
Abstract
Background:
The remnant preservation of a primary vertical graft in revision anterior cruciate ligament reconstruction (ACLR) can benefit anteroposterior stability. However, studies that address this concept are rare.
Purpose:
To evaluate clinical outcomes of remnant preservation of primary vertical graft in revision ACLR.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 74 patients with revision ACLR were included in this retrospective study. Remnant preservation revision ACLR was performed only in patients with primary vertical grafts. The patients were divided into 2 groups according to whether the primary remnant vertical graft was preserved (remnant group; n = 48) or absent or sacrificed (no-remnant group; n = 26). The remnant group was further divided according to the degree of remnant tissue: sufficiently preserved subgroup (graft coverage, ≥50%; n = 25) and insufficiently preserved subgroup (graft coverage, <50%; n = 23). Clinical outcomes were evaluated using the International Knee Documentation Committee (IKDC) subjective form, Lysholm score, Tegner activity scale, manual laxity tests, and side-to-side difference in anterior tibial translation on Telos stress radiographs.
Results:
The mean time to final follow-up was 40.7 ± 16.8 months. The remnant group showed more improved results in the postoperative Lachman test and Telos side-to-side difference than did the no-remnant group (P = .017 and .016, respectively). The post hoc test revealed that the side-to-side difference in laxity in the sufficiently preserved subgroup significantly outperformed that in the no-remnant group (P = .001), although no significant difference existed between the insufficiently preserved and no-remnant subgroups (P = .850). The postoperative IKDC subjective form, Lysholm score, and Tegner activity scale did not show significant differences between the 2 groups (P = .480, .277, and .883, respectively).
Conclusion:
The remnant preservation of the primary vertical graft in revision ACLR may result in better anteroposterior stability. However, subjective outcomes in the remnant group did not exceed that of the no-remnant group. The subgroup analysis revealed that only sufficiently preserved remnants demonstrated better anteroposterior stability.
There are various reasons for failed anterior cruciate ligament (ACL) reconstruction (ACLR). Except for new trauma, tunnel malposition is the primary cause of most failed ACLR. 4,6,14 More specifically, a nonanatomic femoral tunnel position is the most common cause of primary ACLR failure. 9 Nonanatomic tunnel drilling techniques fail to place the femoral tunnel within the native ACL position, leading to more vertical graft placement. 12 Subsequently, the modified transtibial, anteromedial, and outside-in techniques for femoral tunnel position have been improved to achieve a more anatomical tunnel position and enhanced rotational stability. 2,17,18 Although various surgical techniques for optimal tunnel position have been developed, tunnel malposition still persists. 1,8
The vertical graft may cause knee laxity with rotational instability. Revision ACLR is indicated if patients have persistent knee pain and subjective laxity. If magnetic resonance imaging (MRI) confirms that the original vertical ACL graft is loosened or partially torn, 2 possible solutions are considered. The first and conventional method is to remove the primary vertical graft and replace it with a new graft; however, this eliminates any potential benefit arising from the residual stabilizing effect of the remnant tissue of the primary vertical graft. The remnant vertical graft may provide anteroposterior stability, although it does not contribute to rotational stability. If the existing primary graft appears partially intact on MRI, surgeons could consider remnant-preserving revision ACLR as an alternative approach in such cases. A previous surgical technique has also suggested “double-bundle augmentation” of the primary vertical graft. 3 By placing a new femoral tunnel lateral to the primary vertical graft, the remnant-preserved ACL graft can contribute to knee stability. Patients may benefit from this technique during revision when the primary graft is vertical and appears loosened or partially intact.
In this study, we evaluated the effects of remnant preservation of primary vertical graft in revision ACLR. We compared revision ACLR with and without remnant preservation in a single-surgeon series, hypothesizing that remnant tissue preservation will provide better subjective clinical outcomes than those achieved without remnant preservation in revision ACLR. In addition, we hypothesized that the degree of primary ACL graft coverage with remnant tissue would affect clinical outcomes and stability.
