
Abstract
Background:
Bone contusions after acute posterior cruciate ligament (PCL) injury are commonly observed on magnetic resonance imaging (MRI), providing insight into potential mechanisms of injury.
Purpose:
To quantify the size of bone contusions and their locations—lateral tibial plateau (LTP), lateral femoral condyle (LFC), medial tibial plateau (MTP), medial femoral condyle (MFC), and subspinous subregion (SS)—observed on MRI scans of isolated PCL-torn knees acquired within 4 weeks after injury.
Study Design:
Cross-sectional study. Level of evidence, 3.
Methods:
We retrospectively reviewed the clinic notes, operative notes, and imaging of 72 patients (55 men and 17 women) with a grade 2 or 3 primary isolated PCL tear, without any fractures, meniscal tears, or other knee ligament tears, whose MRI scans were obtained within 4 weeks of the injury. The location (LTP, LFC, MTP, MFC, and SS), combined number of compartments, and volume of the bone contusion were recorded based on the MRI Osteoarthritis Knee Score (MOAKS) system—a standardized semi-quantitative mapping technique.
Results:
Contusions were observed in 59 of 72 (81.9%) patients. According to the MOAKS system, areas with a high frequency of bone contusion were anterior SS (30; 41.7%), anterior LTP (26; 36.1%), anterior MTP (24; 33.3%), and posterior LFC (23; 31.9%). Female patients showed significantly higher incidence of bone contusion than male patients in the posterior LTP (P = .024), anterior LFC (P = .017), posterior LFC (P = .006), total MFC (P < .001), and posterior SS (P = .039).
Conclusion:
Bone contusion was observed in most patients with acute isolated PCL rupture. The most common contusion locations observed were anterior SS, anterior LTP, anterior MTP, and posterior LFC. Female patients demonstrated a greater prevalence and extent of bone contusions compared with their male counterparts.
Bone contusion—often referred to as bone bruises or occult osseous subchondral lesions—has recently become a topic of interest in the orthopaedic literature.13,39,59,62 These lesions are commonly used to describe ill-defined magnetic resonance signal changes of bone marrow, and are thought to represent a spectrum of occult bone injuries—including bleeding, inflammation, infarction and edema due to microscopic compression fractures of cancellous bone caused by bone contact.22,34 Histologic evaluation of bone biopsy specimens revealed microfractures of cancellous bone, edema, and bleeding in the fatty marrow when bone contusion appears. 54
The real value of identifying bone contusion lies in gaining insight into the biomechanics of the injury mechanism. It is also easier to identify on imaging than meniscal and other soft tissue injuries, which facilitates a more systematic and focused evaluation of joint injuries. 56 In the context of other knee ligament injuries, such as anterior cruciate ligament (ACL) injury, studies have hypothesized that lateral bruising is related to valgus collapse, while medial bruising is representative of extension and anterior tibial translation, which may help explain injury mechanisms.4,21 Video analysis has been used to estimate knee position at the time of ACL rupture, offering key insights, but is limited by camera sensitivity and the inability to capture the exact moment of injury.5,8,9,18,46 As a result, observed knee angles may represent the effects, not the cause, of ACL rupture. 46 This limitation also applies to studies of posterior cruciate ligament (PCL) rupture mechanisms. Magnetic resonance imaging (MRI)-based bone contusion patterns show high concordance with video analyses of injury mechanisms in ACL ruptures, offering an alternative method for studying injury. 8
Moreover, during bone remodeling, the related subchondral bone areas become stiffer, and signs of early osteoarthritis may appear, suggesting that the initial signal changes in the bone marrow may contribute to the predisposition of the knee to degenerative changes. 23 Thus, it is of interest to study the distribution pattern of bone contusion in patients with isolated PCL injury, from which the relevant mechanism of PCL injury can be inferred. Current research indicates that while PCL reconstruction surgery can achieve certain functional recovery in the short term, a significant number of patients have residual laxity and up to 30% have arthritis and degenerative changes in the long term.6,25,27,28,64 A better understanding of potential PCL injury mechanisms may allow for risk prevention strategies.
Several reports have documented bone contusion in >83% of patients after acute rupture of the PCL. Only Mair et al 33 described the distribution pattern of bone contusion in 35 patients with PCL rupture. They found that, although bone contusion in patients with PCL rupture has a similar incidence to that in ACL rupture, it does not follow a fixed pattern. However, the evaluation of bone contusion in that study did not consider the specific distribution (anterior, central, posterior) of bone contusion as well as its volume size, and they also included patients with other combined injuries, such as fractures and other ligament injuries, which may affect the distribution pattern of bone contusion. As bone contusions may resolve over time, the time from injury to MRI acquisition may affect the observation of bone contusions. However, the reported time for the resolution of bone bruising varies from as early as 3 weeks to 2 years.33,34 Given this insight, this study aimed to document the distribution of bone contusion patterns using the MRI Osteoarthritis Knee Score (MOAKS) system in patients with acute, isolated PCL injuries within 4 weeks after injury, and then to gain a better understanding of the injury mechanisms involved. 19 Thus, we hypothesized that in patients with isolated PCL rupture, bone contusions were predominantly located on the anterior aspect of the tibial plateau and the posterior aspect of the lateral femoral condyle. We further hypothesized that female patients would exhibit a higher frequency and greater volume of bone contusions compared with male patients.
