
Abstract
Background:
Cyclops syndrome is a complication of anterior cruciate ligament (ACL) reconstruction (ACLR). Its recurrence (recyclops) after surgical treatment is poorly understood, with limited research on risk factors and characteristics.
Purpose/Hypothesis:
The purpose of this study is to determine the recurrence rate of cyclops syndrome after previous surgery and identify associated risk factors. It was hypothesized that the recyclops rate is significant and is associated with certain modifiable and nonmodifiable risk factors.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This study included all patients who underwent knee arthrolysis for cyclops syndrome after ACLR at a sports surgery center between 2005 and 2022. The primary outcome was the rate of recurrent cyclops syndrome and its associated risk factors. Secondary outcomes included knee range of motion, measured using a goniometer, both preoperatively and 6 weeks postoperatively, with comparisons made between patients with primary and recurrent cyclops cases.
Results:
During the study timeframe, 12,200 primary ACLRs were performed, from which a total of 359 patients with cyclops syndrome were found (2.9%), with a mean age of 25.34 ± 6.12 years and a male predominance of 57.38%. The recyclops rate was 6.9% (25 out of 359 patients). Risk factors identified in multivariate analysis were as follows: (1) age (patients >27 years, odds ratio [OR], 11.63 [95% CI, 3.41-39.73]; P < .001); (2) type of graft (quadrupled semitendinosus graft: OR, 5.09 [95% CI, 1.05-24.74]; P = .044); (3) bone-patellar tendon-bone grafts (OR, 26.01 [95% CI, 6.52-103.82]; P < .001); (4) absence of lateral extra-articular procedure (LEAP) (OR, 8.49 [95% CI, 1.64-43.97]; P = .011); and (5) time from ACL surgery to initial cyclops surgery of <7 months (OR, 13.62 [95% CI, 4.07-45.66]; P < .001). At 6 weeks postoperatively, the mean residual extension deficit, after initial arthrolysis, was significantly higher in the relapse group than in the no relapse group, with a median of 5° compared with 0° in the no relapse group (P < .001).
Conclusion:
Recyclops syndrome occurred in 6.9% of patients after cyclops arthrolysis. Significant risk factors include age, type of graft, absence of LEAP, and shorter time from ACL surgery to initial cyclops surgery. Among patients who underwent operation for the first time for cyclops, those who had residual extension deficit at 6 weeks postoperatively were more likely to experience recyclops.
Reconstruction of the anterior cruciate ligament (ACL) is a frequent and reproducible procedure with excellent long-term results.2,13 One of the main complications of this procedure is an extension deficit caused by the presence of a fibrous nodule in the intercondylar notch or at the tibial attachment/tunnel of the ACL graft.10,15,26 This condition is known as cyclops syndrome. The fibrous nodule corresponds to fibrovascular tissue with overlying blood vessels, which arthroscopically resembles the eye of a “cyclops.” Histological analysis typically reveals chronic inflammation with multinucleated giant cells, similar to a foreign body reaction.10,15,26
This condition is relatively rare, complicating only 2% to 10% of ACL reconstruction (ACLR).15,17,26 When symptomatic, the diagnosis is made in approximately 93% of cases within 6 months after surgery. Clinically, it manifests as a loss of terminal knee extension, sometimes accompanied by an audible or palpable clunk. 17 Patients may also experience discomfort while walking or running, along with poorer functional outcomes.15,17,26 Magnetic resonance imaging (MRI) aids in diagnosing cyclops syndrome. 26
Several literature reviews have sought to identify the risk factors associated with the occurrence of cyclops syndrome.11,16,17 Previous studies have found that age, graft type, and lateral extra-articular procedures (LEAP) are not associated with an increased risk of cyclops syndrome.1,8,20,21,23,26 However, other factors, such as female sex, a narrow notch, an excessively anterior position of the tibial tunnel, or simultaneous repair of a meniscal lesion, remain debated as potential risk factors.1,3,8,20,21,23,26 The only widely accepted risk factor is the early postoperative presence of an active extension deficit accompanied by a loss of quadriceps tone.3,8,21
While the management of cyclops syndrome through early arthroscopic arthrolysis provides satisfactory clinical results, only a few articles describe the recurrence of cyclops syndrome, either on imaging or clinically, primarily in the form of case reports or small case series.6,7,11,12,16,24 To date, no study has identified risk factors for recurrence.