Methods
Patients
After receiving institutional review board approval for the study protocol, a retrospective analysis was performed on 74 consecutive patients who underwent revision ACLR using the remnant-preserving technique between 2013 and 2017, and informed consent was waived. Surgical indications for revision ACLR included persistent or recurrent subjective instability after a previous ACLR; limitation of daily or athletic activities; objective instability with both positive Lachman and positive pivot-shift testing; and MRI demonstrating the failure of a previous ACL graft, which includes loosening or partial tear of a previous vertical graft. Patients who fulfilled the following criteria were included in the study: (1) 1-stage revision ACLR after primary ACLR and (2) a minimum of 2 years of clinical follow-up. The exclusion criteria were as follows: (1) a history of multiple-ligament injury, (2) chondral lesion with an Outerbridge grade >3, and (3) meniscal defect such as subtotal or total meniscectomy state. Subtotal meniscectomy was defined as a meniscectomy with 3 mm of the peripheral meniscus remaining with an intact rim and root attachments.
Surgical Techniques and Rehabilitation
A single senior surgeon (J.H.A) performed revision ACLR using a single-bundle graft. After confirming primary ACL graft failure through arthroscopic examination, a tibialis anterior tendon allograft, Achilles tendon allograft, or quadruple hamstring autograft was used for 1-stage revision ACLR. Unless tibial tunnel widening was present, the tibialis anterior allograft was used for the revision ACLR. However, reconstruction at a wide tibial tunnel was performed with the Achilles tendon and residual Achilles bone. A tibialis anterior tendon with allobone chips or an autologous iliac bone graft was also performed for a wide tibial tunnel. If patients had an intact harvestable hamstring tendon, a 4-strand hamstring tendon autograft was used. Of the 74 patients, 65 (87.8%) had tibialis anterior tendon allografts, whereas 5 (6.8%) had Achilles tendon allografts. In 4 knees (5.3%), revision reconstruction was performed using double-loop semitendinosus and gracilis autografts. The (fresh-frozen) allograft was irradiated at 12.8 to 19.8 kGy and controlled using a tissue preservation technique (Allowash Process; LifeNet Health). Efforts were made to preserve the remnants of the previous ACL tendon or graft. We attempted to preserve any thickness or length of the remnant tissue if it did not cause any impingement during knee motion. The remnant tissue was sutured using a suture hook with a No. 0 polydioxanone synthetic suture (Ethicon). The free ends of the suture were retrieved through a femoral tunnel. Both free ends were tied to a suspensory fixation device.
To observe the posterior aspect of the lateral femoral condyle, a 70° arthroscope was inserted through the posterolateral (PL) compartment. The arthroscope showed the posterior aspect of the intercondylar notch. The remnant of the previous ACL graft and the inner margin of the cartilage were visualized through the PL viewing portal. The failed graft and fibrous soft tissue were minimally debrided using a shaver or electrocautery to preserve synovialized remnant tissue. Under visualization through the PL portal, a FlipCutter (Arthrex) guide tip was positioned at the center of the previous femoral tunnel if this was located at the anatomical position. However, if the previous femoral tunnel was not in the anatomical position in the preoperative computed tomography scan, an entirely new femoral tunnel was drilled. New femoral tunnels were drilled either completely or incompletely to avoid preexisting tunnels (Figure 1A). After the guide pin was drilled into the intra-articular space using the outside-in technique, the FlipCutter was engaged into the joint space and retrodrilled around 25 to 30 mm to create a femoral tunnel. The femoral tunnel was drilled while observing through the PL viewing portal. After femoral tunnel drilling, the tibial tunnel was drilled. A tibial tunnel guide pin was inserted considering the position of the previous tibial tunnel and remnant tissue (Figure 1B). A new tibial tunnel was made adjacent to the previous tunnel and subsequently overlapped with the previous tunnel to preserve remnant tissue (Figure 1, C and D). We used an allobone or autobone graft when the tibial tunnel diameter exceeded 14 mm or stronger fixation was unavailable. When the aperture of the tibial tunnel was on the anatomical area, we created a divergent tibial tunnel. Although some tibial tunnel apertures were made larger, strong fixation was available using the bone graft and divergent tunnel. After tibial tunnel drilling, the graft was passed through the tibial tunnel while using the ACL TightRope (Arthrex) for femoral fixation. A biointerference screw (BioScrew; ConMed Linvatec), an additional screw (4.0-mm cancellous screw; DePuy Synthes), and a washer were used for tibial fixation.
