
Abstract
Background:
Hip arthroscopy remains one of the fastest-growing procedures in orthopaedic surgery, with an 85% increase in procedure frequency from 2011 to 2018. There is agreement on the need for physical therapy after hip arthroscopy and a strong literature base on various modalities that can be implemented to aid recovery. Yet, little continuity exists among institutions on rehabilitation prescriptions.
Purpose:
To identify common trends and the vast variability in publicly available physical therapy protocols after hip arthroscopy.
Study Design:
Cross-sectional study.
Methods:
Inclusion in protocol collection was based on the 175 Accreditation Council for Graduate Medical Education–accredited orthopaedic surgery programs and their affiliated surgeons. Rehabilitation protocols were collected utilizing a web-based search engine (Google.com) using the input “[Insert Program Name] hip arthroscopy rehabilitation protocol.” Each protocol was analyzed for variability in brace utilization, weightbearing restrictions, range of motion (ROM) restrictions, exercise implementation, and duration for each phase and modality of rehabilitation.
Results:
Of the 175 programs, only 36 unique rehabilitation protocols were publicly available from 41 (23.4%) programs. Thirteen (36.1%) protocols required brace usage with a mean duration of 3.2 weeks. Weightbearing restrictions had the largest variability, ranging from full body weight to just 20 pounds of pressure. ROM restrictions were inconsistent among the 36 protocols with varying views on duration and degree of ROM restriction for various hip rotations. Exercise implementation varied from phase to phase of recovery with little agreement between protocols. Variability in time to return to various levels of activity also existed among the protocols analyzed.
Conclusion:
There is a significant amount of variability that exists within the publicly available hip arthroscopy rehabilitation protocols concerning brace wear, weightbearing restrictions, ROM restrictions, and exercise prescriptions. More work must be done to standardize rehabilitation protocols based on defined criteria and identify which factors have the greatest effect on patient recovery to maximize patient outcomes.
Arthroscopic procedures are on the rise in all surgical specialties, especially in orthopaedic procedures. The utilization of hip arthroscopy has increased drastically in the last decade, with one analysis displaying an 85% increase in hip arthroscopies from 2011 to 2018. 20 The most common indications for hip arthroscopy are femoroacetabular impingement, labral pathologies, hip laxity/instability, and loose bodies. 15 Numerous factors influence whether a patient will recover well from hip arthroscopy if they later need revision, or ultimately receive total hip arthroplasty. While there are many factors correlated with patient outcomes after hip arthroscopy, physical therapy (PT) is a specific factor that is part of the rehabilitation process, as the utilization of PT within weeks after hip arthroscopy has been shown to improve patient outcomes.11,14
While there generally is agreement among hip arthroscopists on the need for PT after hip arthroscopy, the exact regimen and restrictions are extremely variable. While there is a wealth of literature on rehabilitation protocols after hip arthroscopy, there is little continuity in the criteria to determine the rehabilitation approach for patient recovery.1,5,8,17 Previous work has been done by Cvetanovich et al 4 to examine the variability of rehabilitation after hip arthroscopy protocols utilizing the Hip Preservation Society (formerly International Society for Hip Arthroscopy [ISHA]) “Find a Surgeon” tool, which demonstrated the widespread variability in available protocols.
The existing variability in PT rehabilitation protocols after hip arthroscopy is a potential point of concern for surgeons and patients, as this inconsistency may lead to confusion and potentially suboptimal outcomes. The purpose of this study was to evaluate the variability in hip arthroscopy rehabilitation protocols that exist within the 175 Accreditation Council for Graduate Medical Education (ACGME)–accredited orthopaedic residency programs. ACGME-accredited institutions and their surgeons were selected as the primary inclusion criteria to highlight the potential trends in rehabilitation protocols among educational institutions, as these programs are shaping the principles of the future orthopaedic surgeons in the United States. We hypothesized that the available protocols would vary with little consensus concerning weightbearing restrictions, brace wear, range of motion (ROM) restrictions, and specific timing and progression of exercises. This study aimed to better inform those who treat patients with hip arthroscopy by identifying the specific variability that exists between protocols.
