
Abstract
Background:
High-level athletes who undergo hip arthroscopy for femoroacetabular impingement syndrome (FAIS) return to sport (RTS) at a high rate. However, the influence of athlete-specific factors, including sport, sex, and clinical and surgical findings, on the time to RTS remains unclear.
Purpose:
To determine if the time to RTS clearance is influenced by sport and sex in collegiate athletes following hip arthroscopy, as well as determine if the time to RTS is impacted by clinical and surgical factors.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
In total, 62 Division I collegiate athletes (26 female; 89 hips) who underwent hip arthroscopy for FAIS between January 2017 and July 2024 were included in this analysis of routinely collected health and performance data. Demographic information included sport, sex, age, body mass index, and whether unilateral or staged bilateral hip arthroscopy was performed. Preoperative and intraoperative findings included radiographic measures of hip morphology, the number of anchors used during labral repair, and chondral injury grade. RTS clearance was defined as the date of clearance from a member of the medical team for return to full activity. Time-to-event analyses examined the relationship between time to RTS clearance and athlete-specific factors.
Results:
There were significant differences in time to RTS clearance among different sports (P = .002). Athletes in track (median [IQR]: 3.4 [3.2-4.2] months) and wrestling (3.8 [3.2-3.9] months) required less time to RTS clearance than athletes in football (4.9 [4.4-5.4] months; P = .003 and P = .04, respectively). No significant difference was identified between female (4.2 [3.5-5.6] months) and male (4.8 [3.6-5.5] months) athletes regarding median time to RTS clearance (hazard ratio, 0.91; 95% CI, 0.51-1.61; P = .74). No clinical or surgical factors significantly impacted time to RTS clearance (all P values >.05).
Conclusion:
Collegiate athletes in wrestling and track who undergo hip arthroscopy for FAIS demonstrated quicker time to RTS clearance than those in football. There was no difference in time to RTS clearance between sexes. Despite variations in clinical and surgical factors, no variables within these categories significantly impacted time to RTS clearance.
Femoroacetabular impingement syndrome (FAIS) is a common cause of hip pain and dysfunction, 1 particularly among athletes.13,14,26 When symptoms become debilitating and conservative measures are not successful,7,9,19 hip arthroscopy is the leading treatment to manage hip pain and enable athletes to return to sport (RTS). 8 Following hip arthroscopy, it is estimated that 76% to 98% of athletes resume sport participation.4,12,24 However, timing of RTS is poorly understood.4,20 There is a need to better define the typical time to RTS for different sports and sexes, as well as the influence of clinical and surgical factors, to help set patient expectations and inform coaching staffs on athlete availability.
Specifically for female athletes, literature is lacking on outcomes of RTS rates and time to RTS following hip arthroscopy.22,31 A systematic review that assessed the influence of sex on RTS participation after hip arthroscopy identified 14 articles in which female sex was a negative predictor and 6 articles in which female sex was a positive predictor for RTS. 22 The authors described large variation across the reviewed studies due to high heterogeneity of the data, with a lack of randomization and insufficiency of high-level evidence without standardized measures for RTS. 22 Another article identified that female soccer athletes were more likely to discontinue sport after surgery than their male counterparts. 20 Similar to the overall population, while some information is available on the RTS rate for female patients following hip arthroscopy for FAIS,15,28,41 little is known about the specific time to RTS for female collegiate athletes.
Clinical and surgical factors such as demographics, preoperative clinical findings, intraoperative findings, and surgical procedure details may influence an athlete's RTS ability. Specifically, individuals with milder degrees of preoperative radiographic joint space narrowing,23,37 labral repair rather than debridement, 37 and less severe chondral injury 33 are more likely to have better postoperative outcomes. Further, larger radiographic α angles from cam- or mixed-type FAIS are significant predictors of the degree of hip chondral damage identified intraoperatively.21,32,36 Additionally, a higher RTS rate has been observed for athletes with less severe cartilage injury 28 and for those who had a capsular closure performed during hip arthroscopy. 6 A lower RTS rate was observed in athletes with a longer duration of preoperative symptoms 38 and in those who had persistent hip pain postoperatively. 40 While these findings reflect differences in RTS rates or patient-reported outcomes of pain and function, clinical and surgical factors have not been examined relative to how they may affect the time to RTS after hip arthroscopy.
