
Abstract
Background:
Several studies on the relationship between morphological parameters and posterior cruciate ligament (PCL) injury have already been conducted. However, few studies focused on the association between the morphology of the tibial ridge and PCL injury, especially in isolated PCL cases.
Purpose:
To retrospectively compare tibial ridge morphology between patients with isolated PCL tear and age/sex-matched controls with intact PCL after a knee injury.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
In a single center, 78 patients who were diagnosed with isolated PCL tears, confirmed by magnetic resonance imaging (MRI) or arthroscopy, were retrospectively analyzed. The control group consisted of 78 patients who had sustained knee trauma but showed no structural damage on MRI. MRI was used to measure the geometry of the tibial ridge, including the height of the medial tibial ridge (HMTR), the height of the lateral tibial ridge (HLTR), the width between ridges (WR), the slope length (SLPIR), the slope angle of the posterior intercondylar ridge, and the height of the posterior intercondylar ridge (HPIR). Tibial plateau was evaluated with the medial posterior tibial slope (MPTS), the lateral posterior tibial slope (LPTS), and the width of the tibial plateau (WTP). The mean values of these parameters were analyzed using a paired t test, and binary logistic regression analyses were conducted.
Results:
No significant differences were found in age, limb side, or body mass index between groups. Among all patients, those with isolated PCL ruptures demonstrated significantly greater HMTR (9.02 vs 8.12 mm; P < .001), HLTR (8.32 vs 7.26 mm; P < .001), HPIR (16.20 vs 15.56 mm; P = .01), and SLPIR (21.71 vs 21.03 mm, P = .015), along with a narrower WR (11.33 vs 12.58 mm; P < .001), compared with the control group. Sex-specific analysis showed consistent trends in both male and female patients. In addition, male patients exhibited a smaller WTP (7.78 vs 7.92 cm; P = .033) and a lower MPTS (6.86°vs 8.46°; P = .008) compared with female patients. Binary logistic regression identified increased HMTR (hazard ratio [HR], 1.51; P = .028) and HLTR (HR, 1.371; P = .028) as risk factors, while narrower WR was protective (HR, 0.807; P = .007).
Conclusion:
A high and narrower tibial ridge is associated with isolated PCL tears, compared with PCL-intact controls. In sex-stratified analyses, smaller tibial plateau width and reduced MPTS were observed in male patients with PCL compared with male controls, suggesting that the anatomic associations with PCL injury may differ between sexes.
Keywords
Posterior cruciate ligament (PCL) injuries are typically associated with high-energy trauma, often resulting from an impact on the anterior proximal tibia, which forces the tibia to displace posteriorly.22,26,27,30 Despite our understanding of PCL injury mechanisms, the low occurrence rate of these injuries has resulted in a scarcity of literature investigating the anatomic geometry of the knee joint and its association with PCL injury, particularly in isolated cases.3,36
The tibial ridge is a distinct anatomic structure within the posterior intercondylar area of the tibia, playing a crucial role in guiding knee joint kinematics.21,22,32 Specific morphological features of the tibial ridge, such as increased height, greater slope length (SLPIR), and steeper slope angle, may increase the risk of PCL impingement during knee flexion. 34 Few studies have examined the relationship between the PCL injury and tibial ridge morphology. Van Kuijk et al 31 utilized radiographs to outline the tibial ridge with the contour, concluding that a more flattened tibial ridge is related to PCL rupture. 31 Furthermore, Weili et al 34 observed that the sagittal geometry of the posterior intercondylar eminence is greater compared with instances of traumatic anterior cruciate ligament (ACL) ruptures 34 ; however, there is still limited research on tibial morphology and its association with isolated PCL injury compared with a normal knee. This study aimed to retrospectively compare the tibial proximal morphology between isolated PCL tear patients and age- and sex-matched patients with knee trauma but no structural damage evident on magnetic resonance imaging (MRI). We hypothesized that patients with isolated PCL injuries would exhibit tibial morphology characteristics, such as a higher posterior intercondylar eminence and a steeper slope angle, which increase the risk of PCL impingement against the tibial ridge during knee flexion.