Methods
This project was deemed exempt from institutional review board approval as no human participants were involved in this study. The eligible programs for comparison were the 175 ACGME-accredited programs in orthopaedic surgery, along with publicly available protocols from surgeons affiliated with a given ACGME program. Affiliated surgeons were included if they had clear affiliation with an ACGME program on their website and appeared in the web-based search for their given institution. The list of all eligible programs was collected from the ACGME website. Rehabilitation protocols were collected utilizing a web-based search engine (Google.com) using the input “[Insert Program Name] hip arthroscopy rehabilitation protocol.” The search yielded the publicly available protocols that anyone with access to a web-based search engine could obtain. A total of 41 protocols were obtained, with 36 unique protocols that were extracted for data analysis. Five protocols were not included as they were duplicates from hospital systems with multiple ACGME-accredited training locations. Protocol titles ranged from generic hip arthroscopy rehabilitation to specific procedures such as labral repair.
Each rehabilitation protocol was analyzed across multiple domains, including recommendations on brace wear, weightbearing restrictions, ROM restrictions and milestones, progression of rehabilitation exercises, and progression toward return to activity. The data from the protocols were collected and analyzed using Excel (Microsoft Corp). Excel was utilized to analyze the mean implementation of various rehabilitation modalities (time in weeks, weight in pounds/body weight percentage, and degrees of motion restriction) along with the standard deviation across the available protocols. These means and standard deviations were utilized to compare the various protocols on brace wear, weightbearing restrictions, ROM restrictions, and exercise implementation.
Results
Of the 175 ACGME-accredited orthopaedic surgery programs, 41 (23.4%) programs had publicly available rehabilitation protocols with 36 unique protocols included for analysis.
Postoperative Brace Wear and Weightbearing Restrictions
Of the 36 unique protocols analyzed, brace wear and weightbearing protocols have the greatest interinstitutional variability. Regarding brace wear, 13 (36.1%) institutions designate brace wear as a requirement of their rehabilitation protocol, and 4 (11.1%) programs state that the utilization is at the discretion of the surgeon. The final 19 (52.8%) protocols suggest no brace wear is required as part of the hip arthroscopy rehabilitation process. Only 8 of the 13 available protocols outline specific time frames for brace utilization. These 8 protocols suggested brace utilization for a mean of 3.2 weeks (SD, 1.1 weeks). Of these 8 protocols, only 2 also include degree limitations for the brace. These 2 protocols stated restrictions from 0° to 90° with no specification on directionality, and the other program set the requirements to 0° of extension, 70° of flexion, and 10° of abduction.
Weightbearing restrictions set forth by the various protocols presented with a high degree of variability. All 36 protocols referenced weightbearing restrictions in some capacity. One of the 36 available protocols did not detail any specifics with regard to weight restriction but just stated there should be some form of weightbearing restrictions. Three different protocols did not specify the duration of the restriction.
While some protocols defined weightbearing restrictions in terms of percentage of body weight, others used a specific number of pounds. Twelve (33.3%) protocols directly state weightbearing restrictions in terms of pounds. These protocols indicated a maximal weightbearing load of 20 pounds. Ten (27.8%) defined the weightbearing restriction in terms of percentage of body weight. Thirteen (36.1%) protocols did not specify a specific weight restriction but instead stated weightbearing as tolerated or as partial. One (2.8%) protocol stated that there should be 3 weeks of weightbearing restrictions but did not specify what that weightbearing restriction should be. To standardize for this discrepancy to obtain a mean weight restriction in pounds, the protocols that were reported as body weight percentages were converted to pounds utilizing the CDC’s mean weight for men and women in the United States, which comes out to be 199.8 pounds for men and 170.8 pounds for women (total mean for the United States, 185.3 pounds). 7 The 10 programs that stated weightbearing restrictions in terms of body weight percentage had a mean weightbearing restriction of 35% of body weight. When converted to pounds based on the mean American weight, this equates to 65 pounds of prescribed weightbearing. This is >3 times the mean weight restriction set forth by the 12 protocols that define the restriction in pounds (65 vs 20 pounds).
