
Abstract
Background:
The adequate preservation of the anterior cruciate ligament (ACL) remnant at the time of ACLR (ACLR) may improve postoperative clinical outcomes.
Purpose:
To determine the optimal time to perform remnant-preserving ACLR relative to ACL injury and, to this end, to evaluate the condition of the ACL remnant retrospectively at different time points after injury.
Study Design:
Cross-sectional study. Level of evidence 3.
Methods:
Our study cohort comprised 205 patients who underwent ACLR. The patients were divided into 6 groups according to the time between injury and assessment in 2-week intervals up to 12 weeks. Based on their location and volume of the ACL remnant on arthroscopic images, the remnants were classified as follows using the modified Crain criteria: type 1, scarring to the posterior cruciate ligament; type 2, remnant attached to the notch; type 3, remnant attached to the femoral wall; type 4, resorption of the remnant; and type 5, remnant frayed like a mop end.
Results:
The time after injury significantly correlated with the remnant tissue condition (P < .0001). Residual analysis revealed that Type 5 remnants were most common (P < .0001) and type 3 remnants were the least common (P < .0001) at 0 to 2 weeks after injury. Type 3A, 3B and 3C remnants were most common at 2 to 4 weeks after injury (P < .0001, P < .0001, and P = .0002, respectively).
Conclusion:
Adequate remnant tissue (type 3) remained in the subacute phase (2 to 4 weeks) after ACL injury, whereas complete rupture of the remnant (type 4) was observed in the acute phase (0 to 2 weeks).
Anterior cruciate ligament (ACL) injuries are among the most prevalent and challenging musculoskeletal conditions faced by orthopaedic surgeons today.7,17 The surgical options with better outcomes for ACL injuries include remnant-preserving ACL reconstruction (ACLR). Although remnant-preserving ACLR has been associated with complications such as the development of cyclops lesions and inaccuracies in tibial tunnel positioning,1,19,25 recent studies have reported that these complications are not necessarily related to remnant-preserving ACLR.6,11 Therefore, this widely described procedure helps restore mechanical stability; promotes the biological healing of ACL grafts, blood vessels, and mechanoreceptors; provides better knee functional outcomes; and resists the bone tunnel enlargement than does nonremnant-preserving ACLR.3,5,17,22,24,25,29,30,31
The remnant volume of the ACL correlates with the postoperative outcome in terms of objective stability and subjective recovery.10,16 In a recent study, adequate remnant preservation during ACLR improved second-look graft appearance and patient-reported outcome scores. 20 Therefore, remnant-preserving ACLR appears to be a reasonable strategy. When performing this surgery, maintaining the connectivity of the ACL remnant from the femoral to the tibial side is important for preserving the mechanoreceptors and blood vessels in the ruptured ACL. 14
In a previous study, the timing of ACLR after ACL injury was earlier in patients with versus without adequately preserved remnants. 20 However, the optimum time for ACLR remains unclear because few studies have addressed this issue. The presence of a significant amount of remnant tissue in the early phase after ACL injury is considered likely.
We hypothesized that a large volume of intact remnant tissue in the injured ACL would persist for several weeks after the injury. The primary goal of this study was to clarify how the condition of the remnant varies depending on the time after injury. Such knowledge would provide valuable insights into the optimal timing for remnant-preserving ACLR.
Methods
Study Design
This retrospective cohort study enrolled 277 consecutive patients (aged 15-50 years) with an ACL-deficient knee who underwent anatomic double-bundle ACLR at our hospital between March 2012 and July 2020. The reconstruction was performed using 2 hamstring tendon autografts with or without remnant tissue preservation.
The inclusion criterion for the study was an isolated ACL injury treated via double-bundle ACLR within 12 weeks of injury. The exclusion criteria were an injury in a knee ligament in addition to the ACL, a previous knee operation, no arthroscopic data for remnant assessment, and an unknown date of injury. The study design was approved by the institutional review board of our hospital before its commencement (Trial No. 19-00469).