Methods
Inclusion Criteria
Following approval from the hospital, clinic notes and medical imaging (arthroscopy and MRI) were reviewed from patients who presented with complaints of knee pain and were diagnosed with a PCL injury upon evaluation between 2009 and 2021 by 2 fellowship-trained sports medicine orthopaedic surgeons (Y.X. and Z.P.). This included patients treated both nonoperatively and operatively. The inclusion criteria were as follows: (1) clinical examination showing a grade 2 or 3 rupture of the PCL, and MRI showing a high-grade partial rupture or complete rupture of the PCL; and (2) MRI performed within 4 weeks of injury. From the initial 1045 patients identified, the following exclusion criteria were applied: (1) MRI performed >4 weeks after injury; (2) grade 1 PCL injury or posterior drawer test grades 0 to 2; (3) associated bone fracture, including avulsion fracture of tibial insertion of the PCL; (4) associated ACL, medial collateral ligament (MCL), lateral collateral ligament (LCL), patellar tendon, (PT) or meniscal tears (grades 2-3 for any of the above); (5) history of knee surgery; (6) previous knee trauma; (7) presence of rheumatoid arthritis or osteoarthritis (Kellgren-Lawrence >2); or (9) MRI performed at another institution. Consequently, bone fractures can affect the judgment of bone contusions. To better analyze PCL injury mechanisms, contusions caused by ligament avulsions were not considered in this study.
The time between injury and MRI acquisition was documented through a review of clinic notes and MRI reports. All 96 patients underwent MRI on a 1.5-T scanner using the standard knee protocol at our institution (Figure 2). While our research is retrospective in nature and we could not standardize the positioning of patients’ legs during the MRI examination, our hospital’s radiology department adheres to a strict standardized protocol. All radiological procedures are rigorously followed. Any deviations from the standard are promptly corrected during the procedure, or the examination is repeated appropriately. Thus, this potential variance has minimal effect on our study outcomes. All the imaging studies were independently and retrospectively reviewed by 2 board-certified musculoskeletal radiologists (Y.F. and J.G.), one with 8 years of clinical experience and the other with 5 years of clinical experience. To ensure maximal objectivity in our findings, the 2 evaluators were blinded to the patients’ medical histories, physical examinations, diagnoses, and the study's overarching aim. Only fat-suppressed T2-weighted coronal and sagittal images were reviewed to determine the location of bone contusion. The sequence specifics for the images were as follows: a mean repetition time of 4000 ms, echo time of 70 ms, field of view of 16 cm, matrix size of 256 × 256 for display, number of excitations of 2, slice thickness of 4 mm, and interslice gap of 0.4 mm.
Assessment of Bone Contusion
The size and location of contusions were recorded using the MOAKS system for evaluating bone marrow lesions. 19 The MOAKS is a comprehensive system for assessing the whole knee joint in osteoarthritis semi-quantitatively, which refines the scoring of bone marrow lesions (BMLs), cartilage, and the elements of meniscal morphology scoring. 19 Because bone contusions demonstrate decreased signal intensity on proton-density or T1-weighted images and increased signal intensity on T2-weighted images, which is the same as BML, the MOAKS system can also be used to provide regional delineation and scoring across regions for semi-quantitative assessment of bone contusion in patients.19,43 The femur is divided into 6 subregions, and the tibia is divided into 3 subregions (Figure 3). The percentage of the volume of each BML is graded on a 2-dimensional (2D) MR slice. Multiple BMLs can occur within each subregion, and each subregion is assigned a single size grade that accounts for the total extent of all BMLs present in that subregion. The MOAKS grades are as follows: grade 0 = none; grade 1 <33%; grade 2 = 33%-66%; and grade 3 >66%. Compared with the original Whole-Organ Magnetic Resonance Imaging Score standards, MOAKS modifies the thresholds for BML size and develops grades that are more specific.19,51 Patients were grouped according to the number of combined bone contusions (0-5) present on MRI, as well as the location of the contusions, which is presented in Figure 4.
Data Analysis
The mean number of days between injury and MRI acquirement was compared across the groups with different amounts of contusions using a single-factor analysis of variance. Sex differences in contusion location, as defined by the MOAKS system, were analyzed using the χ2 test, and the Fisher exact test was employed when necessary in cases involving a small sample size. We also examined sex differences in the volume of each BML, graded according to the MOAKS system, using an independent sample t test. Heat maps (Figure 5) and 3D models (Figure 6) were used to present the distribution of bone contusions in a more intuitive manner.
Inter- and intrarater intraclass correlation coefficient (ICC) agreements were calculated for the location and number of bone contusions (Appendix Table A2). Agreement was defined as poor, moderate, good, or excellent reliability (<0.5, 0.5-0.75, 0.75-0.9, and >.0.9), respectively. 29 After the ICCs were calculated, if there was any disagreement between the presence or absence of bone bruises and/or the location of the bone bruises, the 2 radiologists rereviewed the cases together until a consensus was reached to make a final determination. All statistical analyses were performed using SPSS Software Version 25.0 (IBM Corp). Statistical significance was set at P < .05.
