
Abstract
Background:
There are concerns that the Latarjet procedure for subcritical glenoid bone loss results in significant graft resorption and increased complications.
Purpose:
To (1) analyze the long-term results of the primary open Latarjet procedure in patients with subcritical preoperative glenoid bone loss and (2) find whether graft resorption influences these results.
Study Design:
Case series, Level of evidence, 4.
Methods:
A total of 50 shoulders (n = 48 patients) underwent the primary open Latarjet procedure at a mean age of 27 years (range, 19-37 years) for recurrent anterior shoulder instability with subcritical glenoid bone loss (<15%). After a mean of 8.5 years (range, 6-13 years), signs of recurrent instability, shoulder function, and patient-reported outcome measures—including the West Ontario Shoulder Instability Index (WOSI); the American Shoulder and Elbow Surgeon (ASES) score; the subjective shoulder value (SSV)—were assessed. Computed tomography-morphometric analysis of graft resorption was conducted to define the pattern and volume of resorption, and its influence on clinical outcomes.
Results:
At the final follow-up, a significant increase in the SSV (65% to 84%; P < .001), with a relative WOSI score of 19% ± 17% and an ASES score of 91 ± 9, was observed. One shoulder (2%) sustained a recurrent traumatic shoulder dislocation after 6.75 years but did not require revision surgery. Five shoulders (10%) experienced a subluxation, and 6 shoulders (12%) had positive anterior apprehension. Significant (P < .001) graft resorption (mean, 24% of the total graft volume) was observed at the long-term follow-up, although no patient underwent revision surgery. Resorption was concentrated in the superior segment of the graft (75%; P < .001). Overall, graft resorption had no significant influence on any clinical outcome measure—including complications, pain, or signs of postoperative instability (P > .05).
Conclusion:
The primary open Latarjet procedure for subcritical glenoid bone loss (<15%) results in an excellent clinical outcome. Although significant graft resorption (ie, concentrated around the superior screw) can be expected at the long-term follow-up, it does not result in adverse clinical outcomes, with complication and recurrence rates comparable to results of the Latarjet procedure for larger glenoid bone loss.
The Latarjet procedure—a well-established26,48 bone block procedure for the operative management of recurrent anterior shoulder instability—was first described 33 in 1957. The long-term clinical outcomes1,8,13,20,28 for the procedure are excellent, with studies suggesting that patients have improved shoulder function, reduced pain, and recurrence rates of <10%.
The Latarjet procedure has a number of procedure-specific complications related to the subscapularis muscle,6,14,16 graft malpositioning,13,15 -17,20,43 and graft resorption.11,49 Recent studies have focused on the effect of the Latarjet procedure on subscapularis muscle quality and graft mal-positioning,18,19 with relatively few studies investigating both resorption and clinical outcomes. Only moderate quality data are available; however, those focusing on graft resorption and clinical outcomes observed no association at the short-term follow-up.41,49
Despite the favorable long-term outcomes29,34,47 in most cases, there remains ongoing debate about the degree of “critical” glenoid bone loss, and its initial threshold of 20% to 25% has been revised32,39 to approximately 15%. With its growing popularity, certain centers have opted to utilize the Latarjet procedure for recurrent anterior shoulder instability with subcritical glenoid bone loss.12,22 The long-term clinical outcomes for patients with subcritical bone loss (<15%) are still unknown.
Therefore, the purpose of this study was 2fold. First, the study sought to assess the long-term clinical outcomes of the primary open Latarjet procedure for recurrent anterior shoulder instability in patients with subcritical glenoid bone loss (<15%). The secondary purpose of the study was to use a computed tomography (CT)-based morphometric technique to characterize the volume and pattern of graft resorption to determine the influence of long-term resorption on clinical outcomes. It was hypothesized that the Latarjet procedure in patients with subcritical glenoid bone loss is associated with excellent long-term recurrence rates and clinical outcomes; nonetheless, these results depend on the degree of postoperative graft resorption.
Methods
Ethical Approval
This retrospective case study was approved by the Cantonal Ethics Committee (No. 2018-01929). All patients gave written consent for this study.
Patients and Image Acquisition
From January 2008 to December 2013, a total of 80 consecutive patients (n = 82 shoulders) aged between 18 and 40 years were treated with a primary open Latarjet procedure for recurrent anterior shoulder instability with subcritical glenoid bone loss (ie, <15% of glenoid surface area). 39 Patients with (1) single screw graft fixation (as both screws were needed as key landmarks to localize the areas of bone loss); (2) hardware removal; (3) revision to shoulder arthroplasty; (4) medical conditions affecting shoulder function; or (5) those who refused follow-up CT scans (incomplete radiographic data) were excluded from this study. Moreover, patients living abroad were not invited for the follow-up, leaving 58 eligible patients (n = 60 shoulders) for this study.
At the final follow-up, 9 of the 58 patients were not available for a review in person, but they reported no complaints or revision surgery at the time of the telephone interview, and 1 person had died unrelated to the shoulder surgery. The reviewed cohort consisted of 48 patients (45 male and 3 female patients) and a total of 50 shoulders, with a mean age of 27 years (range, 19-37 years) at the time of the primary open Latarjet procedure (Figure 1).

A flow chart showing the identified shoulders (n = 82), eligible shoulders (n = 60), and the final cohort of shoulders for analysis (n = 50).