The duration of weight restriction was included in 33 (91.7%) of the protocols available. Variability in the duration of restriction was also widespread, with weightbearing restrictions ranging from 1 week up to 8 weeks, with the mean duration of restriction being 3.4 weeks (SD, 1.5 weeks) weeks.
ROM Restrictions and Progression
Some common hip ROM movements listed in rehabilitation protocols are hip flexion, internal rotation (IR), and external rotation (ER). The greatest concordance between protocols was found within the ROM flexion limitations. Of the 36 protocols, 29 (80.6%) highlight progression goals or restrictions regarding flexion ROM (Figure 1). Early in the recovery process, there was the least agreement on the limitations in flexion, with a mean limitation of 81° (SD, 26°) in the first week and 78° (SD, 32°) during the second week. As the weeks of recovery progress, there is increased agreement between protocols in the rehabilitation prescription for hip flexion ROM compared with the first 2 weeks of the recovery protocol (Figure 2).

Percentage of protocols that address various planes of range of motion in the physical therapy rehabilitation protocol.
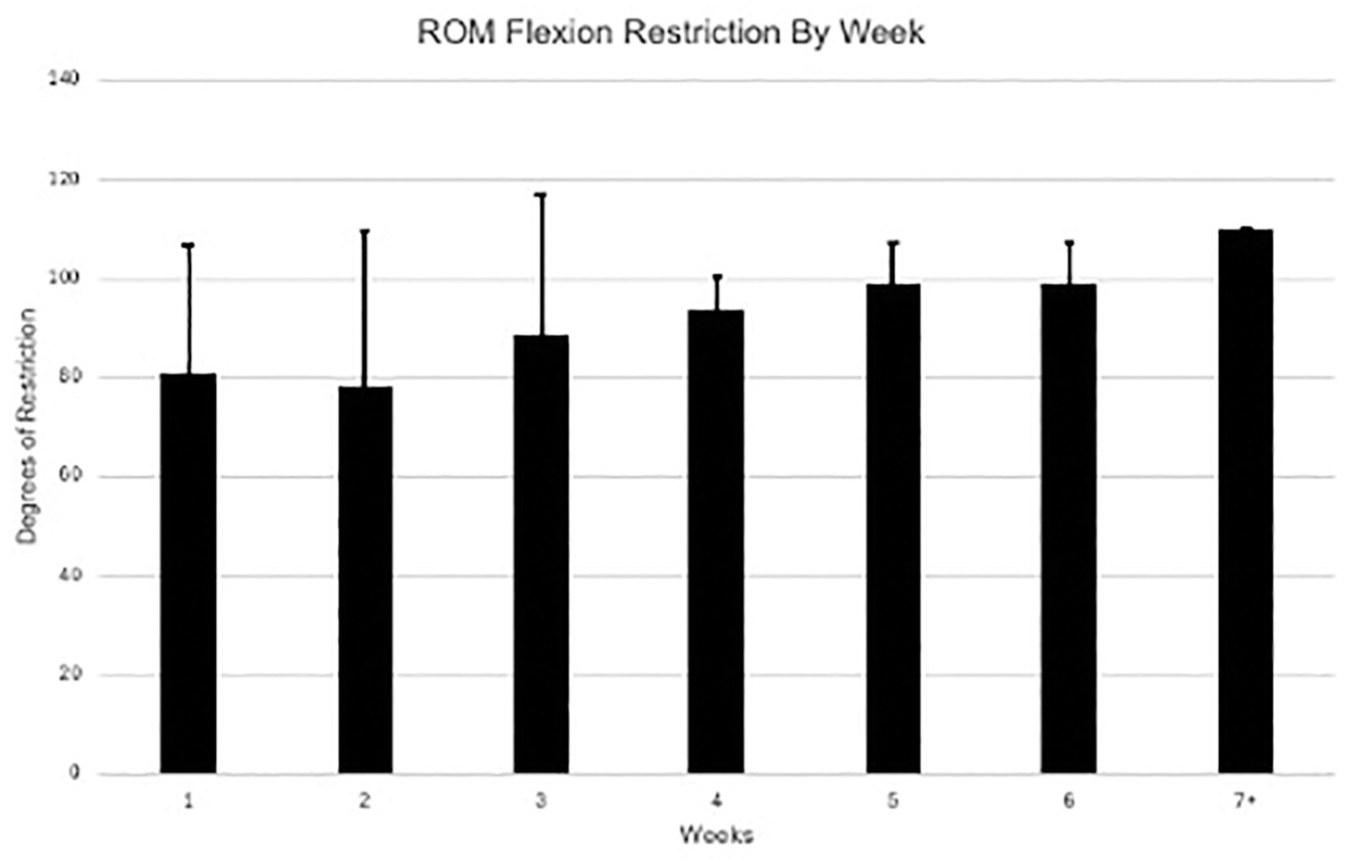
The mean degree of restriction prescribed for flexion range of motion (ROM). Data were aggregated for weeks 7 to 12 as protocols stopped differentiating limitations weekly. Error bars represent standard deviation.
ER and IR ROM displayed some of the greatest variability in ROM metrics addressed in the protocols. There were 19 (52.8%) protocols that stated IR ROM restrictions and 26 (72.2%) protocols that stated ER ROM restrictions (Figure 2). When comparing protocols, the first phase of rehabilitation had the most variability in IR ROM limitations. The limitation of IR ROM during the first phase of recovery