The primary objective of this study was to determine the recurrence rate of recurrent cyclops syndrome before surgery and identify associated risk factors. The secondary objective was to compare postoperative knee mobility between primary and revision cyclops cases. We hypothesized that recurrent cyclops syndrome accounts for a significant proportion of persistent extension deficits in patients previously treated for cyclops syndrome after ACLR and that its occurrence is associated with specific modifiable and nonmodifiable risk factors.
Methods
Study Design and Inclusions
This retrospective cohort study included all patients who underwent knee arthrolysis after ACLR between 2005 and 2022 at a sports surgery center in Paris. Patients were included retrospectively if their medical records contained a diagnosis of cyclops syndrome. Patients who underwent open arthrolysis or arthroscopic arthrolysis for other conditions (eg, postpatellar tendon repair stiffness, villonodular synovitis, or tibial eminence reinsertion) were excluded. The study adhered to the Declaration of Helsinki and complied with French regulatory methodology MR-004 for health-related research. Patients were informed about the study’s objectives and could opt out of participation. Written informed consent was obtained, and for deceased patients, their written objection during their lifetime was honored.
Definition of Cyclops and Recurrent Cyclops Syndrome
Cyclops syndrome was defined as a postoperative clinical extension deficit after ACLR, characterized by MRI evidence of a fibrous nodule located in the roof of the notch or at the ACL tibial attachments/tunnel (Figure 1), requiring arthroscopic arthrolysis for treatment. Recurrent cyclops syndrome was defined as the recurrence of cyclops syndrome after a previous arthroscopic arthrolysis.

MRI series showing cyclops at 6 months postoperatively (to the left) and recurrent cyclops syndrome at 9 months after arthrolysis (to the right) in the same patient. (A) Frontal T2-weighted MRI showing a primary cyclops formation. (B) Frontal T2-weighted MRI showing a recurrent cyclops formation. (C) Sagittal T2-weighted MRI showing a primary cyclops formation. (D) Sagittal T2-weighted MRI showing a recurrent cyclops formation. (E) Axial T2-weighted MRI showing a primary cyclops formation. (F) Axial T2-weighted MRI showing a recurrent cyclops formation. MRI, magnetic resonance imaging.
Surgical Techniques
All surgeries were conducted by 6 senior surgeons (N.L., A.M., Y.B., A.G., O.G., A.H.) specialized in sports surgery. The surgical treatment for cyclops syndrome involves arthroscopic excision of the fibrous nodule located in the roof of the notch or at the ACL attachment/tunnel site. Additional arthrolysis and lysis of adhesions were performed to achieve full extension intraoperatively. No notchplasty was performed at the time of the initial arthrolysis. However, in recurrent cyclops cases, a notchplasty was performed at the time of revision surgery. Initial ACLR techniques varied and included quadrupled hamstring grafts, quadrupled semitendinosus (ST4), or doubled gracilis and semitendinosus, bone-patellar tendon-bone (BPTB) grafts, and combined extra- and intra-articular reconstruction using the modified Macintosh procedure (McFL). 5 Except for the McFL, additional LEAPs were performed selectively in cases with high-grade rotational instability on pivot testing, as well as for high-level athletes requiring enhanced rotational control.
Autografts were used for all reconstructions in this study.