Patients were interviewed and examined at a mean follow-up of 8.5 years (range, 6-13 years) after surgery. Decision for a primary open Latarjet procedure in the presence of subcritical (ie, <15%) glenoid bone loss was based on a history of recurrent anterior shoulder instability and the fact that over the years at the treating shoulder center the recurrence rate with this procedure was significantly lower compared with soft tissue–based stabilization procedures. 50
All pre- and postoperative CT scans were obtained using a 64-slice Somatom Sensation 64 CT scanner (Siemens), with a slice thickness of 0.75 mm and a pitch of 0.8. Postoperative CT scans were obtained at the time of the interview and the examination at the final follow-up.
Surgical Technique
The surgical technique for the open Latarjet procedure was performed according to the Walch refinement of the original technique described by Latarjet.33,42 Through a deltopectoral approach, the coracoid was osteotomized at its base using bent chisels, and the glenoid neck was exposed through a horizontal split of the subscapularis muscle slightly below its mid-level. The harvested coracoid was slightly contoured to get a better fit against the glenoid neck. The graft was positioned flush with the glenoid plane at the 2- to 5-o’clock positions (in a right shoulder) and fixed with two 4.0-mm AO malleolar screws (Synthes). The coracoacromial ligament was sutured to the most medial aspect of the incised capsule. In all shoulders, the rotator cuff had a good quality without obvious pathology.
The shoulder was immobilized for 4 weeks in a sling, and biceps activation, combined abduction, and external rotation (ER) were restricted for 6 weeks. Patients could return to sports after 4 months.
Clinical Assessment
Postoperative clinical data were collected by 2 fellowship-trained orthopaedic surgeons (L.E. and M.W.). Clinical outcome parameters included evidence of anterior apprehension, subluxation, and recurrence of dislocation, work capacity, sports participation, complications, and reoperation. Clinical examination included assessment of range of motion (ROM) measurement, which was measured in degrees for abduction, flexion, and ER, and in points from 0 to 10 for internal rotation (IR) as per the Constant Score (CS). 7 The clinical examination also included assessment of the CS, 7 the Western Ontario Shoulder Instability index (WOSI), 31 the American Shoulder and Elbow Surgeons (ASES) score, and the subjective shoulder value (SSV). 23
Anterior apprehension was defined as a positive apprehension test, 50 and subluxation was defined as the subjective sensation of anterior translation of the humeral head over the glenoid rim, followed by spontaneous reduction. 3 Recurrence of dislocation was defined as any redislocation requiring reduction by the patient, a third party, or a medical professional. 50
CT Morphometric Analysis
CT measurement of graft volume (mm3) and resorption (%) was performed using a previously published technique with excellent reliability. 21 The patient’s preoperative scan and CT scan at the final follow-up were segmented to digitally reconstruct the 3-dimensional (3D) scapula geometry using computer software (Mimics; Materialise). The preoperative and final follow-up scapula geometries were registered (superimposed) to identify the site of coracoid osteotomy during the Latarjet procedure (Figure 2). Virtual osteotomy was performed using the computer software (Mimics; Materialise), and the coracoid was subsequently positioned onto the anterior glenoid of the preoperative scapula geometry. The inferior region of the graft on the final follow-up scapula was used as a reference point to position the coracoid graft, as this has been shown to undergo minimal resorption. 11 This process, therefore, created a third scapula geometry that modeled the surgically repaired shoulder, equivalent to an immediate postoperative scapula (ie, time point zero of graft morphology). The 3 scapula models were registered to help distinguish the native glenoid from the graft at the final follow-up, which was then digitally segmented separately from the scapula. The volume of the initial coracoid graft and the final follow-up graft was compared by measuring graft resorption (or deposition) over time.

Schematic diagram of the protocol used to segment the coracoid and the final follow-up graft. (A) CT registration of the preoperative and final follow-up scapula. (B) The coracoid graft is isolated, and its volume is recorded. (C) A virtual Latarjet procedure is performed to produce a third scapula geometry, the immediate postoperative scapula, which was registered with the postoperative scapula to distinguish the graft at the final follow-up. (D) The cutting planes are aligned for segment and subsegment analysis. CT, computed tomography.
To determine the regions where resorption was localized, the coracoid graft (time point zero of graft morphology) and the final follow-up graft were virtually segmented using the same digital software as described above. Planes that intersected the grafts in the sagittal, coronal, and axial planes were utilized to divide the graft into halves in all 3 planes, that is, into anterior and posterior halves, superior and inferior halves, and medial and lateral halves (Figure 3A). These half segments were further divided into 8 subsegments, with each an eighth of the original graft (Figure 3B). Comparison between the volumes of the corresponding segments and subsegments in the coracoid graft at time point zero and the final follow-up graft allowed for resorption in each segment and evaluation of each subsegment.