ranged from 0° to no limitation. Four protocols stated no limitation or full ROM on IR ROM. The mean restriction among protocols that had defined degrees of restriction was 27.3° (SD, 29.6°) of motion restriction. ER during early rehabilitation was less variable, with motion limitations ranging from 0° to 30° of ER ROM with a mean of 13.2° (SD, 13.5°). IR and ER restrictions were addressed by most programs (52.8% for IR and 72.2% for ER) for the first phase of recovery, yet only 4 (11.1%) programs addressed the ROM goals for IR and ER for the third phase of rehabilitation progression.
Therapeutic and Resistance Exercises
Eight exercises were analyzed across the available protocols. The 8 exercises were leg press, stationary bike, step up/step down, squat progression, pool therapy/water walking, pelvic tilts, ankle pumps, and clam shells. These exercises highlight an array of the exercises commonly utilized from the early stages of mobility to the later stages of recovery where regaining strength becomes a priority.
The most prescribed exercise was stationary biking, with 86% of protocols utilizing the modality. The least utilized exercise was ankle pumps, with 36% of protocols outlining its utilization in the early phases of the recovery process (Figure 3). Stationary biking, ankle pumps, and pelvic tilts were all initiated during the first week, on average. The mean time for initiating pool therapy and clam shells was close to the third week postoperatively. Leg press, step up/step down, and squat progressions were utilized around the fourth week (Table 1).

Percentage of protocols that utilize a given therapeutic or resistance exercise as part of the rehabilitation prescription.
Postoperative Times of Initiation and Termination of Rehabilitation Exercises a

Data are presented in weeks as mean ± SD.