Of the 277 patients enrolled in this study (Figure 1), a total of 72 were excluded because of insufficient data (n = 32), previous revision surgery (n = 15), previous multiligament surgery (n = 6), and unknown date of injury (n = 19). The remaining 205 patients were divided into 6 groups according to the time after injury to remnant assessment: 0-2, 2-4, 4-6, 6-8, 8-10, and 10-12 weeks. Preoperative side-to-side anterior laxity was measured using a KT-2000 arthrometer (Medmetric Corp) on the day before surgery.

Study flowchart. ACL, anterior cruciate ligament.
Surgical Procedure and Evaluation of Remnant Tissue
Surgical reconstruction was performed by 1 board-certified surgeon (M.I.) with at least 20 years of experience. Before ACLR, the condition of the remnant tissue was meticulously observed and recorded via arthroscopy. ACLR was performed as described by Kondo et al. 10
Using arthroscopic images, recorded videos, surgical records, and the modified Crain classification as a reference, 4 the remnant tissue was divided into 5 types according to its location and condition (Figures 2 and 3). In type 1 cases, scarring of the posterior cruciate ligament (PCL) was observed (The Crain classification: group 1), and the ACL fibers were retracted and matted down to the PCL. In type 2 cases, the remnant remained attached to the roof of the notch (The Crain classification: group 2), and the ACL disruption had healed. In type 3 cases, we further divided them into 3 patterns depending on the attachment site and the volume of the remnant. In other words, the remnants of the anteromedial (AM) and posterolateral (PL) bundles were attached to the femoral wall in 3 distinct patterns: type 3A, in which the remnant was attached to the anatomic site in the distal femur, anterior laxity was noticeable, and ≥50% of the injured ACL remained; type 3B, in which the remnant remained at the anatomic site of the AM bundle, and the PL bundle was partially detached from the distal femur; and type 3C, in which the remnant was attached to a nonanatomic site anterior, and distal