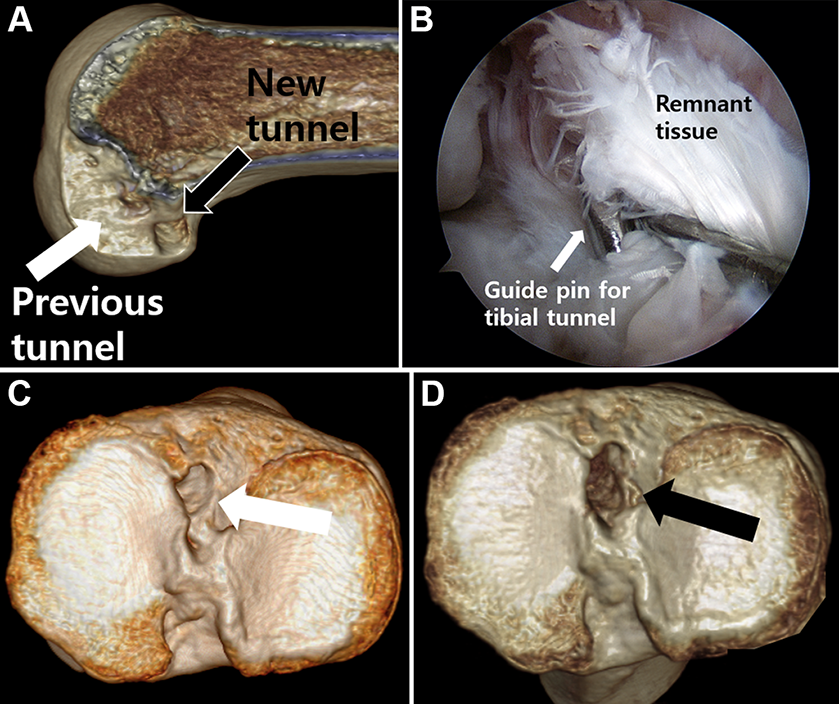
Revision anterior cruciate ligament (ACL) reconstruction with remnant tissue preservation. (A) The previous femoral tunnel aperture was located in a vertical position (white arrow), and the new femoral tunnel was located at a deeper and lower position than the previous tunnel (black arrow) on a 3-dimensional computed tomography (CT) image. (B) A guide pin for the tibial tunnel was inserted adjacent to the previous ACL graft to preserve the remnant tissue. (C) The previous tibial tunnel aperture was located in an anatomical position on a 3-dimensional CT image (white arrow). (D) The new tibial tunnel overlapped with the previous tunnel and was located in an anatomical position (black arrow).
If the previous femoral tunnel was widened and anatomically positioned, staged revision ACLR was performed. However, if the previous tibial tunnel was widened only to <14 mm, revision ACLR with a 1-stage bone graft at a wide tibial tunnel with residual Achilles bone, allobone chips, or an autologous iliac bone graft was performed. The Achilles tendon allograft was passed through the tibial tunnel. The tibialis anterior allograft and hamstring autograft were passed through the tibial tunnel unless tunnel widening was present. The ACL TightRope was used for femoral fixation. A biointerference screw (BioScrew), an additional screw (4.0-mm cancellous screw), and a washer were used for tibial fixation.
The same postoperative rehabilitation regimen was used for all patients, except for those who required meniscal repair. All patients began immediate isometric quadriceps and active range of motion exercises. During the first postoperative week, partial weightbearing within a tolerable range was allowed, an ACL brace was fitted, and range of motion exercises were performed with a 15° increase each week. At 4 and 6 weeks postoperatively, 90° and 135° motions were allowed, respectively. At 6 and 9 months postoperatively, straight-line running and direction changes while running were allowed, respectively. When meniscal repair was performed, rehabilitation was generally modified to exclude weightbearing activities and 90° of knee flexion for the first 6 weeks.