In this study, we examined time to RTS clearance rather than time to return to competition to provide a standardized and clinically meaningful metric reflecting medical readiness for unrestricted participation. This approach minimized variability that may be introduced by factors unrelated to recovery, such as off-season surgeries, delayed competition schedules, or strategic redshirting. Additionally, this ensures that comparisons across sports and sexes are based on recovery progress and provider clearance.
The primary purpose of this study was to identify how time to RTS clearance varies by sport and sex in collegiate athletes following hip arthroscopy for FAIS. In addition, we sought to determine if time to RTS clearance was impacted by clinical or surgical factors. The primary study hypothesis was that athletes in sports requiring cutting, pivoting, or deep angles of hip flexion would have a longer time to RTS clearance after hip arthroscopy compared to athletes in linear sports with less hip flexion requirements. A secondary hypothesis was that athletes with more severe clinical and surgical factors would have a longer time to RTS clearance.
Methods
Participants
Routinely collected health care and performance data were reviewed from the Badger Athletic Performance database and medical records of National Collegiate Athletic Association Division I athletes who underwent hip arthroscopy surgery for the treatment of FAIS between January 2017 and July 2024. To be included, athletes had to be participating in sport at the University of Wisconsin (UW)–Madison prior to surgical intervention and be undergoing hip arthroscopy for FAIS without concomitant procedures (eg, core muscle repair, hip abductor repair). Athletes were excluded if they had preoperatively planned to discontinue sport participation, had a lower extremity surgical procedure within 6 months prior to hip arthroscopy, or if clinical documentation from an external institution could not be accessed. This records review was approved by the university's Health Science Institutional Review Board.
Surgical Technique and Rehabilitation
Nearly all athletes (90.3%) were treated by 1 of 2 surgeons at UW-Health. For these athletes, hip arthroscopy was performed under either general or spinal anesthesia, and they were positioned supine on a hip traction table. Adequate joint distraction was confirmed using fluoroscopy. Standard anterolateral and mid-anterior portals (under fluoroscopic guidance and direct visualization, respectively) were established, and access to the hip joint was achieved via an interportal capsulotomy. Acetabuloplasty and subspine decompression were performed when indicated for pincer or subspine impingement, respectively. Labral repair was performed when tissue quality permitted; otherwise, limited debridement was performed. Following labral management, either the use of suspension sutures or a T-capsulotomy was performed to access the peripheral compartment, and femoral neck osteochondroplasty was performed to address cam morphology. Periodic fluoroscopic imaging and dynamic arthroscopic assessment were used to confirm adequate bony resection. Capsular repair was performed in all cases at the conclusion of the procedure.
All athletes completed their rehabilitation at the same facility, with most following the same postoperative rehabilitation guidelines. A typical postoperative course included 2 to 3 weeks of 20% weightbearing with bilateral crutches, with weaning of crutch use once full weightbearing was achieved without a limp. Impact and high-intensity activity were avoided until a minimum of 12 weeks postoperatively. Clearance for RTS was based on consistent clinical benchmarks across sports, including symptom resolution and the ability to perform sport-specific drills without symptom provocation.
Health History Data Collection
Patient demographic information, including sport, sex, age, body mass index, and clearance to RTS date, was extracted. The clearance to RTS date was also used to determine whether the surgery occurred during the competitive sport season (in-season) or not (off-season), as well as calculate the duration of time from the date of surgery until the beginning of the next competitive sport season. Preoperative findings included the α angle from a modified Dunn view radiograph,23,37 the lateral center-edge angle from an anterior-posterior radiograph,16,42 and Beighton's score. 3 Surgical procedure details included whether a femoroplasty and/or acetabuloplasty was performed, if labral repair was indicated, the surgical limb, and whether it was a unilateral procedure or part of a staged bilateral procedure. Intraoperative findings included the number of anchors used for labral repair, if applicable, to provide a surrogate for the size of the labral tear present and the grade of chondral injury based on the Modified Outerbridge Classification System.11,29,30 The time between procedures was also noted for individuals who underwent staged bilateral hip arthroscopy for symptomatic FAIS.
RTS Time Frame
The primary outcome of interest was the duration of time to RTS clearance following hip arthroscopy surgery. Two electronic medical records (the local hospital system and the internal athletics’ sports medicine department) were used to identify RTS information. For athletes with records in both systems, the RTS clearance date was cross-referenced to ensure consistency between dates. Clearance to RTS was defined as a noted date of clearance from a member of the medical team (surgeon, physical therapist, athletic trainer) for return to full activity/sport with no restrictions. If an athlete underwent bilateral hip arthroscopy to treat FAIS within a 6-month period, the time to RTS clearance was reported as the duration between the second procedure and clearance for full participation. If an athlete underwent bilateral hip arthroscopy with >6 months between operations, the time to RTS clearance for that athlete was only reported within the unilateral group for the primary surgery.