Results
From 2009 to 2021, a total of 1045 PCL tears (745 male and 300 female patients) were recorded, and 973 tears were excluded based on our exclusion criteria (Figure 1). The remaining 72 patients (6.89% of those screened) met the inclusion criteria, comprising 55 men (mean age, 39.03 ± 14.22 years [range, 12-58 years]) and 17 women (mean age, 36.11 ± 13.88 years [range, 17-52 years]). No significant difference was observed in age between male and female patients (P = .128). The patients’ characteristics are given in Table 1.

Flowchart of patient selection. ACL, anterior cruciate ligament; LCL, lateral collateral ligament; MCL, medial collateral ligament; OA, osteoarthritis; PCL, posterior cruciate ligament; PT, patella tendon.
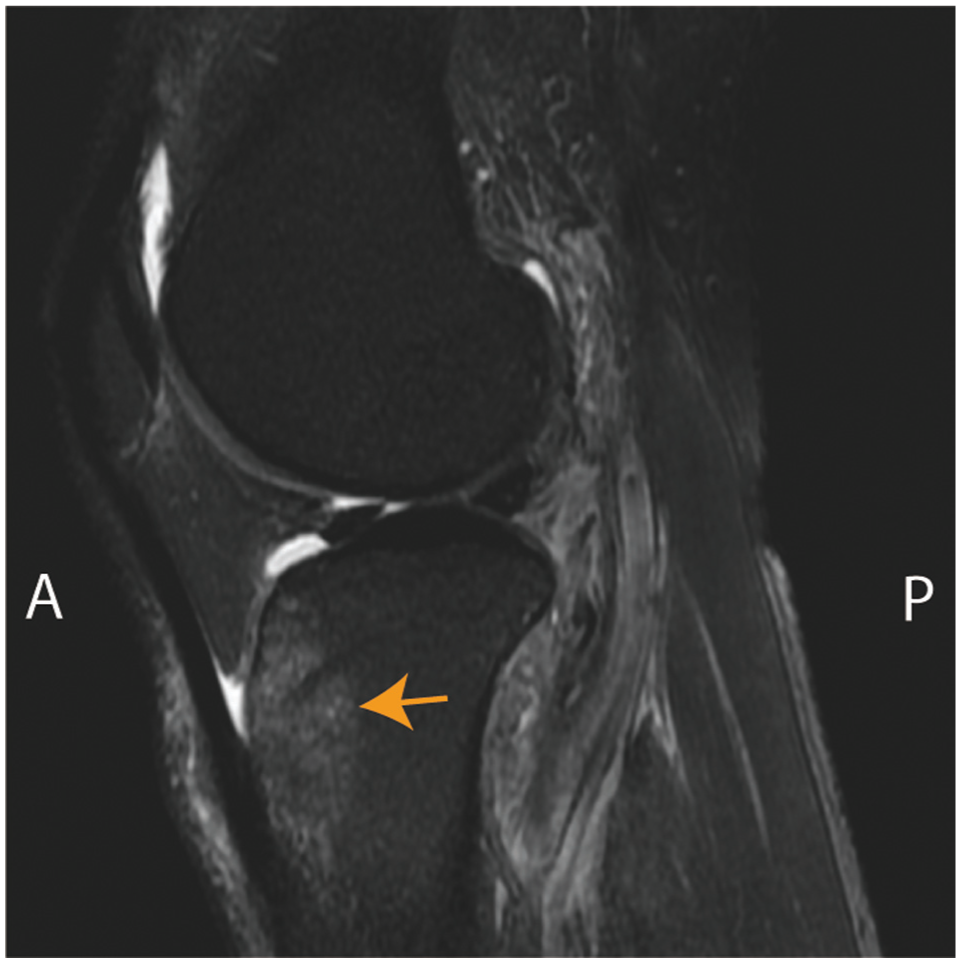
Representative T2-weighted MRI scan from a patient with the most classic PCL rupture contusions pattern, showing contusions (arrow) in the front of the tibia. MRI, magnetic resonance imaging; PCL, posterior cruciate ligament.