Methods
Study Design
Following institutional review board approval, we performed a case-control study in our single center. All patients with an injured knee who visited the outpatient clinic of our hospital between 2012 and 2022 were eligible for inclusion. The patient’s history, results of physical examination, and MRI were used to confirm the diagnosis and assess for any additional injuries. Patients diagnosed with isolated grade 3 PCL injuries with symptoms of pain or instability, meeting the surgical criteria, were included with the following criteria: (1) traumatic grade 3 PCL rupture identified by MRI or arthroscopy; (2) positive posterior drawer test; and (3) MRI images acquired within 6 months after injury using our Picture Archiving and Communication System (PACS) system, maintaining measurement consistency. The exclusion criteria were as follows: (1) combined knee fracture— including PCL avulsion fractures; (2) combined knee ligament tears—including ACL, medial collateral ligament, lateral collateral ligament, patellar tendon; grade >2), meniscal tears (grades 2 and 3); and (3) detectable osteoarthritis (Kellgren-Lawrence grade >2).
The control group was selected from patients who had knee trauma but no structural damage evident on MRI. Patients were excluded if they had (1) evidence of ligament laxity on physical examination, (2) evidence of PCL injury (grades 1-3) defined by MRI or arthroscopy, (4) combined fractures, other knee ligament tears, or detectable osteoarthritis (grade >2) as mentioned.
Imaging Evaluation
All MRI examinations were retrospectively reviewed by 2 fellowship-trained musculoskeletal surgeons (K.Q. and C.W.), each with 8 years of clinical experience, who were blinded to the patients’ history and physical examination. To assess inter- and intrarater agreement, these 2 musculoskeletal surgeons reviewed all MRI examinations from the study group twice, with a 2-month interval between sessions to prevent recall bias. All patients were examined using a 1.5-T MRI (Discovery 750; GE Medical Systems), which included sagittal, coronal, and axial sequences containing both T1- and T2-weighted phases. The scan parameters included the echo time, 25 to 30 msec; repetition time, 2000 to 3000 msec; and slice thickness, 4 mm with no gap. The images were obtained from our hospital’s PACS. Patients were provided clear and standardized instructions regarding leg positioning to maintain consistency across scans. Post-scan reviews were performed by our radiologic technologists and MRI reviewers to assess the positioning and image quality.
According to Iriuchishima et al,13,14 we measured the height of the medial tibial ridge (HMTR), the height of the lateral tibial ridge (HLTR), and the width between ridges (WR). According to Weili et al,11,34 the SLPIR and the slope angle (SAPIR) of the posterior intercondylar ridge, the medial posterior tibial slope (MPTS), the lateral posterior tibial slope (LPTS), the height of the apex of the posterior intercondylar ridge (HPIR), and the width of the tibial plateau (WTP) were measured as well. To obtain a complete view of the height of the entire tibial ridge, coronal images were used for analysis. On the level where the highest height of the tibial crest can be seen, we first made a straight line connecting the inner and outer peaks of the tibial plateau, and then made the vertical lines from the medial and lateral peaks of the tibial ridge, respectively. The length of the vertical line is the highest height of the tibial ridge, and the distance between the 2 vertical lines is the tibial ridge distance (Figure 1).13,14 After defining the sagittal-plane longitudinal central axis of the tibia, a perpendicular reference line was drawn from the lowest tibial attachment of the PCL to this axis. The HPIR was then measured as the perpendicular length from the apex to the reference line. The SLPIR was measured as the distance from the apex of the posterior intercondylar eminence to the lowest tibial attachment of the PCL. The SAPIR was measured as the angle between the reference line and the tangent of the slope of the posterior intercondylar eminence (Figure 2).

Measurements of the HMTR, HLTR, WTP, and WR in a patient with an isolated PCL-torn using a coronal T1 MRI of the left knee. A coronal T1 MRI of a left knee with PCL tear. A straight joint line connecting the inner and outer peaks of the tibial plateau; the distance from the medial to lateral edges of the joint line is WTP. From the top of the medial and lateral tibial ridge, a perpendicular line was drawn to the joint line. The length between the top of the tibial ridge and the cross point of the perpendicular line and the joint line was regarded as the height of the tibial ridge. The length between the cross point of the medial perpendicular line and the joint line, the lateral perpendicular line and the joint line was regarded as the WR. HLTR, height of lateral tibial ridge; HMTR, height of medial tibial ridge; MRI, magnetic resonance imaging; PCL, posterior cruciate ligament; WR, width between ridges; WTP, width of the tibial plateau.