Statistical Analysis
Standard descriptive statistics (mean ± standard deviation or frequency [percentage], as appropriate) were used to describe the athlete population. Time to RTS clearance is reported as median [IQR]. For sports that had at least 3 athletes total (female and male combined), pairwise comparisons to examine the relationship between time to RTS clearance and sport were performed using the log-rank test with Bonferroni adjustment. For all athletes, time-to-event analyses provided univariable Cox proportional hazards models to examine the relationship between time to RTS clearance and variables in demographic, preoperative, intraoperative, and surgical procedure details. For bilateral surgeries, only details pertaining to the second surgical procedure were reported and used in the statistical analyses.
Kaplan-Meier survival curves were used to visualize time-to-event analyses by sport and sex. If an athlete did not have an explicit RTS clearance date noted in the clinical documentation, the most recent note indicating that they had not yet been cleared for RTS was used for right-censoring in the analysis. Right-censoring was applied in all time-to-event analyses, including Kaplan-Meier survival curves and Cox proportional hazards models. If any univariable models identified significant associations, a multivariable model was developed using all significant variables. Univariable model results are reported as hazard ratios (HRs) and 95% confidence intervals. The level of significance was set at α≤ .05. Statistical analyses were performed using R (version 4.4.1; R Core Team).
Results
After the record review process, 62 Division I collegiate athletes (27 athletes having staged bilateral hip arthroscopy) were identified for inclusion (Figure 1). Athlete-specific factors, including demographics, preoperative findings, surgical procedure details, and intraoperative findings, are reported in Table 1. Nearly all athletes (90.3%) were treated by 1 of 2 surgeons at UW-Health. Fifty-three athletes had an explicit RTS clearance date documented. Nine athletes were right-censored during the analysis as they did not have an explicit RTS clearance date. Among these 9 athletes, 3 returned to sport at UW without an explicit RTS clearance date, 2 returned to sport at a professional or national team level upon graduating, 2 returned to sport after transferring to another institution, 1 returned to sport at UW after recovering from a subsequent knee injury that occurred during hip arthroscopy postoperative rehabilitation, and 1 discontinued sport participation entirely. Overall, 98.4% of athletes returned to sport after hip arthroscopy for FAIS, with 100% of male athletes and 96.2% of female athletes returning. Of this cohort, the median time to RTS was 4.4 [IQR, 3.5-5.5] months.