Outcome Measures
The primary outcome was the recurrence rate of recurrent cyclops syndrome, defined as the recurrence of clinical and radiological cyclops syndrome with an extension deficit and fibrous nodule in the notch, necessitating repeat arthroscopic arthrolysis. The study also analyzed risk factors associated with recurrent cyclops formation, such as age, sex, graft type, associated procedures (eg, meniscal suture, meniscectomy, or LEAP), time from ACL surgery to cyclops treatment, and postoperative complications such as hematoma.
Secondary outcomes included pre- and postoperative knee range of motion. This was measured in the outpatient clinic using a standard goniometer. All measurements were taken with the patient in a supine position to eliminate variability associated with sitting or standing postures and stabilize the pelvis and hip during testing. The 0° was defined as a straight line.
Data Collection
All data were collected prospectively based on the clinic’s computerized database using Websurvey software. Other data sources included standardized consultation reports containing clinical examination data (range of motion, any complications), and operative reports.
The following data were collected: (1) age at the time of cyclops syndrome; (2) type of graft used during ACLR; (3) presence of an associated procedure during the ACLR (meniscal suture, meniscectomy, LEAP); (4) occurrence of postoperative complications; (5) pre- and postoperative mobility (range of motion, including extension deficit and flexion); and (6) time to surgical management of cyclops syndrome.
Statistical Analysis
Descriptive statistics were calculated, including frequencies and percentages for categorical variables. For continuous variables, the mean and standard deviation were reported. Comparisons between the 2 groups (patients with no relapse vs patients with relapse) were made using either the Student t test or the Wilcoxon rank-sum test for continuous variables and the chi-square test or the Fisher exact test for categorical variables, depending on the sample size.
Risk factors were analyzed using logistic regression to estimate the odds ratios (ORs) and 95% CIs associated with the outcome of interest. Before fitting the multivariate model, potential confounding variables were identified using univariate regression analyses. Variables with a significant association with the outcome at P < .10 were included in the multivariate regression model. A backward stepwise method was used to eliminate nonsignificant variables from the model, with a threshold of P < .05 for retention in the model.
Continuous variables significantly associated with the outcome were also transformed and analyzed as categorical variables using the receiver operating characteristic (ROC) curve. For example, age was transformed into a categorical variable based on the optimal threshold determined by the ROC curve. The ROC curve and the Youden index were used to determine the optimal threshold for the time between the first ACL surgery and cyclops surgery in relation to the primary outcome, recyclops formation.
Statistical analyses were performed using Datatab software (Version 2024) with a 2-tailed significance level of P < .05.
Results
Characteristics
During the study timeframe, 12,200 ACLR surgeries were performed, from which 359 patients with cyclops syndrome were found (2.9%). The mean age of the population was 25.34 ± 6.12 years, with a male predominance of 57.38%. Most grafts were G2ST2 (75.49%). Patients’ characteristics are presented in Table 1.
Demographic Characteristics a

Data are presented as n (%) or mean ± SD. ACL, anterior cruciate ligament; BPTB, bone-patellar tendon-bone; G2ST2, doubled gracilis and semitendinosus; grafts; LEAP, lateral extra-articular procedure; McFL, combined extra- and intra-articular reconstruction using the modified Macintosh procedure; ST4, quadrupled semitendinosus.
Rate of Recurrent Cyclops Syndrome
The recyclops formation rate was 6.9% (25 out of 359 patients). Among those who experienced a relapse, only 1 patient (4%) experienced another relapse.
Patients with recurrent cyclops syndrome were significantly older (mean age, 30.6 ± 8.45 years vs 24.94 ± 5.73 years; P = .003) and had a shorter time from ACL surgery to cyclops surgery (8.6 ± 7.28 months vs 14.51 ± 18.05 months; P = .001). The type of graft used was also significant, with a higher proportion of BPTB (12 patients; 48%) and ST4 (4 patients; 16%) grafts in the relapse group compared with the no relapse group (BPTB: 26 patients; 7.78%; ST4: 43 patients; 12.87%) (P < .001). LEAPs were less common in the relapse group (2 patients; 8%) compared with the no relapse group (108 patients; 32.33%) (P = .011).