Evaluation of Remnant Tissue and Categorization
A senior surgeon (J.H.A) evaluated and recorded the status of previous ACL grafts during surgery. The medical record described the presence and quality of the ACL remnant. Intraoperative arthroscopic photographs were available for review as part of the documentation.
The morphological type of the remnant was also evaluated and classified into 4 types, as previously described by Crain et al 5 for assessing remnant ACL tissue in primary ACLR. Remnants preserved during the creation of the tibial and femoral tunnels were classified as group R (remnant). Knees with Crain type 1, 2, or 3 remnant tissues, whose proximal end was attached to the femur or posterior cruciate ligament, were also categorized as group R. Patients in group R were divided into 2 subgroups to analyze the effect of the initial graft coverage degree on clinical results. One was the “sufficiently preserved subgroup” (subgroup SP) (Figure 2), in which ≥50% of the graft surface could be covered with the remnant tissue at the end of revision ACLR. The other was the “insufficiently preserved subgroup” (subgroup IP), in which <50% of the graft surface was covered with remnant tissue (Figure 3). The other patients whose remnant tissues were absent or sacrificed were classified as group NR (no remnant). Knees with Crain type 4 remnant tissue, whose distal end was attached to the tibia while the proximal end was not attached anywhere, were also categorized as group NR.
Using intraoperative arthroscopic pictures and medical records, 2 orthopaedic surgeons (D.W.S and D.W.P) evaluated how much the graft surface was covered with remnant tissue retrospectively. The percentages of graft coverage measured by the 2 orthopaedic surgeons were averaged. Two fellowship-trained orthopaedic surgeons assessed the remnant graft coverage percentage on arthroscopic pictures twice, with an interval of 2 weeks. The raters were blinded to all information other than the arthroscopic images.

Arthroscopic picture of a representative case for the “sufficiently preserved subgroup,” in which 50% or more of the graft surface was covered with remnant tissue at the end of revision anterior cruciate ligament (ACL) reconstruction. A 34-year-old man had persistent pain and instability (grade 2 Lachman test and grade 2 pivot-shift instability). (A) The previous ACL graft was loosened and located at a nonanatomic vertical area in arthroscopy. (B) Preoperative computed tomography scan showing a relatively nonanatomic vertical position of the femoral tunnel. During the arthroscopic surgery of the revision ACL reconstruction, a thinning vertical remnant tissue (black arrow) was observed. (C) Intraoperative arthroscopic picture during the revision ACL reconstruction showing that the vertical remnant tissue (black double arrow) covered over 50% of the new ACL graft (white double arrow). (D) Postoperative 1-month routine follow-up magnetic resonance imaging scan showing both the remnant tissue and the new ACL graft on oblique axial view.

Arthroscopic picture of a representative case for the “insufficiently preserved subgroup,” in which 49% or less of the graft surface was covered with remnant tissue. A 27-year-old man had right knee pain and subjective instability (Lachman: grade 2; pivot-shift: grade 2). Preoperative (A) arthroscopic picture and (B) magnetic resonance imaging (MRI) scan showing the remnant tissue. (C) Intraoperative arthroscopic picture and (D) postoperative 1-month routine follow-up MRI scan showing both the remnant tissue and the new ACL graft.
Assessment of Clinical Outcomes
Clinical evaluations, including objective assessment and clinical knee scores, were obtained preoperatively and postoperatively for 6 months and annually. The objective assessments included the Lachman and pivot-shift tests, which were performed by a senior orthopaedic surgeon (J.H.A). After surgery, clinical evaluations were conducted using a Telos stress radiography device. If patients agreed to undergo postoperative routine MRI, postoperative routine follow-up MRI was obtained as part of the clinical protocol at 1 month, 6 months, and annually (Figures 2D and 3D). Knee pain and functional scores were assessed using the Lysholm score, the International Knee Documentation Committee (IKDC) subjective form, and the Tegner activity scale. The objective and subjective outcomes were compared between the groups. Preoperative scores and data from the time of the last follow-up were retrospectively collected from medical records for evaluation.