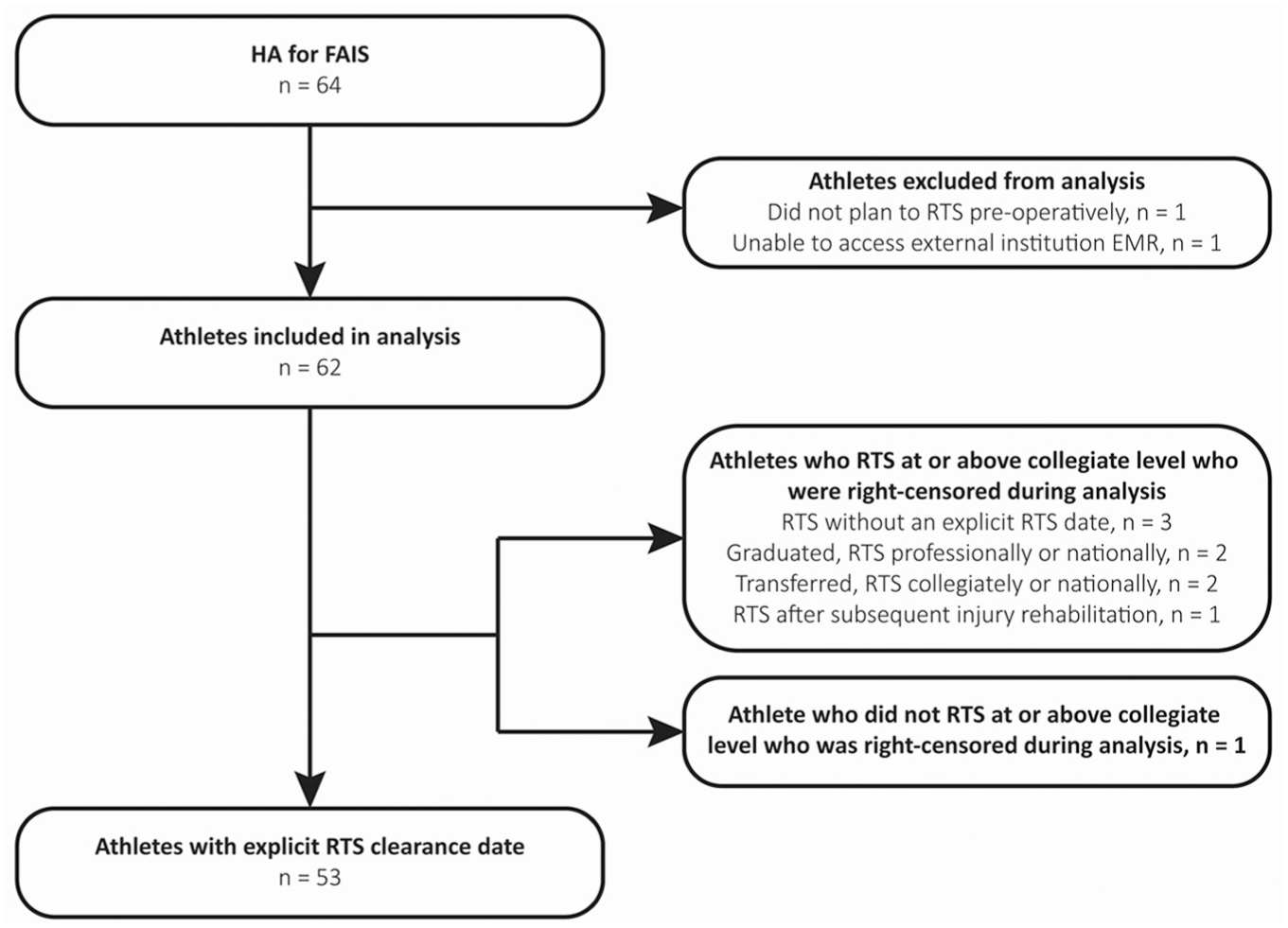
Electronic medical record (EMR) extraction process of athletes who underwent hip arthroscopy (HA) for the treatment of femoroacetabular impingement syndrome (FAIS). All but 1 athlete returned to sport at the University of Wisconsin–Madison or another institution at a collegiate, national, or professional level. RTS, return to sport.
Athlete-Specific Factors a

Data are presented as mean ± SD or number (%) unless otherwise indicated.
Based on total procedures with known information.
Chondral injury grading based on the Modified Outerbridge Classification System: grade 0 = normal cartilage; grade 1 = softening and swelling; grade 2 = partial-thickness defect, diameter <1.5 cm; grade 2a (wave sign) = cartilage delamination; grade 3 = defect to the level of subchondral bone, diameter >1.5 cm; grade 4 = exposed subchondral bone.
Sport
Sports with a minimum of 3 athletes included football, rowing, soccer, wrestling, track, and volleyball (Table 1). Overall, there were significant differences in time to RTS clearance among the different sports (P = .002). Specifically, athletes in track (3.4 [3.2-4.2] months) and wrestling (3.8 [3.2-3.9] months) required less time to RTS clearance than athletes in football (4.9 [4.4-5.4] months; P = .003 and P = .04, respectively; Figure 2). While not statistically significant, athletes in track and wrestling tended to be cleared to RTS sooner than those in soccer (4.6 [4.4-5.7] months; P = .05 and P = .06, respectively). Appendix Figure A1 provides a visual representation of median and IQR of time to RTS clearance among sports with a minimum of 3 athletes.

Kaplan-Meier curve displaying the proportion of athletes who have not yet been cleared to return to sport (RTS) over time following hip arthroscopy for femoroacetabular impingement syndrome, separated by sport. To be included within the analysis, a sport was required to have a minimum of 3 athletes. Tick marks indicate censored observations.
Sex
No difference was identified between female (4.2 [3.5-5.6] months) and male (4.8 [3.6-5.5] months) athletes regarding time to RTS clearance (Figure 3 and Table 2: HR = 0.91; 95% CI, 0.51-1.61; P = .74).