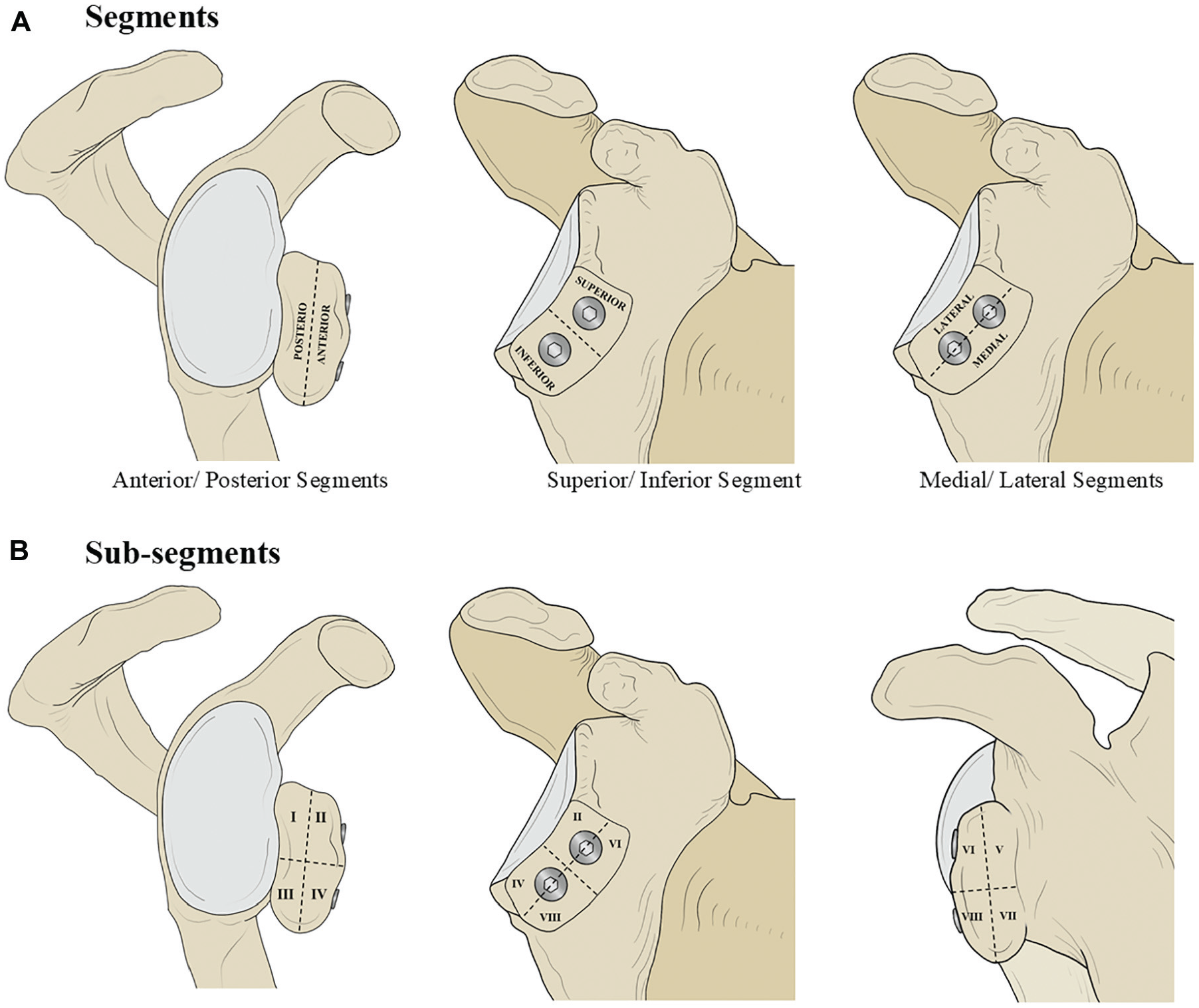
Illustration of the modelled immediate postoperative scapula, with the coaracoid graft positioned on the anterioglenoid rim. (A) The dashed lines show the planes in which the coracoid graft and the final follow-up graft were cut into segments and subsegments (1-8). (B) The volume of equivalent segments (ie, coracoid subsegment 2 and the final follow-up graft subsegment 2) was compared to determine the volume of graft resorption or bone deposition.
CT-scan assessment also included evaluation of graft positioning in the axial plane (ie, ≥1 mm lateral = proud; ≥4 mm medial = medially) and the sagittal plane (ie, <50% of the graft below equator = high).16,21
All CT scans were independently assessed by 2 readers, a fellowship-trained orthopaedic surgeon and a registrar (L.E. and F.F.P.), who were blinded to the clinical results.
Statistical Analysis
Based on a similar study on graft resorption after the open Latarjet procedure, 49 power analysis showed that for a significance level of .05 (type 1 error), a sample size of 50 shoulders is sufficient to provide a desired power of 80% to find a statistically significant difference in pre- and postoperative graft volume.
All data were assessed for normality using the Shapiro-Wilk test. Differences between pre-and postoperative data were analyzed using the paired t test (normal distribution) or the Wilcoxon signed-rank test (non-normal distribution). A 1-way analysis of variance (ANOVA) (for normally distributed data) and a Kruskal-Wallis ANOVA on ranks (for nonparametric data) were utilized to compare the differences between patient groups. The significance level was set at P < .05, and Bonferroni (1-way ANOVA) and Dunn-Bonferroni (Kruskal-Wallis ANOVA on ranks) corrections were applied. All t tests were 2-tailed.
Inter- and intraobserver reliability was assessed for the CT-morphometric volume measurements using the intraclass correlation coefficient (ICC) for absolute agreement, with 1 indicating perfect reliability.
Results
The dominant shoulder was affected in 27 cases (56%), and the mean age at first-time dislocation was 21.3 years (range, 14-34 years). The preoperative amount of glenoid bone loss in the en-face view was assessed by the Pico method on CT scans,17, 35 with a mean of 7% (range, 2%-14%). Five shoulders had preoperative mild (grade 1) glenohumeral osteoarthritis (OA) according to Samilson and Prieto, 38 which was also assessed in all included patients at the final follow-up. For analysis, patients were stratified by preoperative glenoid bone loss into 3 groups: the 0%-5% group, consisting of 15 shoulders; the >5%-10% group, consisting of 23 shoulders; and the >10%-<15% group, consisting of 12 shoulders.
Complications and Recurrent Instability
Four (8%) complications were recorded. At the final follow-up, 1 patient showed signs of mild postoperative frozen shoulder, which resolved after nonoperative management. Three patients reported irritation posterior of the shoulder. None of these 3 patients had radiographic signs of arthritis, and based on the available imaging data it was believed that the pain could have been associated with prominent screws. However, none opted for surgery. One patient (2%) had a traumatic redislocation that did not require revision surgery. Five patients (10%) reported episodes of subluxation, and 6 patients (12%) had a positive anterior apprehension at the final follow-up. No patients underwent revision surgery (Table 1).