Measurements of HPIR, SLPIR, and SAPIR in a patient with PCL-intact and meniscal injury using a sagittal T2 MRI. (A) Reference line. (B) The HPIR was measured as the perpendicular length from the apex to the reference line, and the SLPIR was measured as the distance from the apex to the lowest tibial attachment of the PCL. (C) The SAPIR was measured between the reference line and the tangent of the slope of the posterior intercondylar ridge. HPIR, height of posterior intercondylar ridge; MRI, magnetic resonance imaging; PCL, posterior cruciate ligament; SAPIR, slope angle of posterior intercondylar ridge; SLPIR, slope length of posterior intercondylar ridge.
Statistical Analysis
All analyses were performed using SPSS Statistics (Version 25.0; IBM). The alpha level was set at .05 for statistical significance. A 2-way random effects model was used to assess the inter- and intrarater agreement for imaging evaluation and calculate the intra- and interobserver intraclass correlation coefficient (ICC). The significance of ICC values is as follows: 0<ICC<0.40, poor agreement; 0.4<ICC<0.7, fair to good agreement; 0.7<ICC<1, excellent agreement. 9 A power analysis was performed to determine the adequacy of the sample size; 32 patients would provide 90% power to detect a difference in the HPIR at an alpha level of .05, according to Weili et al. 34 Means and standard deviations were calculated to describe continuous data. After examining the normality, a paired t test was used to compare the mean difference of those morphological characteristics between the PCL rupture group and control groups, and in the male and female groups, respectively. In addition, binary logistic regression was performed to analyze exposure hazard ratios (HRs) for each morphological characteristic.
Results
The patient characteristics of the PCL rupture group and the control group are presented in Table 1. Overall, 78 patients with isolated PCL rupture met the criteria and were enrolled in the study (Figure 3), and 78 control patients were matched to the PCL rupture group according to age and sex. There were no significant differences in age (P = .169), limb side (P = .574), or body mass index (P = .887) between the control and PCL-injured groups.
Patient Characteristics a

Data are presented as n/n or mean ± SD. BMI, body mass index; PCL, posterior cruciate ligament.

A flowchart of case selection in this study. The flowchart shows selection criteria for the 100 patients in the study group. Examples of conditions that may change the native tibial bone geometry include severe posttraumatic deformity (n = 2), congenital deformities (patellar instability with trochlear dysplasia) (n = 2), advanced rheumatoid arthritis, and gout with bone erosion (n = 3). ACL, anterior cruciate ligament; LCL, lateral collateral ligament; MCL, medial collateral ligament; OA, osteoarthritis; PCL, posterior cruciate ligament; PLC, posterolateral corner; PT, patellar tendon.
Before comparing morphological characteristics, Kolmogorov-Smirnov or Shapiro-Wilk normality tests indicated the normality for the data between groups (Table 2); then, a paired t test was implemented (Tables 3 and 4). Among all patients, those with isolated PCL ruptures demonstrated significantly greater HMTR (9.02 ± 1.43 vs 8.12 ± 1.74 mm; P < .001), HLTR (8.32 ± 1.77 vs 7.26 ± 1.48 mm; P < .001), and HPIR (16.20 ± 2.69 vs 15.56 ± 1.26 mm; P = .01), along with a narrower WR (11.33 ± 2.40 vs 12.58 ± 2.41 mm; P < .001), compared with the control group. In addition, significant differences were observed in the SLPIR (21.71 ± 2.40 vs 21.03 ± 1.38 mm; P = .015) and MPTS (7.52°± 3.85° vs 8.47°± 2.74°, P = .035) (Figure 4). No significant differences were observed in SAPIR (women: P = .693; men: P = .574) and LPTS (women: P = .989; men: P = .617) between PCL rupture and control groups. When stratified by sex, both male and female patients with PCL injuries had significantly higher HMTR (women: 8.36 vs 6.44 mm; men: 9.31 vs 8.85 mm; P < .05), HLTR (women: 7.70 vs 6.20 mm; men: 8.58 vs 7.71 mm; P < .01), HPIR (women: 16.87 vs 15.56 mm; men: 17.90 vs 17.21 mm; P < .05), and lower WR (women: 10.11 vs 11.46 mm; men: 11.70 vs 13.07 mm, P < .05) than their sex-matched controls. Moreover, male patients with PCL showed a smaller WTP (7.78 vs 7.92 cm; P = .033) and a reduced MPTS (6.86° vs 8.46°; P = .008) compared with female patients. To standardize the data, we calculated the ratio of these parameters by WTP to reduce the effect of inherent structural differences on the results (Table 5).