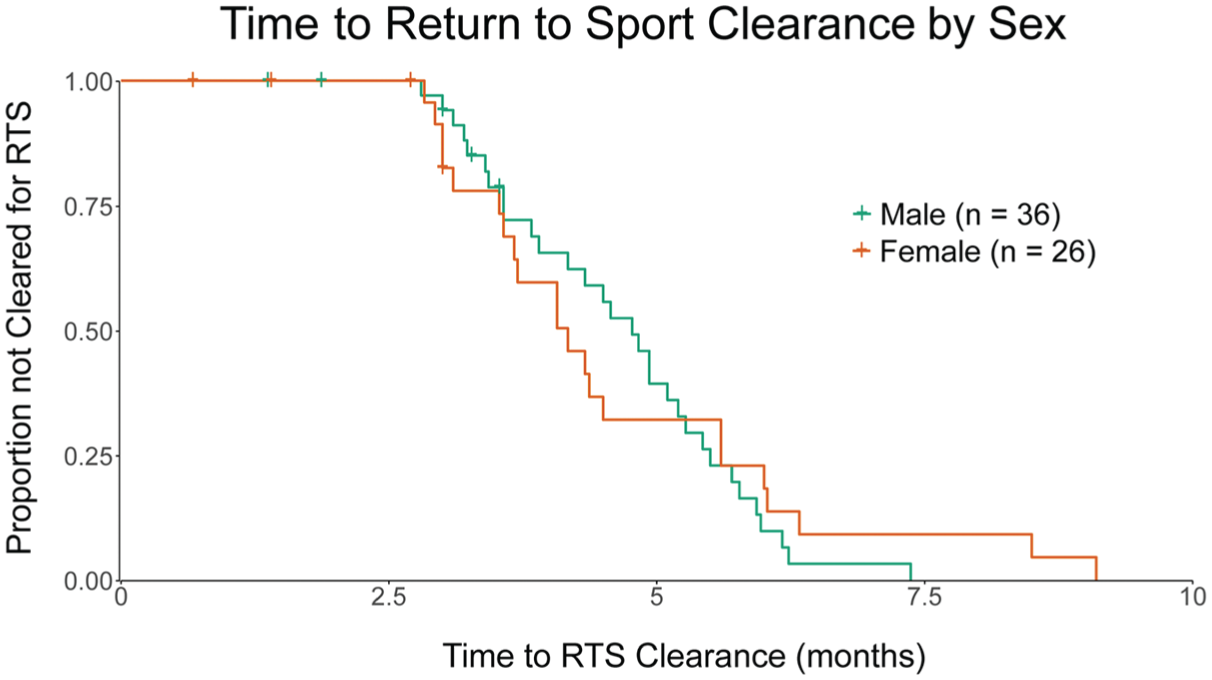
Kaplan-Meier curve displaying the proportion of athletes who have not yet been cleared to return to sport (RTS) over time following hip arthroscopy for femoroacetabular impingement syndrome, separated by sex. Tick marks indicate censored observations.
Univariable Time to Event Analyses for Potential Factors Affecting Time to Return-to-Sport Clearance a

The Cox proportional hazards models accounted for censored data. HR, hazard ratio; LCEA, lateral center-edge angle.
If surgery occurred during the competitive sport season (in-season) or not (off-season).
Based on the duration of time (months) from the date of surgery until the beginning of the next competitive season.
Based on procedures with known information from the unilateral surgery or the second surgery if bilateral.
A global P value is reported from the log-rank test. As differences between levels were nonsignificant, hazard ratios for each level are not reported.
Clinical and Surgical Factors: Demographic Characteristics, Preoperative and Intraoperative Findings, and Surgical Procedure Details
No clinical or surgical factors were found to significantly impact time to RTS clearance based on univariable analyses (Table 2: all P values >.05). As such, a multivariable analysis was not performed.
Discussion
This study aimed to identify how time to RTS clearance varies by sport and sex in collegiate athletes following hip arthroscopy for FAIS. In addition, we sought to determine if time to RTS clearance was impacted by any clinical or surgical factors, including demographics or preoperative, intraoperative, or surgery-related findings. The primary findings of this study are that (1) collegiate track and wrestling athletes undergoing hip arthroscopy for FAIS were cleared for RTS more quickly compared to football athletes, and (2) there was not a statistically significant difference in time to RTS clearance between female and male athletes. Additionally, no factors within athlete demographics, preoperative clinical findings, intraoperative findings, or surgical procedure details were found to significantly affect time to RTS clearance.