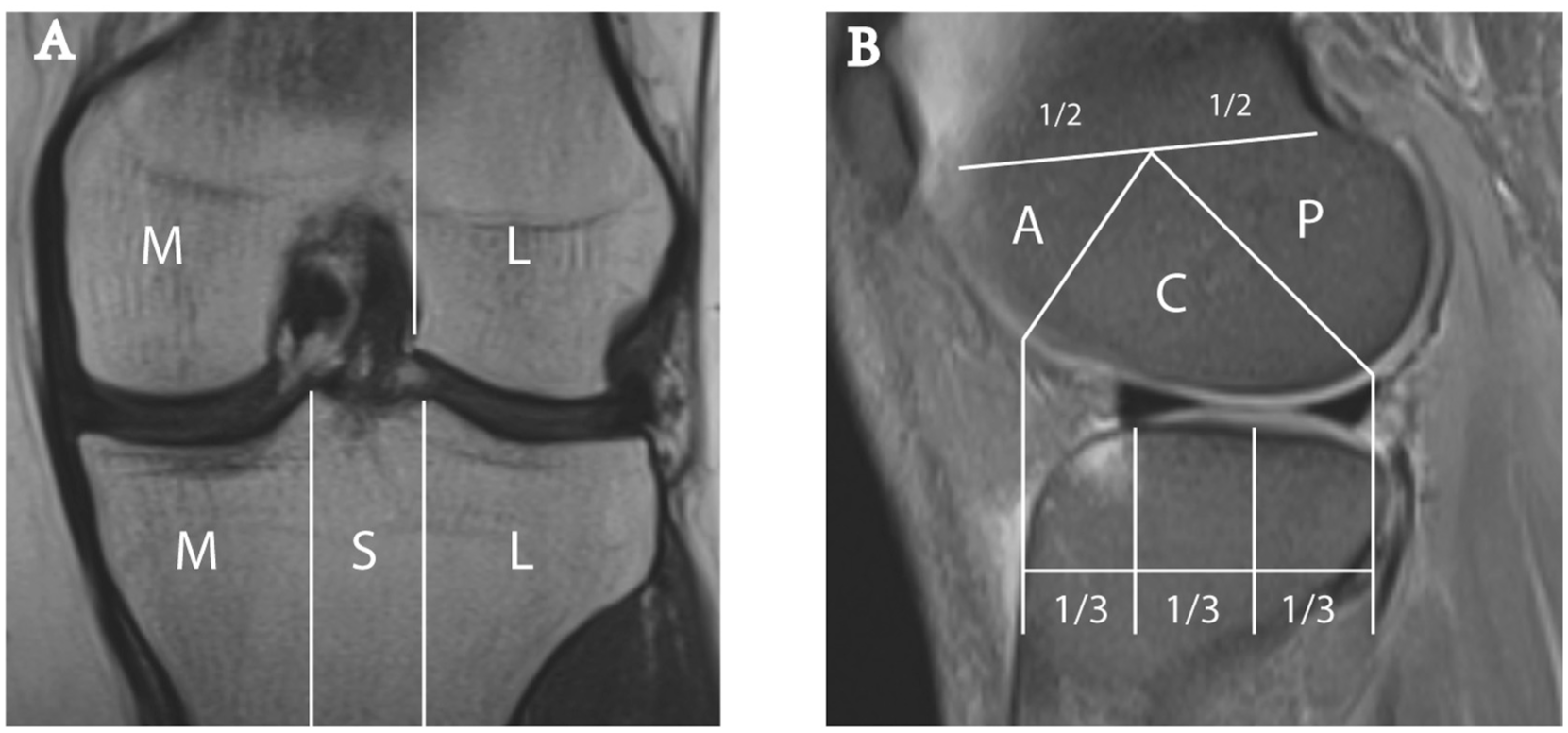
Anatomic delineation based on the MOAKS system. (A) The coronal image demonstrates the anatomic division of the tibia into 3 subregions: medial (M), subspinous (S), and lateral (L). Similarly, the femur is segmented into the medial (M) and lateral (L) femoral condyles, with the intercondylar notch classified as part of the medial femur. (B) The sagittal projection illustrates the anatomic segmentation of the femur into anterior (A), central (C), and posterior (P) regions. This division mirrors that of the tibia, which is partitioned into equal thirds along its length. MOAKS, MRI Osteoarthritis Knee Score.
Patient Characteristics (N = 72) a

Data are presented as mean ± SD and n (%). “+” indicates involvement of at least 1 compartment in the corresponding combined injury; “–” indicates no involvement. LFC, lateral femoral condyle; LTP, lateral tibial plateau; MFC, medial femoral condyle; MTP, medial tibial plateau; SS, subspinous subregion.
The frequency and pattern of bone contusions, categorized by compartment, are shown in Figure 4. Of the 72 patients, 13 patients had no contusion, and in the remaining patients with contusions, the most common types of each kind of combined contusion are as follow: LTP for only 1 bone contusion compartment (4 of 11; 36.4%), LFC + MFC/LFC + SS/LTP + SS (3 of 15; 20%) for 2 compartments, MFC + LTP + SS (5 of 17; 26.1%) for 3 compartments, MFC + LTP + SS + MTP/LFC + MFC + SS + MTP/LFC + MFC + SS + MTP (4 of 13; 30.8%) for 4 compartments, and 3 patients (4.2%) had contusions in all 5 compartments. We found that LFC had a higher incidence of bone contusion, which is uniformly highlighted in all patterns of bone contusion containing LFC, as shown in Figure 4. The other 4 compartments are all represented in Appendix Table A2, respectively, in the same way.

Frequency of bone contusion patterns by number of contusions. Patterns are also grouped by the number of contusions (bruises). Percentages may not sum to 100 due to rounding. LFC lateral femoral condyle; LTP, lateral tibial plateau; MFC, medial femoral condyle; MTP, medial tibial plateau; SS, subspinous subregion.