Graft Failure
Graft failure was defined as the need for additional surgery (re-revision ACLR with or without anterolateral ligament reconstruction) after revision ACLR. If the clinical history and physical examination were compatible with ACL graft failure, MRI was performed. ACL graft failure was diagnosed using MRI and physical examinations of evident instability on Lachman test, pivot-shift test, or Telos stress radiographs.
Statistical Analysis
All statistical analyses were conducted using SPSS software (Version 20.0; IBM Corp). For a priori power analysis, the sample size was based on the postoperative side-to-side difference (SSD) on Telos stress radiographs among the 3 groups (groups SP, IP, and NR). The means of the 3 groups for 5 patients were 2.4, 3.9, and 5.4 mm, respectively, and the SD was 3.1 mm. For an alpha of .05 and 80% power, the required total sample size was 66 patients. The current study involved 74 patients.
The intraobserver and interobserver reliabilities in measurements of the graft coverage of the 3 groups were assessed using the intraclass correlation coefficient with the respective 95% CIs. Mean differences for continuous variables were compared with the t test for normal distribution data. The Shapiro-Wilk test was used to determine whether the continuous variables were normally distributed, and the Mann-Whitney test was used when the data were not normally distributed. Comparisons for categorical variables were performed using the chi-square test or Fisher exact test (when the sample size was <5). For the chi-square test for trends, a linear-by-linear association was used. Analyses among the 3 subgroups were performed using the analysis of variance with a Bonferroni/Dunn correction for multiple comparisons or a chi-square test. The Kruskal-Wallis test was used when the data were not normally distributed. A P value <.05 was considered statistically significant.
Results
Patient Characteristics
In total, 98 patients underwent revision ACLR, and 24 were excluded. Hence, 74 patients were included in the present study. Figure 4 illustrates the flowchart for patient inclusion.

Flowchart of patient enrollment. For subgroup SP (sufficiently preserved), ≥50% of the graft surface was covered with remnant tissue; for subgroup IP (insufficiently preserved), <50% of the graft surface was covered with remnant tissue. ACL, anterior cruciate ligament; IP, insufficiently preserved ; NR, no remnant; OB, Outerbridge; SP, sufficiently preserved.
The mean time to final follow-up was 40.7 ± 16.8 months; 26 patients underwent remnant sacrifice and were classified into group NR, and the remaining 48 patients who underwent remnant preservation comprised group R. No significant differences existed between the groups regarding any demographic data, except for remnant Crain type (Table 1).
Preoperative Demographic Data and Clinical Characteristics a

a Data are presented as mean ± SD unless otherwise indicated. Boldface P value indicates a statistically significant difference between groups (P < .05). ACLR, anterior cruciate ligament reconstruction; NR, no remnant; R, remnant. Deg, degree; mo, months.
Clinical Outcomes and Graft Failure
At the last follow-up, the mean IKDC, Lysholm, and Tegner scores for both groups significantly improved compared with the preoperative scores. Neither the preoperative nor postoperative subjective outcome scores showed significant differences between the 2 groups. In both groups, the results of the Lachman and pivot-shift tests and anterior tibial translation SSD on Telos stress radiographs significantly improved postoperatively compared with those before the operation. No significant difference was observed in the results of the preoperative Lachman and pivot-shift tests between the 2 groups; however, the preoperative Telos SSD significantly differed. Group NR showed a significant preoperative Telos SSD difference compared with group R (Table 2). After revision ACLR, group R showed significantly superior results on the postoperative Lachman test and Telos SSD compared with group NR (Table 2).