ROC Curve Cutoffs Before Risk Factors Analysis
The ROC curve analysis for age versus recurrent cyclops formation showed an optimal cutoff age of 27 years (area under the curve [AUC], 0.73; Youden index, 0.439), indicating a moderate ability to distinguish between patients with and without recurrent cyclops (Figure 2A). For the time between the first ACL surgery and cyclops surgery versus recurrent cyclops surgery, the ROC curve showed an optimal time of >7 months (AUC, 0.723; Youden index, 0.451) (Figure 2B).
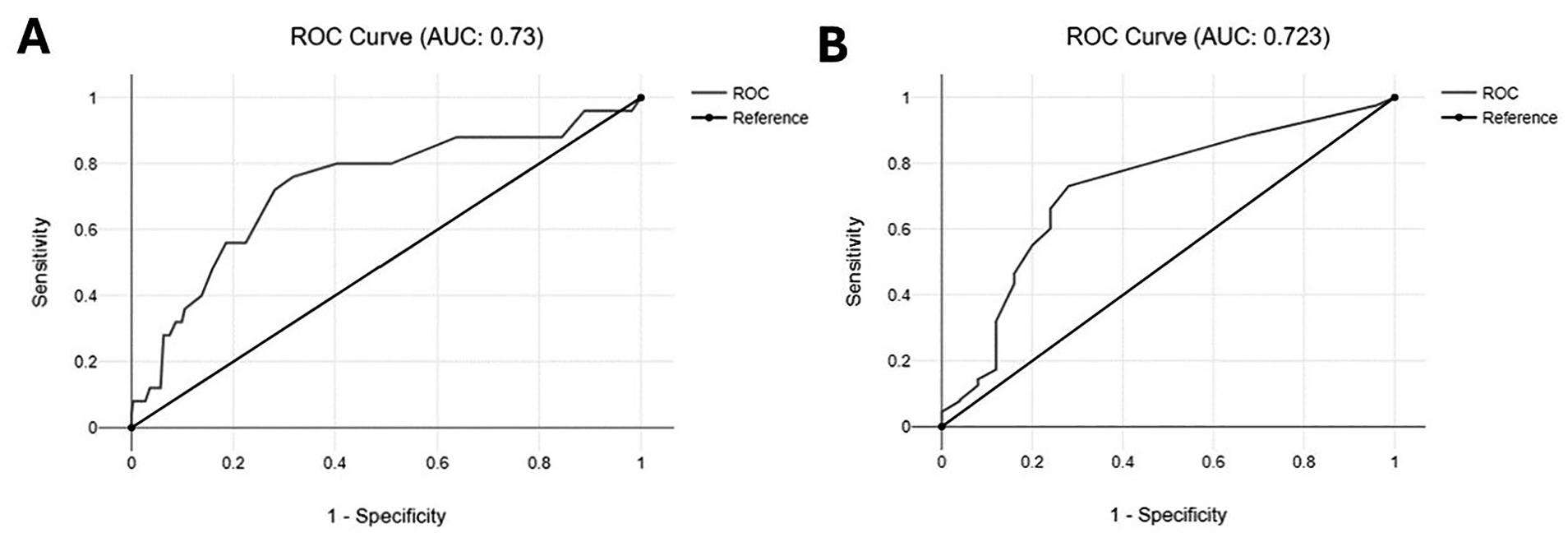
(A) ROC curve analysis of age versus recurrent cyclops syndrome: Youden index, 0.439; optimal cutoff, 27 years old. (B) ROC curve time versus recurrent cyclops syndrome: AUC, 0.277; Youden index, 0.451; optimal time, >7 months. AUC, area under the curve; ROC, receiver operating characteristic.