We did not detect significant differences in the time between PCL injury and MRI acquirement among the 0- to 5-bone contusion groups, with a mean of 7.11 ± 7.63 days for the 0-contusion group, 5.09 ± 6.31 days for the 1-contusion group, 4.75 ± 6.54 days for the 2-contusions group, 9.25 ± 9.45 days for the 3-contusions group, 5.53 ± 7.89 days for the 4-contusions group, and 5.90 ± 8.79 days for the 5-contusions group (Appendix Table A1).
The frequencies of contusions in male and female patients are reported in Table 2. Some significant differences were noted in the frequencies between male and female patients—including posterior LTP (9.1% vs 23.5%; P = .024), anterior LFC (12.7% vs 5.9%; P = .017), posterior LFC (29.1% vs 41.2%; P = .006), total MFC (47.3% vs 58.8%; P = .019), and posterior SS (3.6% vs 23.5%; P = .039). The differences in volume of each BML between male and female patients are presented in Table 3. We observed a significant difference in posterior LTP (0.137 ± 0.4508 vs 0.413 ± 0.8070; P = .040), with female patients scoring higher than male patients.
Contusion Frequency by Compartment and Sex a
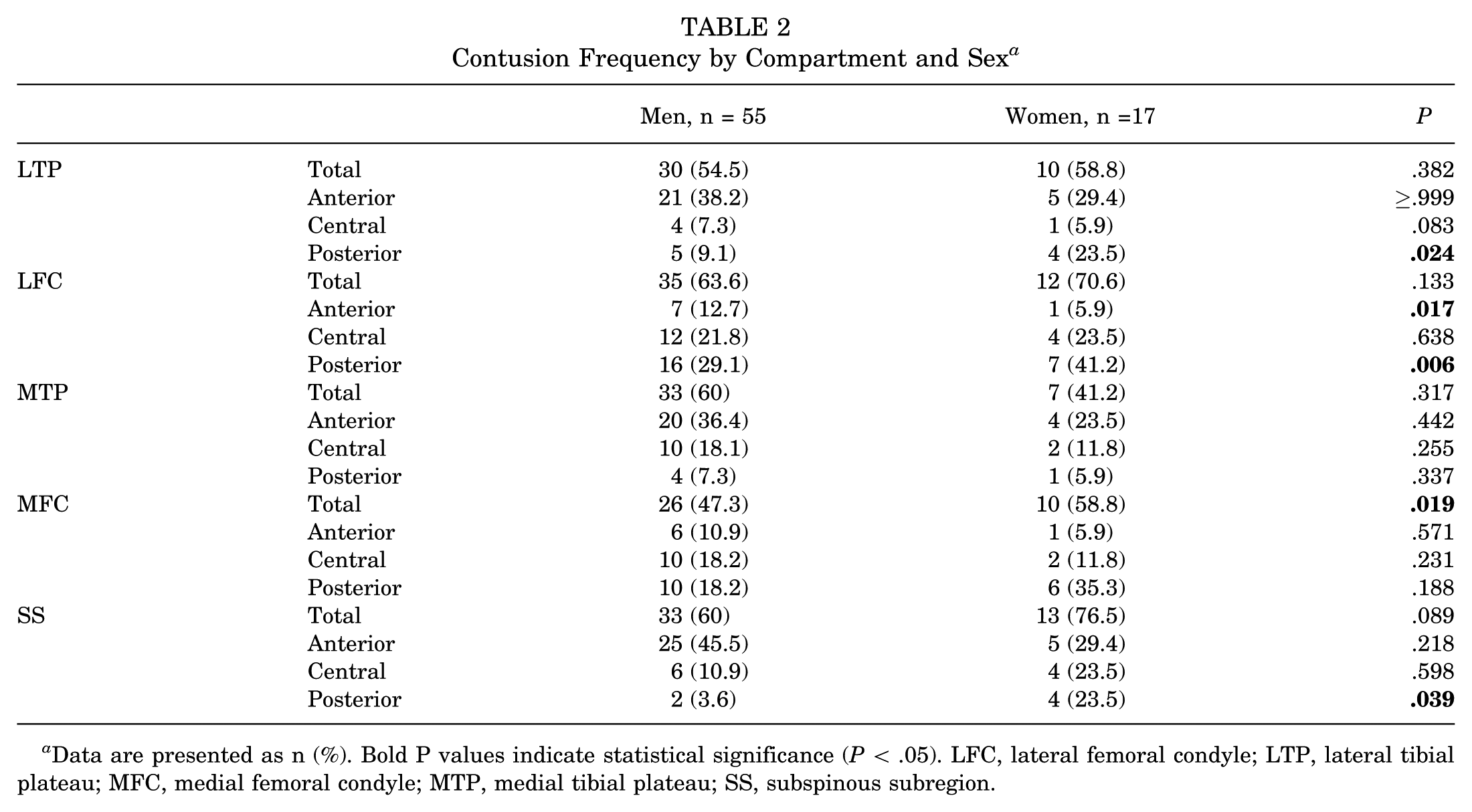
Data are presented as n (%). Bold P values indicate statistical significance (P < .05). LFC, lateral femoral condyle; LTP, lateral tibial plateau; MFC, medial femoral condyle; MTP, medial tibial plateau; SS, subspinous subregion.
