting and jumping, reducing stress on the elongated PCL. 9 Furthermore, specific stretching and massage of the gastrocnemius muscle can help reduce muscle tension and prevent excessive contraction.8,31 For patients with an exceptionally low MTPS, anterior opening wedge high tibial osteotomies can be combined with PCL reconstruction to increase the tibial plateau slope, thereby reducing posterior tibial translation. 23
We acknowledge the limitations of our study. First, because of the retrospective design of this study, certain confounding factors were not controlled, such as injury mechanism and the type of footwear worn during the injury. Second, given that most PCL injuries are contact-related,3,20 the proportion of patients with noncontact injury included in this study is relatively low. Future research could focus on this specific population for a more detailed analysis. Third, the study only assessed the anatomic morphology of the knee joint among Asian patients, and there may be variations in the bony structures among different ethnicities. Last, the study had a limited number of female participants, as PCL injuries are predominantly observed in men. 37
Conclusion
A decreased LFC-H/D and a reduced MTPS were identified as risk factors for isolated PCL rupture. Sex-specific analysis further suggested that a decreased LFC-H/D was a risk factor for isolated PCL ruptures in both men and women, whereas a lower MTPS was a risk factor exclusively in men.
Footnotes
Final revision submitted March 12, 2025; accepted March 31, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the Gansu Provincial Health Bureau Science Foundation of China (22JR11RA197). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The Second Affiliated Hospital, School of Medicine, Zhejiang University (R2022-1003/I20221199).