Risk Factors Analysis
In the univariate analysis, age, type of graft, the use of LEAP, having early hematoma complications, and the time from ACL surgery to the initial arthrolysis were identified as potential risk factors and were thus included in the multivariate model (Table 2).
Risk Factors of Recurrent Cyclops Syndrome a

Bold P values indicate statistical significance. ACL, anterior cruciate ligament; BPTB, bone-patellar tendon-bone grafts; G2ST2, doubled gracilis and semitendinosus; McFL, combined extra- and intra-articular reconstruction using the modified Macintosh procedure; LEAP, lateral extra-articular procedure; OR, odds ratio; Ref, reference; ROC, receiver operating characteristic; ST4: quadrupled semitendinosus.
In the multivariate analysis, age remained a significant factor. Patients >27 years had an OR of 11.63 (95% CI, 3.41-39.73; P < .001) compared with younger patients. The type of graft also continued to show significant associations: ST4 grafts had an OR of 5.09 (95% CI, 1.05-24.74; P = .044), and BPTB grafts had an OR of 26.01 (95% CI, 6.52-103.82; P < .001). The absence of LEAP procedure was also significantly associated with recurrent cyclops syndrome with an OR of 8.49 (95% CI, 1.64-43.97; P = .011). Last, a time from ACL surgery to first cyclops surgery of <7 months was associated with an OR of 13.62 (95% CI, 4.07-45.66; P < .001) compared with a time >7 months.
Postoperative Knee Mobility
The surgery improved all patients at 6 weeks postoperatively in terms of extension deficit and flexion (P < .05). However, patients in the relapse group had a greater extension deficit at 6 weeks postoperatively, with a median of 10° (5°-20°) compared with 0° (0°-5°) in the no relapse group (P < .001) (Table 3).
Outcome Measure at 6 Weeks After Arthrolysis in the No Relapse Group and Second Arthrolysis in the Relapse Group a

Data are presented as median (min-max) or n (%). Post, postoperative; Preop, preoperatively.
Subgroup Analysis of Cyclops Outcomes at 6 Weeks After Initial Arthrolysis
After initial arthrolysis, the median residual extension deficit at 6 weeks was significantly higher in the relapse group (median: 5°; min-max: 0°-10°) than in the no relapse group (median: 0°; min-max: 0°-5°; P≤ 00.1) (Table 4).
Subgroup Analysis of Mobility Between the No Relapse and Relapse Groups at 6 Weeks After the First Arthrolysis for Cyclops Syndrome a

Data are presented as median (min-max) or mean ± SD. The Bold P value indicates statistical significance.
Discussion
The main finding of this study was that recurrent cyclops syndrome occurred in 6.9% of patients after initial surgery for cyclops syndrome. The key risk factors identified included age >27 years, a time of <7 months between ACL surgery and initial cyclops surgery, and specific surgical factors such as graft type and absence of a LEAP.
Risk Factors
In a large literature review, Noailles et al 17 found that cyclops syndrome prevalence was between 1.9% and 10.2%. While the graft type does not influence the risk of primary cyclops syndrome,1,8,20,21,26 in our series, we found a higher proportion of BPTB and ST4 grafts in the relapse group compared with the no relapse group. This finding raises questions about the role of graft size in the recurrence of cyclops syndrome, as ST4 and BPTB grafts are generally large-volume grafts. This aligns with the literature, which indicates that an increased graft-to-notch size ratio is a known risk factor for cyclops syndrome.9,11 However, the confidence interval for this factor is large in our study, which may limit its reliability. This limitation arises because the number of BPTB grafts in our study is relatively small (n = 38 BPTB) compared with the G2ST2 technique.
Our study demonstrates that patients who did not receive LEAP were exposed to a higher odds of relapse (OR, 7.63). As indicated in the literature,4,10 repetitive microtrauma may perpetuate the fibrotic process responsible for nodule formation. For instance, Delcogliano et al 4 postulated that the microtrauma responsible for the formation of the granulation tissue and then the formation of the nodule could be related to the micromotion between the bone rim of the tibial tunnel and the neo ligament. This could explain the higher recurrence rate observed in the group without LEAP.