to the AM and PL bundle footprints, or ≤50% of the injured ACL remained. Type 3A and 3B patterns indicated an adequate remnant condition. In type 4 cases, the remnants were not observed (The Crain classification: group 4). In type 5 cases, the ruptured ACL had a discontinuous appearance resembling frayed mop ends.
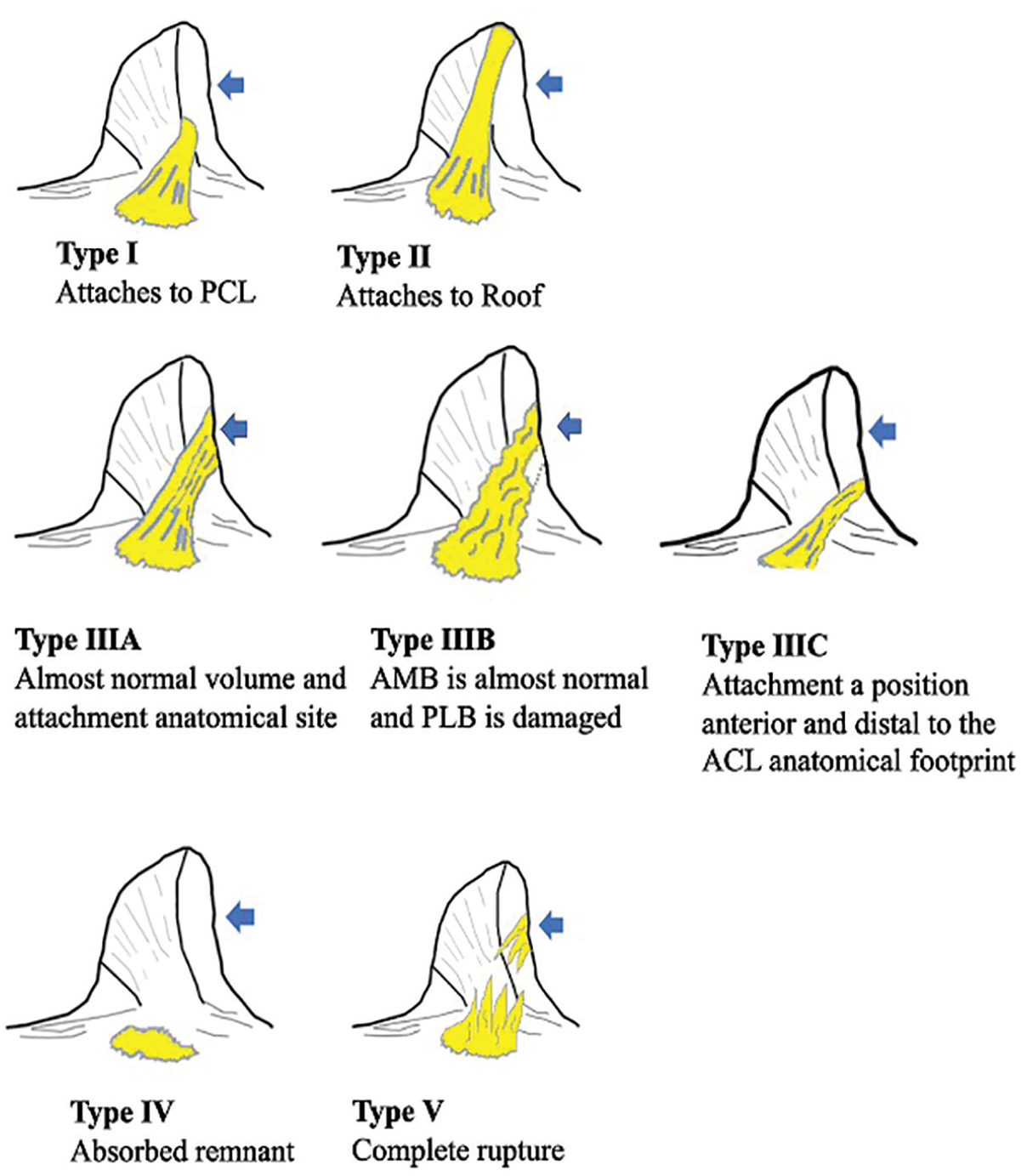
The modified Crain classification. Type 1: scarring of the PCL. Type 2: remnant attached to the roof of the notch. Type 3A: large amount of remnant attached to the anatomic site of the AM and PL bundles, with an apparent anterior laxity. Type 3B: large amount of remnant attached to the anatomic site of the AM bundle, with detachment of the PL bundle. Types 3A and 3B indicate adequate remnant preservation. Type 3C: remnant attached to the nonanatomic site of the AM and PL bundles, or ≤50% of the remnant remains. Type 4: remnant absent at the femoral wall. Type 5: ruptured ACL has discontinuous appearance resembling frayed mop ends. The blue arrows indicate the attachment of the ACL to the lateral femoral condyle. ACL, anterior cruciate ligament; AM, anteromedial; PL, posterolateral; PCL, posterior cruciate ligament.

Arthroscopic images taken during ACLR. (A) The remnant is attached to the anatomic site of the AM and PL bundles (type 3A). (B) The remnant is attached to the anatomic site of the AM bundle and partially detached from the PL bundle (type 3B). (C) The remnant is ruptured and has a discontinuous appearance resembling frayed mop ends (type 5). ACLR, anterior cruciate ligament reconstruction; AM, anteromedial bundle; PL, posterolateral.
Reproducibility of Remnant Classification
Two experienced orthopaedic surgeons (D.S. and M.I.), who were blinded to all descriptive data, acted as observers and independently scored the ACL remnant set of arthroscopic images and videos. Interreader reliability was evaluated by comparing the scores of the 2 observers. To evaluate intrareader consistency, one of the observers (D.S.) was asked to score the remnant at least 4 weeks after the initial assessment.