Normality Tests of the Morphological Characteristics a

HLTR, height of the lateral tibial ridge; HMTR, height of the medial tibial ridge; HPIR, the height of the apex of the posterior intercondylar ridge; K-S, Kolmogorov-Smirnov; PCL, posterior cruciate ligament; SAPIR, slope angle of the posterior intercondylar ridge; SLPIR, slope length of the posterior intercondylar ridge; S-W, Shapiro-Wilk; WR, width between ridges; WTP, width of the tibial plateau.
Comparison of the Morphological Characteristics by Sex a

Data are reported as mean degrees ± SD, unless otherwise indicated. Bold P values indicate significance. HLTR, height of the lateral tibial ridge; HMTR, height LPTS, lateral posterior tibial slope the medial tibial ridge; HPIR, height of posterior intercondylar ridge; MPTS, medial posterior tibial slope; PCL, posterior cruciate ligament; SAPIR, slope angle of posterior intercondylar ridge; SLPIR, slope length of posterior intercondylar ridge; WR, width between ridges; WTP, width of tibial plateau.
Paired T-Test of the Morphological Characteristics of All Patients a

Data are reported as mean ± SD, unless otherwise indicated. Bold P values indicate significance. HLTR, height of the lateral tibial ridge; HMTR, height LPTS, lateral posterior tibial slope the medial tibial ridge; HPIR, height of posterior intercondylar ridge; MPTS, medial posterior tibial slope; PCL, posterior cruciate ligament; SAPIR, slope angle of posterior intercondylar ridge; SLPIR, slope length of posterior intercondylar ridge; WR, width between ridges; WTP, width of tibial plateau.

High and narrower tibial ridge in PCL tears. (A) Control group, a coronal T1 MRI of a left knee showed a wide and short tibial ridge. (B) PCL rupture group, a coronal T1 MRI of a left knee with isolated PCL rupture without fracture or ligament injury showed a narrow and high tibial ridge. MRI, magnetic resonance imaging; PCL, posterior cruciate ligament.
Paired T Test of the Uniformed Morphological Characteristics a

Data are reported as mean ± SD, unless otherwise indicated. Bold P values indicate significance. HLTR, height of the lateral tibial ridge; HMTR, height LPTS, lateral posterior tibial slope the medial tibial ridge; HPIR, height of posterior intercondylar ridge; PCL, posterior cruciate ligament; SLPIR, slope length of posterior intercondylar ridge; WTP, width of tibial plateau.
We also conducted a comparison of morphological parameters between male and female participants and found that HMTR, HLTR, WR, WTP, HPIR, and SLPIR were significantly greater in male than in female patients (P < .001 for all). No significant sex differences were observed in SAPIR, MPTS, or LPTS (P > .05) (AppendixTable A1).
Binary logistic regression analyses were performed to identify independent anatomic predictors of isolated PCL rupture (Table 6). In the overall cohort, several morphological parameters were independently associated with the presence of isolated PCL rupture. Increased HMTR (HR, 1.51; P = .028) and HLTR (HR, 1.371; P = .028) were significant risk factors, while narrower WR (HR, 0.807; P = .007) was inversely associated with PCL injury. Other variables, including WTP, HPIR, SLPIR, SAPIR, MPTS, and LPTS, did not reach statistical significance in the full cohort (P > .05 for all). Among female patients, increased HMTR (HR, 1.603; 95% CI, 1.094-2.349; P = .016), HLTR (HR, 2.015; 95% CI, 1.286-3.156; P = .002), HPIR (HR, 1.487; 95% CI, 1.074-2.058; P = .017), and SLPIR (HR, 1.632; 95% CI, 1.166-2.285; P = .004) were significantly associated with higher odds of PCL injury, while narrower WR was a protective factor (HR, 0.756; 95% CI, 0.592-0.964; P = .024). In male patients, similarly significant associations were observed for HMTR (HR, 1.444; 95% CI, 1.098-1.898; P = .008), HLTR (HR, 1.378; 95% CI, 1.097-1.730; P = .006), HPIR (HR, 1.194; 95% CI, 1.006-1.417; P = .042), and SLPIR (HR, 1.171; 95% CI, 1.003-1.367; P = .045). WR remained inversely associated with PCL rupture risk (HR, 0.733; 95% CI, 0.621-0.864; P < .001), while a narrower WTP (HR, 0.281; P = .007) and reduced MPTS (HR, 0.865; P = .006) were also significant predictors. SAPIR and LPTS were not significantly associated with PCL rupture in either sex.