Other risk factors identified in this study include age, with patients >27 years having 11 times the risk of experiencing cyclops relapse. While age is not commonly recognized as a risk factor for primary cyclops, this finding contrasts with earlier studies, such as that by Wang and Ao, 27 which asserted that age does not influence the risk. However, their study was limited to 24 cases and analyzed age only as a continuous factor, without the detailed ROC and categorical analysis we conducted. The increased risk in older patients may be due to slower rehabilitation, which increases the risk of stiffness and extension deficit. Other potential causes might include decreased tissue elasticity, different graft healing dynamics, and increased scar formation.
A noteworthy finding of this study was that patients operated for cyclops before 7 months of surgery were exposed to a higher risk of recurrence (OR, 12.35). This timeline aligns with the ligamentization process of the ACL, known to occur between 6 and 48 months after surgery.14,30 Studies have shown that during the initial 6 months after surgery, the MRI signal intensity of the ACL graft increases, which then starts to decline.25,28 This pattern corresponds with histological findings that show high levels of vascularity and cell proliferation occurring during the early remodeling phase, which typically spans from 3 to 9 months postoperatively.4,18,19 Given the cyclops formation physiopathology, which involved high vascularity leading to scar tissue formation, 29 we hypothesized that operating within this early period of intense vascular activity would predispose patients to a higher risk of recurrence. The heightened vascularity and cell activity could contribute to more aggressive scar tissue development, thus increasing the likelihood of cyclops reformation. However, this hypothesis should not necessarily recommend delaying treatment of cyclops, as long-term functional outcomes were not analyzed in this study.
Postoperative Knee Mobility
Early postoperative presence of active extension deficit is described in the literature as a risk factor for cyclops syndrome.3,8,21 In our series, although there was a significant improvement in range of motion after treatment of the first episode of cyclops syndrome, the persistence of an early postoperative active extension deficit seems to contribute to the recurrence of cyclops syndrome. Potential factors that might interact in the development of early extension deficit include incomplete fibrous tissue resection, anterior graft placement, or a narrow intercondylar notch, leading to impingement.3,4,8,11,17,21 In addition, arthrogenic muscle inhibition may further limit extension. 22
Limitations
This study is subject to certain limitations. First, this was an observational, retrospective study. As the recurrence of cyclops syndrome is a rare event, data were collected on a small number of patients (n = 25), and conclusions should be treated with caution. A longer follow-up period and functional scores could be beneficial to draw more robust conclusions. Second, some studies have emphasized the possibility that a narrow notch is a risk factor for cyclops syndrome.3,11 However, this was not assessed in this study. Moreover, tunnel placement was not evaluated, although it may influence impingement risk and fibrotic tissue formation. Another limitation of the study was that age and time from ACLR to arthrolysis cutoffs were based on a relatively low Youden index, which may limit their discriminative ability. However, these cutoffs were used only as supplementary analyses, with the primary analysis conducted on these variables as continuous data. Finally, no histological analysis of the cyclops lesions was performed to assess the impact of any increased vascular activity or inflammatory markers on the development of recurrent cyclops lesions.
Conclusion
This study found a 6.9% rate of recurrent cyclops syndrome in patients already undergone arthroscopic arthrolysis after ACLR. Significant risk factors include age, type of graft, absence of LEAP, and shorter time from ACL surgery to initial cyclops surgery. Among patients who underwent surgery for the first time for cyclops, those who had residual extension deficit at 6 weeks postoperatively were more likely to experience recurrent cyclops syndrome.
Footnotes
Final revision submitted February 21, 2025; accepted March 4, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: N.L. is a consultant for the Websurvey Society. A.H. is a consultant for Arthrex and DePuy. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Groupe Hospitalier Pitié-Salpêtrière.