Statistical Analysis
All data are presented as the mean ± standard deviation. The Kolmogorov-Smirnov test was used to check the normality of the data. Within-group comparisons were performed using 1-way analysis of variance, with the Fisher least significant difference test for post-hoc multiple comparisons of ordinal categorical variables. The Pearson chi-square test was used to analyze nominal categorical data. Weighted κ-values were used to categorize the condition of the remnant tissue. According to Landis and Koch, 12 the Kappa values were scored as follows: 0, poor agreement; 0-0.20, slight agreement; 0.21-0.40, agreement; 0.41-0.60, moderate agreement; 0.61-0.80, substantial agreement; and 0.81-1, almost perfect agreement. Commercially available software programs (GraphPad Version 10, GraphPad Software; JMP Version 14, SAS Institute Inc) were used for statistical calculations. The significance level was set at P < .05.
Results
Patient Characteristics
A total of 205 patients (112 men and 93 women), with a mean age of 31.8 years (range, 15-50 years), were registered for evaluation. The mean age, body mass index (BMI), and preoperative side-to-side anterior laxity measured using a KT-2000 arthrometer are shown in Table 1. There were no significant differences in the arthroscopic intra-articular treatments among the 6 groups. The medial and lateral menisci were injured in 105 patients (Table 2). No cartilage injuries requiring surgery occurred.
Baseline Characteristics of the Patients a

The data for age, BMI, and anterior laxity are presented as mean ± SD. P values were determined using 1-way analysis of variance. BMI, body mass index.
Types of Injuries a

Data are presented as n (%). P values were determined using the chi-square test. PF, patella femoral.
Relationship Between Time After Injury and Remnant Tissue Classification
There were significant differences between the time after injury and the condition of the remnant tissue (P < .0001) as determined via residual analysis (Figure 4). Type 5 remnants were most common in the 0-2 week group (P < .0001), type 3A to 3C remnants in the 2-4 week group (P < .0001, P < .0001, and P = .0002, respectively), type 4 remnants in the 8-10 week group (P = .004), and type 1 remnants in the 10-12 week group (P = .038). The second most common occurrence of type 3A to 3C remnants was in the 2-4 week group (P < .0001, P = .013, and P = .042, respectively). Types 3A and 3B were the least common in the 0-2 week group (P < .0001 and P = .0054, respectively) and the 10-12 week group (P < .0001 and P = .027, respectively), and types 4 and 5 were the least common in the 2-4 week group (P = .039 and P = .043, respectively).

The distribution of the remnant types according to the time of assessment after injury. The number and percentage of each remnant type (1-5) are shown in panels A and B, respectively. There were significant differences between the time after injury and the condition of the remnant tissue (P < .0001).
Reproducibility of Remnant Classification
The weighted Cohen Kappa values were calculated for each score separately. The values for inter-reader and intrareader agreement on remnant type were 0.9185 and 0.8890, respectively, indicating almost perfect agreement.
Discussion
The most important finding of this study is that the condition of the ACL remnant varies depending on the time after ACL injury. Contrary to our hypothesis, the completely ruptured remnant pattern (type 5) was observed in 0 to 2 weeks after injury, whereas a more favorable type (type 3A and 3B) was observed at 2 to 4 weeks. These findings offer valuable insights into the optimal timing of remnant-preserving ACLR relative to ACL injury and have potential implications for surgical outcomes and rehabilitation.
Biological responses within the knee after ACL injury could account for the observed variations in remnant condition. For example, injury-induced inflammatory responses may worsen the condition of the remnant in the acute phase (within 2 weeks after injury). During this phase, there may be extensive swelling, hemorrhage, and inflammation within the knee joint, which could compromise the integrity and viability of the ACL remnant. 8 After this phase, while scar tissue forms, some of the remnant tissue may undergo biological changes that potentially enhance its capacity for preservation. Preservation-enhancing events include the initiation of the proliferative phase of tissue healing at 2 to 4 weeks after injury, as well as the synthesis of collagen and formation of granulation tissue, which may contribute to the stabilization of torn ACL remnants. 15 These trends suggest that the incidence of ruptured ACL remnants will decrease and that of continuous remnant tissue will increase 2 weeks after injury. Minimal acute inflammation in the joint may allow for better evaluation and handling of the remnant tissue during surgery.