Long-Term Complications, Reoperations, Apprehension, Subluxation, and Dislocations for the Patient Cohort at the Final Follow-up Stratified by Preoperative Glenoid Bone Loss a

Values are presented n (%). The significance level for between-group differences was set at P < .05. Preop, preoperative.
No significant differences were observed in the rates of complications, apprehension, subluxations, or dislocations between patients with different levels of preoperative glenoid bone loss (Table 1).
Clinical Outcomes
The mean CS% (P = .037) and its subcategories, and the SSV (P < .001) were significantly improved at the final follow-up (Table 2). Overall, the whole cohort had a significant mean increase of 2 points in CS pain (P < .001) at the final follow-up, with a mean pain score of 15 (no pain). In the Total Activity subcategory of the CS, the whole cohort demonstrated a significant increase in activity (P = .003). At the final follow-up, patients with 0% to 5% bone loss showed a mean increase of 24 SSV points (P < .001), those with 5% to 10% bone loss showed an increase of 15 points (P = .001), and those with 10% to 15% bone loss showed a significant increase of 21 SSV points (P = .017).
Clinical Scores for the Patient Cohort Preoperatively and at the Final Follow-up Stratified by Preoperative Glenoid Bone Loss a
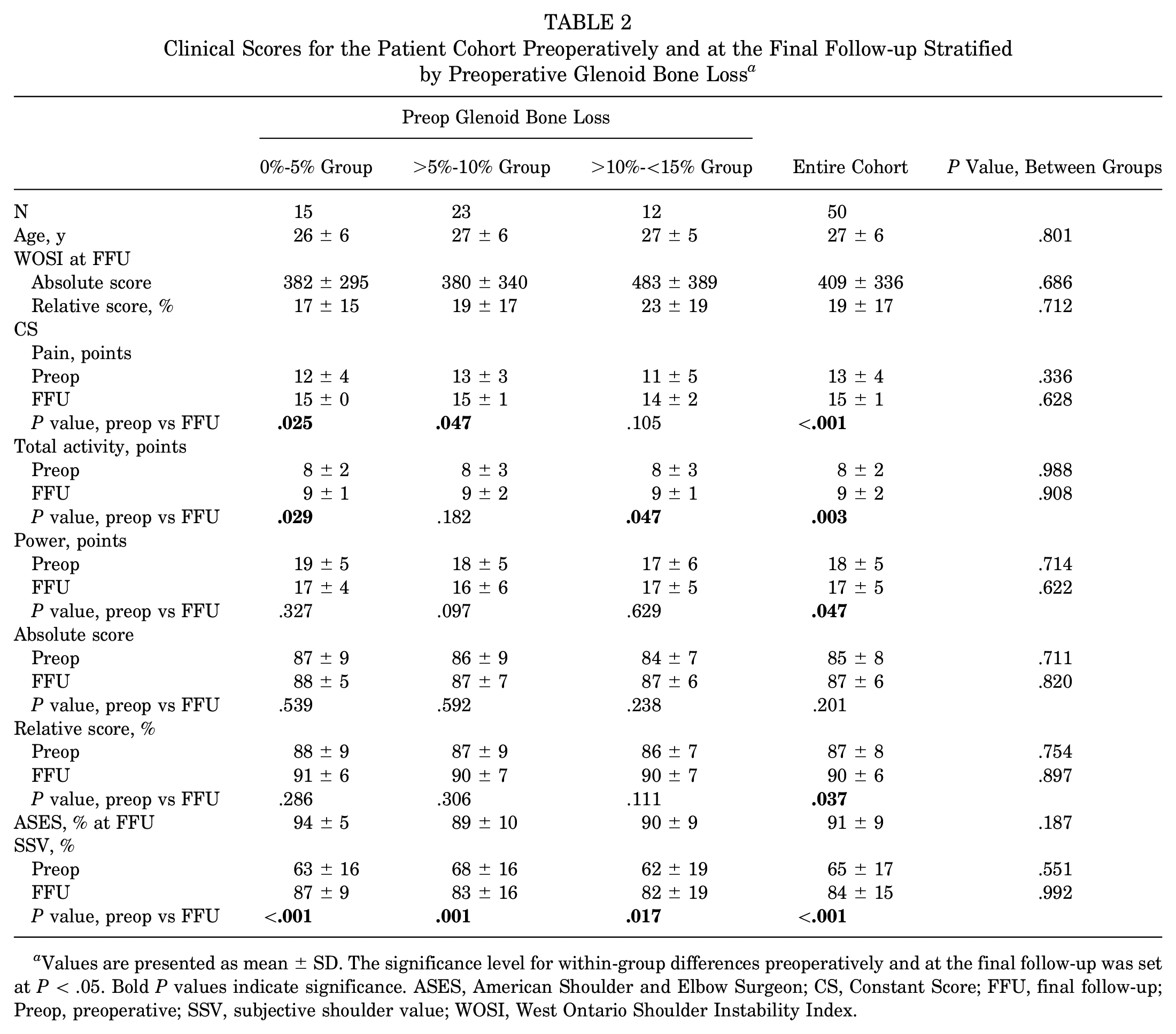
Values are presented as mean ± SD. The significance level for within-group differences preoperatively and at the final follow-up was set at P < .05. Bold P values indicate significance. ASES, American Shoulder and Elbow Surgeon; CS, Constant Score; FFU, final follow-up; Preop, preoperative; SSV, subjective shoulder value; WOSI, West Ontario Shoulder Instability Index.