Sex Differences in the Volume of Each BML Graded by the MOAKS System a
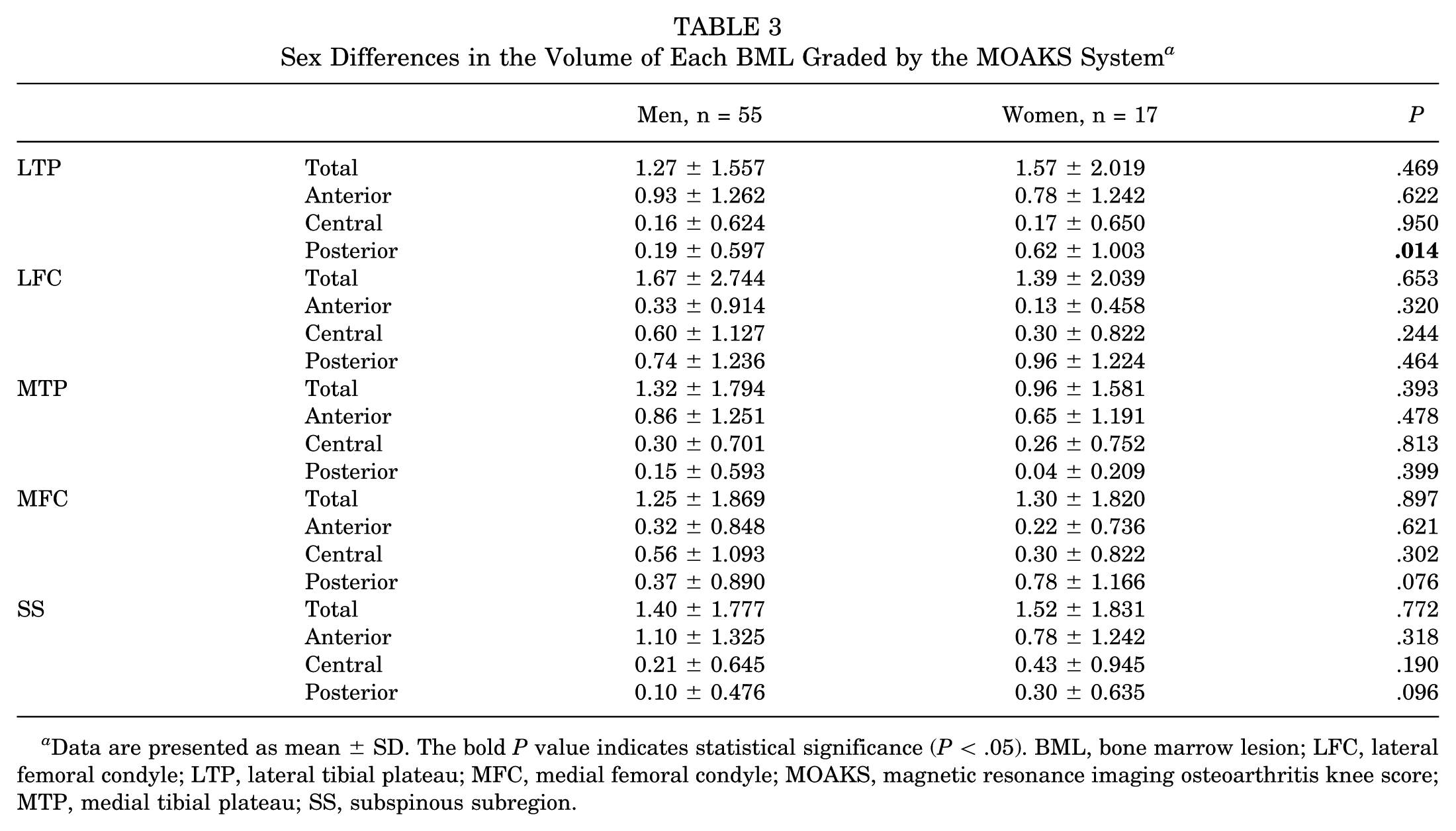
Data are presented as mean ± SD. The bold P value indicates statistical significance (P < .05). BML, bone marrow lesion; LFC, lateral femoral condyle; LTP, lateral tibial plateau; MFC, medial femoral condyle; MOAKS, magnetic resonance imaging osteoarthritis knee score; MTP, medial tibial plateau; SS, subspinous subregion.
The sex differences in the volume of each BML are shown in Table 3. No significant differences were observed between male and female patients in any compartment except for the posterior LTP (0.19 ± 0.597 vs 0.62 ± 1.003; P = .014).
The frequency and distribution of bone contusion patterns are presented in the form of a heat map in Figure 5. Posterior LFC (23; 31.9%), anterior LTP (26; 36.1%), anterior SS (30; 41.7%), and anterior MTP (24; 33.3%) occurred at high frequency. To visualize the distribution pattern of bone contusions associated with PCL rupture, a 3D model of the knee joint was also created and combined with the bone contusion frequency and volume data for each compartment (Figure 6).