Our findings identified that track athletes were cleared for RTS quicker than football athletes, partially supporting our hypothesis that sports involving cutting, pivoting, or deep angles of hip flexion may require a longer time to RTS clearance. However, this hypothesis was not fully supported because athletes in wrestling, which requires repetitive positions of deep hip flexion, were also cleared for RTS quicker than football athletes and were cleared for RTS just as quickly as track athletes. Additionally, there were no significant differences between athletes in soccer, rowing, or volleyball in time to RTS clearance when compared to all other sports. With the time to RTS clearance being similar among nearly all sports within this analysis, a lack of difference may be due to the standardization of the postoperative recovery protocol for all athletes. Based on this rehabilitation protocol, 3.5 to 4 months is the quickest time to RTS if there are no postoperative complications (eg, persistent postoperative hip pain). This is supported by the overall median time to RTS clearance of 4.4 [3.5-5.5] months observed in this study. However, with track and wrestling athletes having a quicker time to RTS clearance than football athletes, other factors not considered in this study may influence the time required to RTS clearance between sports, such as psychosocial factors. Specifically, athletes in individual sports have been found to score significantly higher on conscientiousness (eg, achievement striving, self-discipline) and autonomy measures than athletes in team sports.27,34 This may contribute to a greater self-reliance and intrinsic motivation during postoperative rehabilitation, potentially resulting in a quicker time to RTS. However, the impact of specific psychosocial factors cannot be characterized within the scope of this study.
Overall, the average time to RTS clearance observed in this study was quicker than prior reports.4,10,20 In a cohort of young, competitive soccer players, a mean time to RTS of 7.62 ± 6.05 months was noted, 20 which is longer than our finding of 4.6 [4.4-5.7] months to RTS clearance for soccer athletes. Additionally, athletes in our study who compete in contact sports (eg, football, 4.9 [4.4-5.4] months; wrestling, 3.8 [3.2-3.9] months) were cleared for RTS more quickly than previous findings of 6.4 ± 0.4 months. 4 Contrary to our study, prior literature did not report any statistically significant differences in time to RTS between clusters of sport type 4 or specific sports. 10 Of note, our study specifically examined time to medical clearance for unrestricted sport participation, rather than return to competition, which may partially explain the shorter RTS time frames observed compared to prior reports.
The differences identified between prior literature and our findings may be attributed to using different methods to define the time to RTS.2,10,20 This study used a robust definition for RTS clearance by identifying an explicit statement of clearance for full activity/sport without restrictions by a member of the medical team. This ensures that the duration of time between surgery and RTS clearance is standardized among all athletes and is not confounded by extraneous time frames (ie, time to RTS self-reported as the number of weeks until the patient could play soccer with minimal pain after surgery 20 or reporting time missed from competition after surgery 2 ). Further work examining time to RTS should aim to use a standardized and explicit definition of RTS when reporting findings.
This study did not identify a difference in time to RTS clearance by sex (P = .74). Limited prior work has examined the impact of sex on time to RTS, as the predominant focus has been on the rate of returning to sport after hip arthroscopy. Notably, 1 study reported no difference in RTS timelines between elite female and male athletes, 38 matching our findings of no significant sex-based difference in time to RTS. In general, male athletes are more likely to have larger preoperative α angles, more mixed-type FAIS, less pincer-type FAIS, and more severe chondral defects compared to female athletes. 28 Additionally, male athletes are more likely to compete in contact sports, 28 while female athletes are more likely to compete in flexibility sports (eg, dance and gymnastics) 12 that may demand larger hip flexion angles and may be more challenging to return to after hip arthroscopy. Our study did not include any flexibility sports (eg, gymnastics, dance, cheer), which may partially explain why we saw no differences in time to RTS clearance by sex. Interestingly, the 2 athletes with the longest time to RTS clearance (8.5 and 9.1 months) were both female rowing athletes who had substantial difficulties managing anterior hip pain during postoperative recovery. Given that rowing involves repetitive, end-range hip flexion, it is unsurprising that these 2 athletes required a gradual progression back to sport. However, it should be noted that, as a collective team, the time to RTS clearance for rowing athletes did not differ significantly from other sports. While no differences in time to RTS clearance by sex were found in this study, sex-specific variations in pathological findings of FAIS and sport-specific demands on the hip are important considerations during the postoperative rehabilitation for each athlete.