For active ROM, across the entire cohort, a significant decrease in ER (13º; P < .001) and a significant increase in abduction (12º; P = .003) were observed at the final follow-up. For IR, a 1-point decrease (P = .017) was only observed in patients with >10% to <15% bone loss. For detailed information about ROM, see Appendix Table A1.
No significant differences were observed between the groups with different levels of preoperative glenoid bone loss (0%-5% vs >5%-10% vs >15% bone loss) for any of the clinical parameters measured at the final follow-up.
CT Morphometric Analysis
The mean graft resorption of all patients included was 686 mm,3 which was a significant loss of 24% of graft volume over the follow-up period (P < .001) (Table 3). When comparing graft resorption between different levels of preoperative glenoid bone loss, patients with 0% to 5% preoperative glenoid bone loss demonstrated the largest volume of graft resorption, losing 28% of the volume at the final follow-up (P = .002), while patients with >5% to 10% bone loss lost a mean of 26% (P < .001). Resorption in the >10%-<15% group was lower (14%) and did not reach statistical significance at the final follow-up (P = .067). No significant differences were observed in graft resorption between the different groups of preoperative glenoid bone loss at the final follow-up (P = .329).
Coracoid Graft Volume at Timepoint Zero, Final Follow-up Volume, and Graft Resorption for Shoulders (N = 50) Stratified by Preoperative Glenoid Bone Loss a

Negative graft resorption values indicate loss of bone volume at the final follow-up, while positive graft resorption values indicate net bone deposition. Bold P values indicate significance. The threshold for significant differences in graft volume at time point zero and at the final follow-up was set at P < .05. FFU, final follow-up; Preop, preoperative.
Overall, the maximum recorded graft resorption for a patient was 71%, while the maximum bone deposition recorded was an increase of 29% (Figure 4). A total of 37 shoulders (74%) showed net graft resorption at the final follow-up, while 13 shoulders (26%) showed net bone deposition. Of the patients with net bone deposition, 3 patients were in the 0%-5% preoperative bone loss group, 4 in the >5%-10% group, and 6 in the >10%-<15% bone loss group.
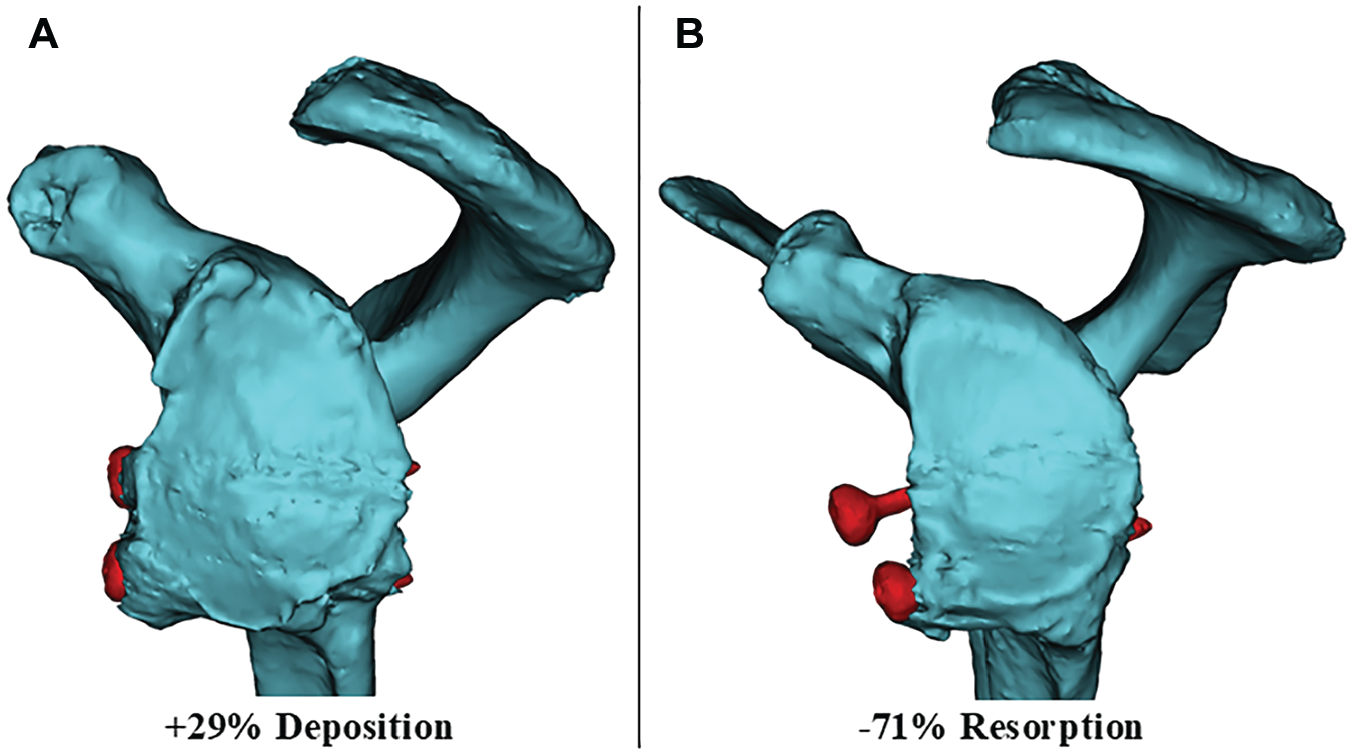
(A) Postoperative scapula geometries of 2 patients demonstrating bone deposition and (B) graft resorption. Screws are highlighted in red.