Heat map of frequency and distribution for bone contusion patterns. We calculated the frequency of bone contusions (ie, the number of patients with bone contusions in a single region as a proportion of the study population) for each region of the femoral and tibial articular surface according to the regional division of the MOAKS system. These were displayed based on whether they occurred at high (red) or low (blue) frequency. We interpret the grade of frequency of bone contusion patterns in a single distribution based on the definition using data obtained from summary statistics by ourselves (>0.3, high frequency; 0.2-0.3, moderate frequency; and <0.2, low frequency). MOAKS, MRI Osteoarthritis Knee Score.

Microscopic principles and bone contusion distribution associated with isolated PCL rupture. (A) Bone contusion, often accompanied by ACL and PCL rupture, is microscopically mainly manifested as collapse of trabecular bone as well as hemorrhage and edema of subchondral bone. (B) The distribution of bone contusion on the articular surface of the femur and tibia was based on the divisions of the MOAKS system in this study. (C) Frequency of bone contusion in each compartment of the articular surface of the femur and tibia. MOAKS, MRI Osteoarthritis Knee Score.
Intrarater and interrater reliability, assessed using ICCs, showed at least good levels of agreement across all measures (Appendix Table A2).
Discussion
In this study, we found that in patients with isolated PCL rupture, bone contusions are commonly observed in the anterior SS, anterior LTP, anterior MTP, and posterior LFC. Additionally, female sex is identified as an associated factor contributing to the presence of bone contusions. Numerous studies have observed that bone contusion frequently accompanies PCL rupture, but there exists a significant shortfall in the realm of targeted, systematic research specifically focusing on bone contusion associated with PCL rupture.13,50,56,58,59,61 Mair et al 33 were the first to examine bone contusion distribution in patients with PCL rupture; however, that study also included patients with combined MCL and LCL injuries and cartilage injuries, which may change the distribution of bone contusion and influence the elucidation of the mechanism of PCL rupture. We utilized the MOAKS system, an MRI-based semi-quantitative assessment method, to evaluate the distribution of bone contusions in patients with isolated PCL rupture, excluding other ligament injuries and fractures, within 4 weeks of injury for the first time. Our study observed a high incidence of bone contusion on the posterior LFC.
Bone contusions, often from impingement, are potential indicators of injury mechanisms (Figure 7). 57 The high-frequency bone contusion regions we observed were consistent with previous studies, such as the work by Kannus et al, 20 which ascertained that a dashboard injury, the predominant mechanism of PCL injury, occurs when the knee is flexed and significant force is directed at the anterior aspect of the proximal tibia. Concurrently, bone contusions can manifest on the tibia’s anterior surface and occasionally on the patella’s posterior aspect. 56 Thus, it is consistent with our findings that the anterior regions of the tibia, specifically the anterior LTP, anterior SS, and anterior MTP, exhibited high contusion frequencies. 57 Intriguingly, the posterior LFC was the sole region on the femur’s articular surface with high contusion frequency. This observation suggests a possible pivotal mechanism underlying PCL injuries. Beyond the relative posterior displacement of the flexed tibia, external rotation and valgus alignment of the knee joint may be contributory during PCL injury. The pattern of bone contusion in the LFC is commonly linked with pivot-shift or multiplanar, valgus-loading injury mechanisms.15,56 Anatomic and biomechanical studies have shown that the PCL consists of 2 bundles—the anterolateral and posteromedial.1,61 The PCL attaches to the lateral aspect of the medial femoral condyle,1,2,14,60 and the tibia between the medial plateau and lateral condyle, just distal to the articular surface.2,14,31,42,47,60 The PCL runs anteromedial to posterolateral in the joint, and with posterior tibial displacement after impact, force is transmitted through the PCL, producing an outward and posterior force, resulting in external tibial rotation. 63

The biomechanical mechanism of PCL rupture and the corresponding bone contusion location are preliminarily speculated in this study. PCL, posterior cruciate ligament.
Kaplan et al 21 proposed a contrecoup mechanism in ACL injuries, in which bone contusions result from a rebound impact as the subluxated knee reduces after high-energy trauma. Based on this concept, we propose a novel hypothesis for PCL injuries: the posteriorly subluxated tibia may similarly undergo a rebound injury during spontaneous reduction, contributing to the high frequency of bone contusions observed in the posterior LFC. This may be particularly relevant in PCL-injured knees that have concomitant varus alignment and relative external rotation of the proximal tibia, which may predispose the posterior LFC to focal impact. Additionally, previous studies have reported a high incidence of concomitant injuries to the posterolateral complex (PLC) structures in patients with PCL rupture.52,57 Given the anatomic proximity of the PLC to the posterior LFC, such associated injuries may further explain the increased prevalence of bone contusions in this region.