While not a primary purpose of this study, the overall rate for RTS in this cohort was high (98%), with only 1 athlete not returning to sport. A recent meta-analysis identified that 87.9% (95% CI, 82.6%-92.3%) of athletes RTS after hip arthroscopy for FAIS, 40 with the predominant reason for discontinuing sport being persistent hip pain. This identifies a high overall success rate of hip arthroscopy for addressing symptomatic pathology, enabling athletes to return to competitive sport. Additionally, athletes who undergo bilateral surgery may be less likely to RTS than unilaterally operated patients, with 73% and 93% of collegiate athletes returning to sport, respectively. 28 However, within a cohort of elite soccer players, bilateral surgery was not a risk factor for failing to RTS. 20 When comparing male and female athletes, a recent systematic review found that female athletes had a 5.5% to 8.3% lower RTS rate compared to male athletes. 15 Given that nearly all athletes in this cohort returned to sport, we were unable to detect any differences in RTS rates based on the type of procedure (unilateral vs bilateral) or sex.
The lack of significance of time to RTS clearance based on clinical or surgical factors of demographics, preoperative findings, intraoperative findings, and surgical procedure details does not support our hypothesis that athletes with more severe findings would demonstrate a longer time to RTS clearance. These factors being nonsignificant may enhance patient expectations and provide guidance on directions for future work in this field. Specifically, the severity of hip joint pathology may not meaningfully affect recovery time frames after hip arthroscopy, as preoperative (eg, larger α angle) and intraoperative (eg, larger labral tear, higher-grade chondral injury) findings did not significantly affect time to RTS clearance. Additionally, the timing of surgery relative to the competitive season (in-season vs off-season) and the time until the start of the next competitive season did not influence time to RTS clearance. However, given that the spread of time to RTS clearance in this cohort was between 2.80 and 9.10 months, other factors not considered in this study may influence the time required for RTS clearance. Such factors to consider in future investigations include preoperative duration of hip pain,18,39 self-reported preoperative anxiety and depression, 35 persistence of pain postoperatively,17,40 recovery of hip and thigh muscular strength postoperatively,5,25 and sport-specific hip joint demands. 4
Limitations
While all athletes in this study were guided by UW Athletics rehabilitation staff postoperatively, variations within clinical practices were not controlled. As this study is a retrospective review of health care data, an a priori power analysis was not performed. We acknowledge that we may be underpowered to characterize the average time to RTS clearance within specific teams, given a small sample of athletes who underwent hip arthroscopy, which raises the possibility of type II error (ie, failing to detect a difference when a difference exists). Nevertheless, this is the most comprehensive analysis of time to RTS clearance by sport and sex in high-level athletes to date. Future work should aim to corroborate these findings in a larger sample. Additionally, 9 athletes were right-censored during the time-to-event analyses, as an explicit RTS clearance date could not be identified. We were unable to include preoperative symptom duration in our analysis. Although prior studies have shown that symptom duration can influence the likelihood and level of return to sport, this variable was inconsistently documented in our cohort and therefore could not be reliably incorporated into our time-to-event modeling. Future prospective studies should examine whether preoperative symptom duration also impacts the timeline for RTS clearance. Lastly, it is important to note that we used a strict RTS clearance definition based on a medical provider clearance for full, unrestricted participation in sport. As such, we are unable to make statements about athletes’ ability to return to their prior level of performance or their ability to successfully RTS long term. However, our results indicate that all athletes who returned to sport did so at the same or a higher (ie, national or professional) competitive level after surgery.
Conclusion
Collegiate athletes in wrestling and track who undergo hip arthroscopy for FAIS demonstrated quicker time to RTS clearance than those in football. There was no difference in time to RTS clearance between sexes. Despite variations in clinical and surgical factors, no variables within these categories significantly impacted time to RTS clearance.
Footnotes
Appendix
Acknowledgements
The authors thank Robert Hatch and Apoorva Dhawan for their assistance with data extraction from the electronic medical record system.
Final revision submitted November 19, 2025; accepted December 1, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This project was supported by the National Center for Advancing Translational Sciences, National Institutes of Health (grants TL1TR002375 [M.L.K.] and KL2TR002374 [K.A.K.] and by a Promotion of Doctoral Studies Scholarship from the Foundation for Physical Therapy Research (M.L.K.). A.M.S. is a consultant for Stryker Corporation. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Wisconsin–Madison Minimal Risk IRB (Health Sciences); submission ID number 2018-0049, dated February 17, 2020.