When the coracoid graft was divided into segments, significant graft resorption over time was observed in all segments (superior, anterior, posterior, medial, and lateral) except for the inferior segment (see Appendix Table A2). The superior segment showed the highest degree of resorption at the final follow-up (44%; P < .001), and the inferior segment showed the least/no resorption (1% deposition; P = .751).
The greatest subsegmental resorption was concentrated in the anterior-superior-medial (6) (75%; P < .001) and anterior-superior-lateral subsegments (2) (47%; P < .001). Subsegments posterior-inferior-medial (7) (23%; P < .001) and posterior-inferior-lateral (3) (8%; P = .148) showed significant bone deposition over the follow-up period (Table 4).
Coracoid Graft Volume at Time Point Zero, Final Follow-up Volume, and Graft Resorption for the 8 Graft Subsegments of the 50 Shoulders a

To calculate resorption, the volume of each segment at time point zero was compared with that at the final follow-up. Negative graft resorption values indicate loss of bone volume at the final follow-up, while positive graft resorption values indicate net bone deposition. Bold P values indicate significance. The threshold for significant differences in volume between segments at time point zero and the corresponding segment at the final follow-up was set at P < .05.
When comparing segment and subsegment resorption between different levels of preoperative glenoid bone loss, patients with >10% to <15% glenoid bone loss showed significantly less overall graft resorption (%) and significantly increased graft deposition compared with patients with 0% to 5% and >5% to 10% preoperative glenoid bone loss. In all of the posterior (P = .029), superior (P = .033), and lateral segments (P = .037), patients with >10% to <15% bone loss showed significantly less graft segment resorption than the other 2 groups. Patients with >10% to <15% glenoid bone loss also showed significantly less bone resorption in subsegment 1 (posterior-inferior-lateral) (P = .022). In subsegment 3 (posterior-inferior-lateral), patients with >10% to <15% preoperative bone loss showed significant bone deposition with an increase of 25% of graft volume, which was significantly higher (P = .039) than in patients with 0% to 5% (1% resorption) and >5% to 10% (6% deposition) preoperative glenoid bone loss. More detailed information can be found in Appendix Table A3.
About clinical outcomes, no association was observed between graft resorption or deposition on clinical outcome parameters (P > .05).
CT assessment of graft union showed full consolidation in all shoulders. A laterally overhanging position was noted in 15 shoulders (30%; 2 shoulders grade 1, 4 shoulders grade 2 radiographic OA) and a too medially positioned graft in 1 shoulder (2%). In the sagittal plane, 15 (30%) shoulders had the graft positioned above the equator. None of these parameters had a significant influence on graft resorption or deposition (P > .05).
CT-morphometric volume measurements showed excellent interrater (ICC, 0.930 [95% CI, 0.75-0.98]; P < .001) and intrarater reliability (ICC, 0.991 [95% CI, 0.963-0.998]; P < .001).
Discussion
The main findings of this study are that the primary open Latarjet procedure for recurrent anterior instability in patients with subcritical (0%-<15%) preoperative glenoid bone loss was effective at improving shoulder function and reducing pain; had high levels of subjective outcome; and was associated with a low recurrence and complication rate. It was also found that these clinical outcomes were not influenced by the volume of long-term graft resorption, albeit significant resorption was observed in most patients, which was mainly localized around the superior screw.
At all levels of preoperative bone loss and graft resorption, patients demonstrated significant improvements in clinical outcomes. These improvements occurred despite patients losing a mean of one-quarter of whole-graft volume by the final long-term follow-up. Graft resorption was found to be concentrated in the superior segment, particularly in the superoanterior region (ie, around superior screw head), with preservation of graft volume around the inferior segment, particularly in the inferior subsegments closer to the joint. Despite significant graft resorption across the patient cohort and at different levels of preoperative glenoid bone loss, this did not influence clinical outcomes or postoperative complications.
While the exact cutoff has been debated and revised, the open Latarjet procedure for recurrent anterior shoulder instability has been traditionally utilized in patients with glenoid bone loss of >15%. Long-term systematic reviews demonstrate that in this patient cohort, the procedure is effective, with excellent clinical and functional outcomes and a low complication rate. One systematic review with a 10-year follow-up period and 845 shoulders found a persistent apprehension rate of 9.9%, a dislocation rate of 3.2%, and a revision rate of 3.7%, with residual pain in 36% of the studied shoulders. Clinical scores 28 across the included studies were excellent, with a mean SSV of 89% and a CS of 83% at the final follow-up. In a more recent systematic review with a longer (15-year) follow-up period, these findings were reinforced. The study similarly found low complication rates, with persistent apprehension in 9.2% of the cohort, a dislocation rate of 3.4%, and a revision rate of 5.1%, with ongoing pain in 34% of the included shoulders. The study found that the open Latarjet procedure had good functional outcomes, with an SSV of 88% and a CS of 83% at the final follow-up. 8 The present study found an apprehension rate of 12%, compared with 9.9% and 9.2% in the systematic reviews, a dislocation rate of 2% compared with 3.2% and 3.4%, and a revision rate of 0% compared with 3.7% and 5.1%. The clinical scores were also consistent with an SSV score of 84% in the present study compared with 89% and 88%, and a CS of 90% in the present study compared with 83% in both systematic reviews. However, ongoing pain in the present study was less than that described in both reviews, with 20% of our cohort reporting ongoing postoperative pain compared with 36% and 33% in the systematic reviews. Thus, the present study suggests that the primary open Latarjet procedure in patients with subcritical glenoid bone loss (<15%) can, at worst, produce comparable results to the Latarjet procedure in patients with larger preoperative glenoid bone loss (>15%).