Discussion
Our study found that there is substantial variability in the publicly available rehabilitation protocols after hip arthroscopy concerning bracing, weightbearing, ROM restrictions, and exercise implementation. The most consistent recommendations across the 36 available protocols are an emphasis on some form of weightbearing restriction during the recovery process, with all 36 protocols highlighting the need for load restrictions on the affected leg. There was strong concordance in the necessity for stationary bike utilization through the rehabilitation process, as the vast majority (86%) of protocols highlighted this modality. Beyond these commonalities, there was a large amount of variability in all phases of the rehabilitation process, with little agreement on the time frame of various restrictions and progression landmarks. This inconsistency among rehabilitation protocols is not limited to hip arthroscopy and can be found among other orthopaedic procedures as well. 16
A study on the variability of rehabilitation protocols after hip arthroscopy has previously been done, but the time gap and expanding knowledge regarding hip arthroscopy illustrate differences compared with the current work. 4 While the previous study examined programs across North America through the ISHA “Find a Surgeon” tool, our work focused on the ACGME-accredited orthopaedic surgery residency programs and their affiliated surgeons. Furthermore, most of the protocols obtained from the previous study were from personal surgeons’ websites. Personal websites were only included based on their explicit ties to an ACGME-accredited program and contingent on their website appearing when the web-based search terms were used for their respective program. Private practice or nonacademic personal websites were not included in this study, as we aimed to delineate the variability within the academic medicine space regarding the variability and scarcely available rehabilitation protocols after hip arthroscopy.
When comparing the results of the previous study to our findings, there is an 8-year time gap between the 2 data collection periods, enabling the evaluation of the progression and changing views of practitioners when it comes to rehabilitation modalities after hip arthroscopy. One example from the previous study found that 55% of protocols designated brace usage after surgery, while our search found that only 36% of protocols utilized bracing. This highlights the trend in recent studies that have found no differences in outcomes after hip arthroscopy with bracing compared to without bracing. 10 Many of the ROM progressions are consistent across the 2 studies, along with the inclusion of several therapeutic/resistance exercises, but the time gap between the 2 papers highlights the changing landscape of rehabilitation after hip arthroscopy.
There is a great deal of work being done by orthopaedic surgeons, hip specialists, and physical therapists to establish some guidelines that can provide a framework for health care providers who may be unsure of the best postoperative course after hip arthroscopy. For example, in 2019 there was a panel of physical therapists and orthopaedic surgeons that collaborated on a set of guidelines for the care surrounding femoroacetabular impingement syndrome with the support of the ISHA. 18 The collective focused on preoperative care, surgical management, nonsurgical management, and postoperative recovery. The paper detailing the group’s outlooks on hip arthroscopy provides some suggestions on different restrictions in the various phases of recovery, but ultimately recognizes that there is little scientific research being done to discover the most optimal means of recovery. The views on hip arthroscopy rehabilitation are based on surgeon experience and guidance by colleagues, which confirms the necessity for further studies to identify the modalities and guidelines that lead to optimal recovery. Furthermore, several other PT-guided papers have examined rehabilitation, but these studies also came to the conclusion that further work must be done, and these studies are becoming increasingly dated (2014 and 2020).2,3
While there was general agreement on postoperative weightbearing restriction, the length of modified weightbearing and the amount of force allowed were inconsistent. The length of the restrictions ranged from 1 to 6 weeks, depending on the protocol, and some protocols utilize a percentage of a patient’s body weight, while others use pounds of weight. A recent systematic review performed by Hemstock et al 9 examined if there are adequate data to conclusively determine weightbearing protocols after hip arthroscopy. The group concluded there was insufficient comparative evidence to make specific weightbearing restrictions. 9 This lack of definitive data may be an important reason for there being little agreement on the duration and degree of weightbearing restrictions after hip arthroscopy.
There was strong disagreement over the utilization of brace wear in all the protocols, with 19 protocols calling for no brace utilization, 13 requiring brace usage, and 4 protocols suggesting brace wear is at the discretion of the surgeon. A study by Johnson et al 10 found that elimination of the postoperative brace after hip arthroscopy does not increase the risk of complications. The patients who did not utilize a brace did not experience any statistically significant differences in pain or complications at 2- and 6-week follow-up appointments. 10 Multiple other studies have corroborated the data set forth by Johnson et al, and the literature points to the fact that there is no definitive benefit to postoperative bracing after hip arthroscopy.6,12,13,19 There is still a need for continuity to develop on the matter across the orthopaedic surgeon community, as shown by the variability in the rehabilitation prescriptions.