The above findings have significant clinical implications in terms of the timing of remnant-preserving ACLR. Given the favorable condition of the remnant between 2 and 4 weeks after injury, surgical intervention during this period may be beneficial in terms of facilitating graft incorporation, improving revascularization, and preserving proprioception, all of which are crucial for restoring knee function. 18 Several studies have examined the ideal timing for ACLR to achieve favorable clinical outcomes. 27 These studies associated surgery within 8 days after injury with good functional performance, 27 surgeries within the 3 to 4 weeks after injury with improved clinical outcomes and stability,2,7 and surgery within 3 weeks after injury with high Tegner activity scores. 5 From the viewpoint of remnant-preserving ACLR, we reported that the condition of the remnant was better observed 2 to 4 weeks after ACL injury.
Remnant-preserving ACLR has been extensively documented; compared with no remnant-preserving ACLR, it restores mechanical stability better and promotes biological healing of ACL grafts, blood vessels, and mechanoreceptors, ultimately leading to better knee function.10,17,22,25 In a previous study, preserving anatomically positioned and adequate remnant tissue during double-bundle ACLR improved patient-reported outcome scores. 20 In the present study, the possibility of retaining continuous and adequate remnant tissue (type 3A and 3B) within 2 to 4 weeks after injury was significantly high. In addition, Van Keulen et al 26 reported the importance of continuous remnant preservation in remnant preservation ACLR surgery to obtain a lower clinical failure rate and ACL revision surgery rate compared with standard ACLR. 26 Consequently, we recommend performing remnant-preserving ACLR within this timeframe.
Regarding the effect of remnant-preserving ACLR on graft rupture, Webster et al 28 reported no significant association between graft rupture rates and remnant preservation. They showed that the percentage of graft rupture rate was 8.8% (20/228) in the no stump group, 5.8% (20/342) in the group of tibial stump preservation <50%, and 3.8% (3/88) in the group of tibial stump preservation >50%, respectively. Although there was no statistically significant difference, the graft rerupture rate tended to decrease in proportion to the amount of preserved remnant. In contrast to this study, which graded the tibial side of the preserved remnant, some authors have emphasized the importance of connecting the remnant from the femur to the tibia and applying tension to the remnant to achieve better clinical outcomes and stability during remnant-preserving ACLR.20,23,26 We believe that the maximum benefit from remnant-preserving ACLR can be achieved when the connected remnant, which maintains tension and blood supply on both the tibial and femoral sides, is preserved during surgery. By preserving an appropriate remnant in this manner, there is a potential to alter the relationship between graft rupture rates and remnant-preserving ACLR.
In the present study, type 1 and 2 remnants, as originally classified, were more frequently observed 10 weeks after injury than in the early phase. We speculate that this might be due to a combination of biological factors and individual behaviors after ACL injury. In the early phase, ruptured ACLs that have not remodeled are often observed; during this phase, patients find it difficult to engage in daily life activities because of knee pain, swelling, and inflammation. Subsequently, as the inflammation subsides, the ACL remnant tissue can begin remodeling. As a result, there might be some remnants that were connected to both the femur and the tibia. During the remodeling phase, in some cases, scar tissue may have formed and connected to the remnant tissue on the femoral wall, allowing the remnant tissue to potentially achieve continuity from the femur to the tibia. Such cases could be classified as type 3 remnants according to our classification. At this time, patients may begin walking and engaging in low-intensity activities. With increased activity levels, remnant tissue may be subjected to mechanical stress. Given its weaker resistance to mechanical forces compared with the ACL, the remnant tissue may detach from the lateral wall of the femur, depending on the nature and direction of the applied forces. Subsequently, it may reconnect to the PCL (The Crain classification group 1), the notch (The Crain classification group 2), or a nonanatomic site of the ACL (The Crain classification group 3).