We also observed sex differences in the distribution of bone contusions and drew an initial conclusion that the proportion of female patients with bone contusions is higher than that of male patients in several compartments, with significant differences. In general, the differences in bone contusion patterns between male and female patients may be due to several factors—including osseous, neurological, mechanical, movement pattern, and bone mineral density. Growing evidence has shown that poor or abnormal lower limb biomechanics—particularly neuromuscular control of the core—are underlying factors contributing to the higher incidence of knee injuries in women compared with men.16,17,30,36,37 Previous studies have demonstrated that the quadriceps muscle plays a protective role for the PCL by exerting an anteriorly directed force on the tibia, thereby reducing posterior tibial translation.12,35 In our subsequent investigation, we observed that female patients exhibit lower levels of quadriceps muscle activation, strength, endurance, and neuromuscular control compared with male patients.3,24,38,41,45 These differences likely result in greater relative tibial displacement during knee injuries in female patients, leading to more pronounced bone contusions. Popp et al 53 also found that the total volumetric bone mineral density, trabecular thickness, and cortical area and thickness are significantly higher in male patients than in female patients. These findings suggest that female patients are more prone to the collapse of trabecular bone, as well as hemorrhage and edema of the subchondral bone during impact, which may result in more pronounced bone contusions. This could also explain why we observed larger BML volumes in female patients at several locations.
Given that bone contusions may result in prolonged pain and dysfunction, early recognition of typical contusion patterns could improve diagnostic accuracy and inform clinical decision-making. Tailoring management strategies to these biomechanical and patient-specific risk factors may ultimately improve patient prognosis and optimize long-term functional outcomes. In female patients, early initiation of quadriceps strengthening, proprioceptive training, and the use of knee braces or other orthotic supports may enhance knee joint stability and mitigate the risk of PCL injury.7,32,49 For athletes, sport-specific neuromuscular training focused on technique and alignment during knee-flexion activities—such as squatting and jumping—may help maintain proper biomechanics and reduce posterior tibial stress during high-demand movements. 11 Additionally, targeted stretching and soft tissue mobilization of the gastrocnemius muscle may help decrease excessive muscle tension and prevent compensatory overactivity, which could otherwise contribute to altered knee mechanics.10,44
There are several limitations and potential criticisms of our study: (1) We did not classify the causes of PCL injuries, such as sports injuries or trauma, which may also affect the mechanistic explanation. (2) Due to the uneven sex distribution of PCL injury itself, there are far more men than women in our study, and sex itself is also an influencing factor of bone contusion. (3) We did not perform an MRI immediately after injury, and the interval may have biased our results of bone contusion from those at the time of injury. However, we analyzed the time from injury to MRI separately for patients with different numbers of combined contusions, and there was no significant difference between the groups; thus, this study was not affected (Appendix Table A1). (4) PLC has a combined injury relationship with approximately 60% PCL rupture.52,57 However, due to the high rate of misdiagnosis and missed diagnosis of PLC injury on MRI (50%-76%), we did not include PLC in this study.26,40,48,55 (5) This retrospective study was limited by the inability to standardize patient leg positioning during MRI examinations, which may have introduced potential bias into the final statistical measurements. (6) In this study, only the MOAKS system, a semi-quantitative method, was used to assess bone contusion, and more advanced imaging processing methods, such as image analysis of machines and region of interest, were lacking.
Conclusion
In patients with isolated PCL injury, bone contusion often occurred in the anterior subspinous subregion, anterior lateral tibial plateau, anterior medial tibial plateau, and posterior lateral femoral condyle. Female patients demonstrated a greater prevalence and extent of bone contusions relative to their male counterparts.
Footnotes
Appendix
Interrater and Intrarater ICC Agreements for Each Compartment a

| Interrater ICC | Intrarater ICC | ||
|---|---|---|---|
| LTP | Total | 0.872 | 0.881 |
| Anterior | 0.926 | 0.716 | |
| Central | 0.823 | 0.840 | |
| Posterior | 0.870 | 0.961 | |
| LFC | Total | 0.766 | 0.703 |
| Anterior | 0.932 | 0.755 | |
| Central | 0.711 | 0.912 | |
| Posterior | 0.802 | 0.831 | |
| MTP | Total | 0.744 | 0.804 |
| Anterior | 0.759 | 0.973 | |
| Central | 0.971 | 0.909 | |
| Posterior | 0.827 | 0.891 | |
| MFC | Total | 0.911 | 0.833 |
| Anterior | 0.906 | 0.764 | |
| Central | 0.837 | 0.979 | |
| Posterior | 0.881 | 0.800 | |
| SS | Total | 0.795 | 0.931 |
| Anterior | 0.910 | 0.884 | |
| Central | 0.744 | 0.799 | |
| Posterior | 0.861 | 0.851 |
Agreement was defined as poor, moderate, good, or excellent reliability: <0.5, 0.5-0.75, 0.75-0.9, and >0.9, respectively. ICC, intraclass correlation coefficient; LFC, lateral femoral condyle; LTP, lateral tibial plateau; MFC, medial femoral condyle; MTP, medial tibial plateau; SS, subspinous subregion.
Final revision submitted May 15, 2025; accepted June 9, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The Second Affiliated Hospital, School of Medicine, Zhejiang University (IR2022546).