Another finding of the study is that patients undergoing the open Latarjet procedure in the setting of subcritical glenoid bone loss have minimal loss of active ROM of the shoulder postoperatively. Previous studies showed that ROM is mostly unchanged postoperatively, except for ER and IR, which consistently show minor reductions that are likely only clinically significant in overhead athletes.2,19,20,40 In a recent study by Sinha et al, 40 patients were shown to have statistically significant losses in ROM at 24 months after the Latarjet procedure, with a loss of 6° in abduction and flexion, 10° in ER, and 6° in IR. A further systematic review of the open Latarjet procedure similarly found a mean loss of 12° in ER. 2 In the present study, a significant reduction of active ER (13°) was observed, which is largely in keeping with the literature for patients with larger preoperative glenoid bone loss. On the other side, it was observed that active abduction increased by 12° at the final follow-up, although the authors do not have a plausible explanation for this increase in active abduction. Active IR was only significantly reduced in patients with >10% to <15% glenoid bone loss and not in those with no to <10% preoperative glenoid bone loss, despite the latter group of patients showing significantly more overall graft resorption than those with >10% to <15% glenoid bone loss. However, the significant reduction in active IR in the >10%-<15% group at the final follow-up was only 1 CS point, which appears to be clinically insignificant.
Graft resorption after the open Latarjet procedure has arisen as one of the complications of greatest clinical concern. It has been proposed that more severe graft resorption may predispose patients to increased recurrence rates, pain, and reduced subscapularis function.1,13,19,27 While the present study found that patients with >10% to <15% glenoid bone loss showed less resorption and increased bone deposition, this did not lead to improved clinical outcomes, nor did increased resorption in the other groups lead to worse clinical outcomes, specifically not worse IR, not an increased recurrence or complication rate, nor an increased need for hardware removal due to anterior shoulder pain, or jeopardizing the subscapularis. The observed results are in keeping with a study by Sahu et al, 37 which compared patients who underwent the Latarjet procedure with no preoperative glenoid loss to those with ≥15% bone loss, and found no significant differences in clinical outcomes (Rowe score, SSV, redislocation, and apprehension) at a minimum of 1 year follow-up (range 1-4 years). Zhu et al 49 did not stratify patients by preoperative glenoid bone loss, but they observed that different qualitative grades of resorption were not associated with worse clinical outcomes (ASES, CS, and Rowe score). Also, they found no significant difference in ROM between patients with minor and major resorption. Ting et al 41 in a cohort of median 15% preoperative bone loss, similarly found no difference in WOSI scores between patients who had minor and major graft resorption at a median of 44 months. The present study not only reinforces these findings but further demonstrates, for the first time, that the excellent clinical outcomes are maintained over a long-term follow-up period and that graft resorption is not a driving factor for failure of the Latarjet procedure.
The present study has also found that graft resorption is influenced by the degree of preoperative glenoid bone loss, with patients who had >10% to <15% preoperative bone loss demonstrating less graft resorption and increased bone deposition compared with patients with 0% to 5% and >5% to 10% glenoid bone loss. One might stipulate that this is attributed to increased mechanical loading of the graft from the humeral head with increasing preoperative glenoid bone loss. Recent computer-based biomechanical data 18 showed that the Latarjet procedure in larger glenoid bone loss models leads to a significant increase in graft contact pressure compared with models with subcritical glenoid bone loss, which may explain why there is likely less graft resorption with larger glenoid bone loss. This appears to be due to the graft’s relative “centralizing” in the case of large anteroinferior glenoid defects (ie, the graft moves closer to the center of the glenoid with larger bone defects) and the resulting load-sharing effect of the bone block. While resorption may be decreased, patients with larger defects are more susceptible to graft malpositioning and increased glenohumeral contact pressures. 18 In smaller or no bony defects, the graft is further anterior, and the excess bone on the periphery of the graft experiences less loading from the humeral head, resulting in resorption of mechanically unloaded bone according to the Wolff law. 45 This is supported by the fact that in the present study, increased resorption was observed in the anterior segment (further away from the joint) compared with the posterior segment (closer to the joint), which is consistent with observations made by Kee et al. 30
An alternative explanation for the patterns of resorption observed may be related to the disruption of the blood supply of the graft. In cadaveric studies investigating the blood supply to the coracoid process before and after Latarjet, it has been found that the native coracoid is nourished by 2 to 3 arteries (including variable supply from the conjoint tendon), and that these are sacrificed during coracoid process osteotomy.9,25 The decreased resorption in the inferior portion of the graft (distal coracoid) may be in part due to preservation of the arterial supply from the conjoint tendon, which remains intact during the procedure, while disruption to the proximal blood supply, where the coracoid is osteotomized, may provide an ischemic explanation for why resorption is increased in this region.
In light of the findings of the present study, the literature, and anticipation of prominent superior segment resorption, consideration could be given to adapting the Latarjet surgical technique to include a hybrid fixation technique. Di Giacomo et al 10 compared the standard Latarjet technique with a modified procedure involving 2 screws through a custom-made miniplate, and found that while posterior region resorption was significantly reduced with the miniplate, resorption was still concentrated in anterior and superior regions of the graft for both techniques. Boileau et al 4 have also developed an alternative to the traditional Latarjet surgery, proposing an arthroscopic suture button technique instead of fixation with screws. This approach is safe and effective at stabilizing the shoulder, although a recent systematic review 36 suggests that it has a higher rate of postoperative recurrent instability than a 2-screw construct. Nevertheless, several studies have shown that a suture button approach results in less graft resorption and has fewer complications than a screw-based construct, such as prominent metalware.5,24,44,46 The present study, however, highlights that resorption is predominately localized in the superior segment (screw). As such, the authors suggest that a hybrid fixation technique using an inferior screw and a superior suture suspension fixation could be used to reduce superior graft resorption in the long-term. This overcomes the limitations of a 2-screw construct and, at the same time, avoids the doubts about primary stability in all-suture fixation techniques.