It is well accepted by the orthopaedic community that PT is a vital part of the rehabilitation process after hip arthroscopy, and the integration of PT in the weeks after the procedure drastically improves patient outcomes.11,14 While research into rehabilitation after hip arthroscopy is expanding, our study shows that there is little agreement across publicly available rehabilitation protocols set forth by the ACGME training programs and their affiliated surgeons. There has been evidence that formal PT is useful postoperatively, as a 2016 study assessing the 2-year outcomes of patients who followed a criteria-based PT protocol after hip arthroscopy found that these patients had excellent outcomes. 5 While this study did not definitively advocate a particular protocol, it did suggest that extensive collaboration between surgeons and therapists is paramount.
This study is not without limitations. Although 175 ACGME-accredited orthopaedic residency programs and their affiliated surgeons were included in the study, only 36 unique rehabilitation protocols were publicly available for analysis by the researchers. While this relatively small number may limit some of the ability to analyze protocols, it further underscores the lack of availability and consistency across academic programs in the United States. Furthermore, the percentage of weightbearing restrictions and pounds of weightbearing restrictions are difficult to compare and would be unique to each patient. We attempted to normalize this by comparing the mean body weight, but these normalized body weights may not apply to every patient, as their actual weight may vary dramatically from the mean. A range of procedural rehabilitation protocols were included. There was no variation when comparing generic rehabilitation protocols versus case-specific protocols (eg, hip arthroscopy rehabilitation vs labral repair rehabilitation).
Conclusion
There is a significant amount of variability that exists within the publicly available hip arthroscopy rehabilitation protocols concerning brace wear, weightbearing restrictions, ROM restrictions, and exercise prescriptions. More work must be done to standardize rehabilitation protocols based on defined criteria and to identify which factors have the greatest effect on patient recovery to maximize patient outcomes.
Footnotes
Final revision submitted February 17, 2025; accepted March 28, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: T.B.E. has received educational support from Smith & Nephew, Arthrex, and Gentleman Orthopedic Solutions and hospitality payments from Exatech, Pacira Pharmaceuticals, IlluminOss Medical, Stryker Corporation, Prime Surgical, Next Science, Zimmer Biomet Holdings, Encore Medical, LinkBio Corp, Linvatec Corporation, and OSSIO. E.W.B. has received educational support from Prime Surgical; consulting fees from LinkBio Corp; and hospitality payments from Smith & Nephew, Stryker Corporation, Arthrex, LinkBio Corp, Zimmer Biomet Holdings, IlluminOss Medical, Next Science, and Orthofix Medical. A.M.M. has received educational support from Prime Surgical and Arthrex; honoraria from Fidia Pharma USA; nonconsulting fees from Arthrex; a grant from DJO; consulting fees from Stryker Corporation and Miach Orthopaedics; and hospitality payments from Prime Surgical, Fidia Pharma USA, Smith & Nephew, Ethicon US, Flexion Therapeutics, Pacira Therapeutics, Innovation Technologies, IlluminOss Medical, Bioventus, Exatech, DePuy Synthes Sales, Zimmer Biomet Holdings, Next Science, Linvatec Corporation, and Orthofix Medical. A.J.C. has received educational support from Supreme Orthopedic Systems, Arthrex, Smith & Nephew, and Prime Surgical; consulting fees, nonconsulting fees, and a grant from Arthrex; and hospitality payments from FX Shoulder USA, Smith & Nephew, Vericel Corporation, Stryker Corporation, IlluminOss Medical, Prime Surgical, Exatech, DePuy Synthes Sales, Zimmer Biomet Holdings, Linvatec Corporation, and Orthofix Medical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.