Several studies have reported the outcomes of remnant-preserving ACLR, and most have adopted various methods for preserving remnant tissue. Using recorded videos, Kim et al 9 defined 4 remnant types based on morphological patterns. Remnants that had been preserved or partially detached at the femoral insertion during the creation of the femoral tunnel were categorized as follows: group A, remnant fully covered with synovium; group B, >50% synovial coverage; and group C, <50% synovial coverage. Lee et al 13 divided ACL remnants into 2 groups after comprehensively reviewing operative records and video recordings. A remnant volume of >20% was defined as group 1, and a remnant volume of <20% was defined as group 2. In group 2, the femoral side of the remnant tissue was not preserved. Shimodaira et al 21 reported that remnant preservation was achieved when the remnant was attached to the roof with sufficient thickness and >50% continuity. Suh et al 23 reported the utility of remnant preservation with tensioning in preventing the development of cyclops lesions and demonstrated better clinical outcomes in the remnant preservation with tensioning group compared with the control group. The Crain classification 4 is a well-known method of categorizing ACL remnants after injury. In the study by Crain et al, 4 the mean time between ACL injury and ACLR was 78 weeks. In more recent studies, this interval was significantly shorter; thus, directly applying the Crain classification to ACLR may be problematic.2,9,20,22 Furthermore, in the Crain classification, no type locates the remnant in the anatomic position of the ACL. Crain classification 3 is defined as the remnant being located on the medial wall of the lateral femoral condyle, not at the anatomic attachment. Practically, our previous study showed that the remnant was attached to the anatomic position of the wall of the femoral condyle. Therefore, Crain classification group 3 was divided into 3 groups. Verifying the effect of remnant-preserving ACLR on clinical outcomes is challenging because of the different remnant conditions and methods of preservation.
Limitations
Despite its several novel findings, our study has some limitations. First, because of the small number of patients in our study, we were unable to control for all potential confounding factors (eg, age, sex, BMI, and activity level). Therefore, studies with larger sample sizes are needed to confirm our findings and generalize them to a larger population. Second, the mechanisms underlying ACL injuries in our cohort were unknown. The condition of the ACL remnant tissue may vary depending on the forces applied to the knee at the time of injury. Third, the condition of the ACL remnant was evaluated retrospectively using arthroscopic images, mainly still images, and surgical records. Consequently, it was difficult to obtain quantitative data for the remnant tissue. Further research is needed to develop objective methods for accurately assessing remnant volume during surgery. Fourth, the relationship between remnant type and clinical outcome was not examined. However, some studies have reported that an adequate volume of remnant tissue could be related to clinical outcomes.16,20,21 Our future goal is to clarify the precise relationship between remnant condition and clinical outcomes. Before that, we proposed conducting this study to examine the remnant condition according to surgical timing for remnant-preserving ACLR. Fifth, the activity level of the patients between ACL injury and ACLR was unclear and may have affected the remnant pattern. To the best of our knowledge, the relationship between the level of sports activity and remnant type has not yet been clarified. Nevertheless, as previously mentioned, the activity level may have an influence; nonetheless, this has not been proven at this time. It is essential to acknowledge that individual variations in healing responses and the presence of other intra-articular injuries can affect decision-making regarding the timing of surgery. Therefore, further research with a larger number of cases and longer follow-up periods is needed to evaluate the clinical value of the morphological remnant condition.
Conclusion
Adequate remnant tissue (types 3A and 3B) remained in the subacute phase after ACL injury (2-4 weeks); however, the remnant was completely ruptured (type 5) in the acute phase (0-2 weeks). To maximize the advantages of remnant-preserving ACLR, performing this procedure during the subacute phase (2-4 weeks) is recommended. Our findings suggest a favorable context for remnant-preserving ACLR with potential benefits in graft integration and functional recovery.
Footnotes
Final revision submitted March 2, 2025; accepted March 11, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from NTT East Japan Sapporo Hospital.