The following limitations ought to be acknowledged. A limitation of the present study is that the use of image registration to determine where the coracoid was osteotomized during surgery was used, and does not account for minor macroscopic remodeling that may be done during surgery to increase congruency with the anterior glenoid, and may lead to small reductions in volume. However, the current image registration technique was proven to be highly correlated with the 2D gold standard technique by Zhu et al, 49 and was also found to have excellent inter- and intrarater reliability with the obvious advantages of 3D assessment of graft resorption. 21 This limitation could also be addressed with early postoperative CT scans to obtain the exact volume of the transplanted graft. However, this is costly and exposes patients to unnecessary ionizing radiation. The current technique represents a noninvasive method of measuring immediate postoperative graft volume, at the cost of what is likely a minor and clinically insignificant inaccuracy in immediate postoperative graft volume. Another limitation is that there may be variations associated with graft positioning during the virtual Latarjet procedure to produce the modeled immediate postoperative scapula. The inferior region of the graft at the final follow-up was used to position the coracoid graft during the virtual Latarjet procedure, as this has been previously characterized as undergoing minimal to no resorption. Furthermore, there may be variations in the positioning of the cutting planes used to divide the grafts for regional, segmental analysis. The glenoid has 3 distinct anatomic shapes, and when coupled with normal variation in graft positioning during surgery, the position of the cutting planes could not be rigidly standardized between patients. To overcome this, the planes were oriented so that 50% of the immediate postoperative graft was on either side of the cutting plane. Another limitation is that the study did not include a soft-tissue procedure for comparison with clinical outcomes, which is relevant considering that patients had only subcritical preoperative glenoid bone loss. Finally, the study did not collect clinical data related to return to sports.
Conclusion
The primary open Latarjet procedure for subcritical glenoid bone loss (<15%) results in an excellent clinical outcome. Although significant graft resorption (ie, concentrated around the superior screw) can be expected at the long-term follow-up, it does not result in adverse clinical outcomes, with complication and recurrence rates comparable to results of the Latarjet procedure for larger glenoid bone loss.
Footnotes
Appendix
Mean Whole Graft, Segment, and Subsegment Resorption Stratified by Preoperative Glenoid Bone Loss a

| Preop Glenoid Bone Loss | Entire Cohort | P Value, Between Groups | |||
|---|---|---|---|---|---|
| 0%-5% | >5%-10% | >10%-<15% | |||
| N | 15 | 23 | 12 | 50 | |
| Resorption, % | |||||
| Whole graft resorption | –28 ± 21 | –26 ± 21 | –14 ± 20 | -24 ± 21 | .329 |
| Anterior | –44 ± 29 | –41 ± 22 | –31 ± 23 | –40 ± 24 | .612 |
| Posterior | –15 ± 22 | –13 ± 24 | 2 ± 26 | –10 ± 24 |
|
| Superior | –48 ± 24 | –48 ± 21 | –31 ± 28 | –44 ± 24 |
|
| Inferior | –2 ± 26 | 1 ± 28 | 9 ± 24 | 1 ± 27 | .647 |
| Medial | –32 ± 22 | –30 ± 21 | –23 ± 19 | –29 ± 21 | .527 |
| Lateral | –22 ± 26 | –22 ± 23 | –4 ± 23 | –18 ± 24 |
|
| 1. Posterior-superior-lateral | –26 ± 35 | –27 ± 30 | –8 ± 33 | –22 ± 32 |
|
| 2. Anterior-superior-lateral | –47 ± 35 | –56 ± 29 | –32 ± 28 | –47 ± 31 | .441 |
| 3. Posterior-inferior-lateral | –1 ± 29 | 6 ± 35 | 25 ± 44 | 8 ± 36 |
|
| 4. Anterior-inferior-lateral | –3 ± 40 | –6 ± 36 | 7 ± 30 | 3 ± 37 | .682 |
| 5. Posterior-superior-medial | –42 ± 26 | –43 ± 25 | –32 ± 39 | –40 ± 29 | .418 |
| 6. Anterior-superior-medial | –78 ± 25 | –77 ± 21 | –67 ± 28 | –75 ± 24 | .209 |
| 7. Posterior-inferior-medial | 16 ± 31 | 23 ± 37 | 35 ± 16 | 23 ± 35 | .598 |
| 8. Anterior-inferior-medial | –27 ± 37 | –17 ± 37 | –14 ± 31 | –19 ± 35 | .899 |
Data are presented as mean ± SD unless otherwise indicated. Bold P values indicate significance. The threshold for significant between-group differences in resorption was set at P < .05. Negative graft resorption values indicate loss of bone volume at final follow-up, while positive values indicate net bone deposition; Preop, preoperative.
Acknowledgements
Imaging was performed with the support of the Swiss Center for Musculoskeletal Imaging (SCMI) at the Balgrist Campus of the University of Zürich, Zürich, Switzerland.
The authors would like to acknowledge Ms Bree McAleer for preparing the scapula illustrations contained in Figures 2 and 3.
Final revision submitted March 11, 2025; accepted March 28, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: Financial support was provided by the AGA-Gesellschaft für Arthroskopie und Gelenkchirurgie (grant No. 78). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Cantonal Ethics Committee (No. 2018-01929).