Binary Logistic Regression of All Patients a

Bold P values indicate significance. HLTR, height of the lateral tibial ridge; HMTR, height of the medial tibial ridge; HPIR, height of posterior intercondylar ridge; HR, hazard ratio; LPTS, lateral posterior tibial slope; MPTS, medial posterior tibial slope; SAPIR, slope angle of posterior intercondylar ridge; SLPIR, slope length of posterior intercondylar ridge; WR, width between ridges; WTP, width of tibial plateau.
Our radiographic measurements had excellent intra- and interrater reliability, both fell within the excellent agreement interval (Table 7).
Intra- and Interrater ICC a

HLTR, height of the lateral tibial ridge; HMTR, height of the medial tibial ridge; HPIR, height of posterior intercondylar ridge; ICC, intraclass correlation coefficient; LPTS, lateral posterior tibial slope; MPTS, medial posterior tibial slope; SAPIR, slope angle of posterior intercondylar ridge; SLPIR, slope length of posterior intercondylar ridge; WR, width between ridges; WTP, width of tibial plateau.
Discussion
The main finding of this study was that patients with isolated PCL rupture exhibited significantly higher medial and lateral tibial ridges, a narrow intercondylar ridge distance, and a higher sagittal posterior intercondylar ridge compared with PCL-intact controls. These differences were consistently observed in both male and female subgroups. In addition, in male patients, a significantly lower MPTS and a smaller WTP were also noted, suggesting that certain anatomic characteristics associated with PCL injury may differ by sex.
The tibial ridge is a product of evolution, which may have evolved to resist internal and external rotation of the knee and support vertical body positions and motion.29,35 However, the tibial ridges are subjected to contact stress between the tibiofemoral articulation, and their size as well as position determine the motion of the knee and the risk of impingement during flexion.17,33 From the perspective of motion mechanics, a sudden posteriorly directed force applied to the proximal tibia may cause impingement between the bony structures and stretched ligaments, and a high tibial ridge would increase the risk of contact. Amis et al 1 describe the bony attachments of the PCL, its fiber anatomy, and the patterns of tightening and slackening during knee flexion–extension with an anatomic paper. In deep knee flexion, the PCL passes through a narrowing gap between the posterior aspect of the femur and the tibial plateau; and it is a potential injury mechanism when a person falls onto the tibial tuberosity with the knee flexed, as PCL may be compressed or sheared between the bones during hyperflexion, especially with a high and sharp-shaped front tibial ridge (Figure 5). MRI research supported this mechanism with the finding that the PCL would gradually approach the posterior intercondylar ridge during flexion.5,21 A similar case-control study by Weili et al 34 further supports this mechanism, reporting a greater sagittal HPIR and SLPIR for PCL-injured participants compared with ACL injury controls. A key methodological distinction lies in the control group selection: whereas Weili et al used ACL-injured patients as controls, our study employed patients with knee trauma but no structural damage evident on MRI. This difference in cohort design may explain the discrepancies in SAPIR findings between the 2 studies. Moreover, their study overlooked the general tibial plateau morphology and unique bony characteristics potentially predisposing to ACL injuries, contrasting with our focus on how a steeper SAPIR is linked to PCL rupture. In extension, the PCL is curved concave forward away from the ridge. While in full flexion, PCL becomes straight and curves convex forward over the roof of the intercondylar notch, with a good chance of hitting the front tibial ridge. In addition, there is an inverse relationship between the size and shape of the tibial ridge and the volume of the intercondylar notch: a larger or hyperplastic tibial ridge reduces the notch volume, compressing and bending the PCL, which alters its trajectory and tension distribution. 18
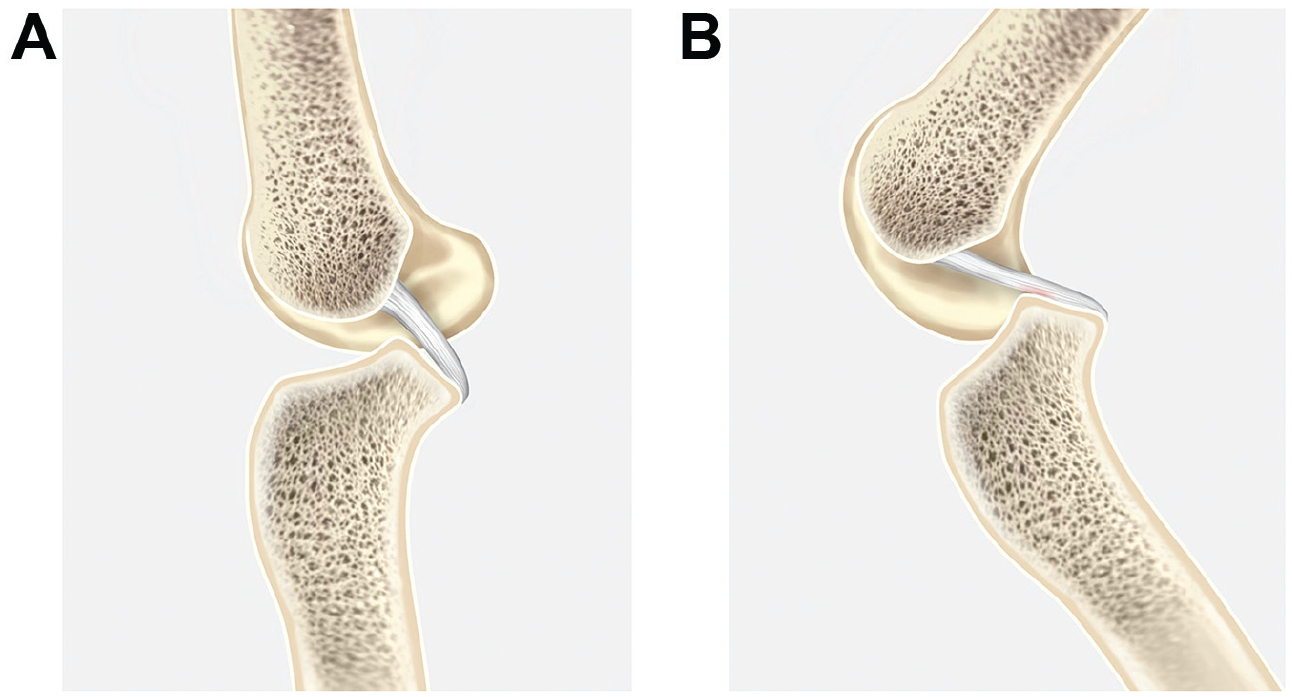
The diagram shows the relationship between the high and narrower tibial ridge and the movement of the posterior cruciate ligament. (A) Relaxation of the PCL in the case of a straight knee joint. (B) Demonstrated impingement between the high and narrower tibial ridge and the PCL during knee flexion. PCL, posterior cruciate ligament.
We also explored the tibial plateau size and slope between injured participants and controls. Because the mean natural inclination of the tibia is thought to have a significant effect on the in-situ force experienced by the cruciate ligament, it is thought that changes in the inclination of the tibia plateau may alter the normal motion mechanics of the knee joint. Morphological changes in the tibial plateau are thought to be related to the injury of ACL and PCL, and may be anatomic differences for primary PCL tear.2,6,7 Moreover, differences in tibial plateau geometry between sexes and individuals may influence knee injury susceptibility, osteoarthritis development, and the outcomes of knee arthroplasty procedures. 10 By biomechanical tests in vitro, Bernhardson et al 2 concluded that PCL graft forces significantly increased as PTS decreased.2,16 In our study, we noticed that male patients with PCL tears had significantly decreased MPTS and smaller WTP, which differed from female patients (Table 3). This is supported by a similar case-control study performed by Fan et al, 8 in which no statistical difference in LPTS was found between the PCL rupture group and the control group in both sexes, while MPTS showed a significant difference among male groups only. This may suggest different injury mechanisms between male and female patients, such as anatomic and biomechanical variations that influence ligament loading patterns.20,24,28 The medial tibial plateau mainly affects the stability of the knee joint in the anteroposterior direction, while the lateral tibial plateau is mainly related to the stability of the knee joint rotation. 37 Our study indicates that men were more frequently affected by PCL injuries than women in our cohort (55 vs 23), and sex-stratified analysis revealed that certain anatomic characteristics associated with PCL injury differed between men and women. This disparity may be influenced not only by anatomic differences but also by factors such as sex-based variations in neuromuscular control, biomechanical properties, hormonal levels, injury mechanisms, and landing mechanics, as suggested in previous studies.19,37
The morphological characteristics of the tibial ridge identified in this study may have implications for graft protection and surgical planning in patients undergoing PCL reconstruction. Baoshan et al recommend conservative weightbearing after PCLR for patients with shallow medial tibial depth or small lateral poseterior tibal slope angles to avoid graft issues, while dynamic braces and quadriceps strengthening help stabilize knees in those with narrow tibial ridges.15,23,25 Although targeted surgical solutions are yet to be reported, potential directions exist. For example, arthroscopic resection of excessively large tibial spines and advanced techniques like selective bone resection combined with hybrid fixation, and shaping the medial condyle’s lateral wall might be potential in addressing such prominent tibial ridge abnormalities4,12; nonetheless, further research is needed to confirm their effectiveness. Our findings highlight the potential value of preoperative assessment of tibial ridge parameters, which may help identify patients at greater risk for postoperative instability or graft failure. These anatomic insights could serve as a foundation for future research aimed at improving individualized surgical strategies and rehabilitation protocols.
Limitations
We acknowledge some limitations to our study. (1) Given the low incidence and uneven sex distribution of PCL rupture, our study has a limited sample size, which may affect the credibility of the study. (2) The enrollment was limited to Chinese, and ethnicity may be an important factor affecting the bone structure. (3) Because of the retrospective design of this study, certain variables—eg, injury mechanism, daily activity levels, and technical factors related to MRI acquisition—were not standardized. Consequently, residual confounding factors that may have influenced the results cannot be entirely ruled out.
Conclusion
In our cohort, we found that a high and narrower tibial ridge may be significantly associated with isolated PCL tears, when compared with age- and sex-similar traumatic PCL-intact injury controls. In sex-stratified analyses, smaller tibial plateau width and reduced MPTS were observed in male PCL patients compared with male controls, suggesting that the anatomic associations with PCL injury may differ between sexes.
Footnotes
Appendix
Comparison of Morphological Parameters Between Male and Female Groups a

| Male Group | Female Group | P | |
|---|---|---|---|
| HMTR | 9.10 ± 1.44 | 7.89 ± 1.48 |
|
| HLTR | 8.14 ± 1.67 | 7.06 ± 1.51 |
|
| WR | 12.37 ± 2.41 | 10.89 ± 2.25 |
|
| WTP | 7.86 ± 0.45 | 6.85 ± 0.57 |
|
| HPIR | 17.55 ± 2.01 | 16.22 ± 2.01 |
|
| SLPIR | 23.79 ± 2.22 | 21.79 ± 1.96 |
|
| SAPIR | 47.90 ± 4.87 | 48.17 ± 4.76 | .624 |
| MPTS | 7.80 ± 3.40 | 8.49 ± 3.66 | .649 |
| LPTS | 5.93 ± 3.76 | 6.39 ± 4.27 | .749 |
Data are presented as mean ± SD. Bold P values indicate significance. HLTR, height of the lateral tibial ridge; HMTR, height of the medial tibial ridge; HPIR, height of posterior intercondylar ridge; LPTS, lateral posterior tibial slope; MPTS, medial posterior tibial slope; SAPIR, slope angle of posterior intercondylar ridge; SLPIR, slope length of posterior intercondylar ridge; WR, width between ridges; WTP, width of tibial plateau.
Final revision submitted April 15, 2025; accepted May 1, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The Second Affiliated Hospital, School of Medicine, Zhejiang University (R2022-1003/I20221199).