Subjective and Objective Outcomes at the Last Follow-up a
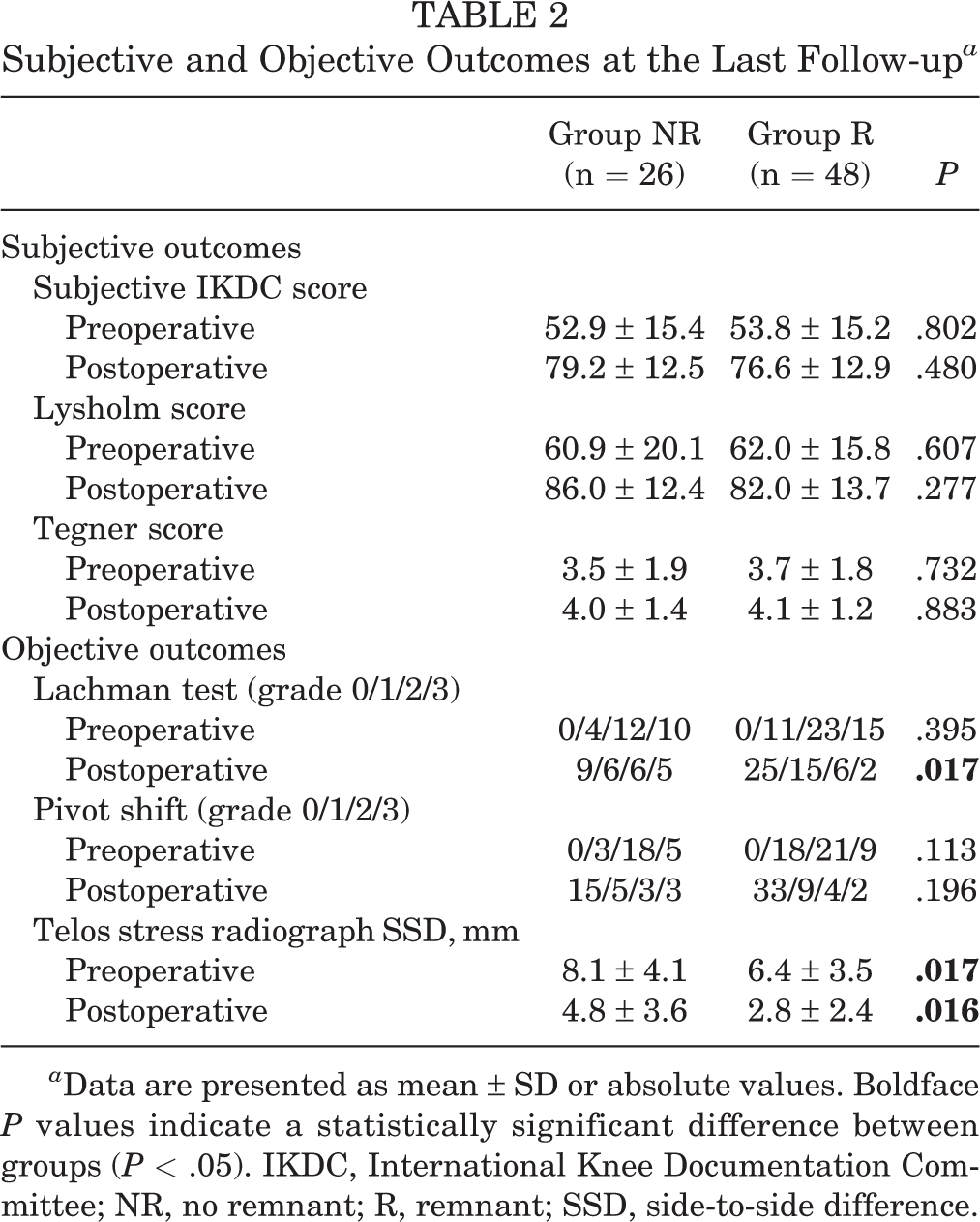
a Data are presented as mean ± SD or absolute values. Boldface P values indicate a statistically significant difference between groups (P < .05). IKDC, International Knee Documentation Committee; NR, no remnant; R, remnant; SSD, side-to-side difference.
There were 6 failures (23%) in group NR and 2 (4%) in group R, and the difference in the graft failure rate between the 2 groups was significant (P = .019). The 8 graft failures were confirmed by follow-up MRI scans and physical examinations. The cause of these failures was traumatic events in 5 patients after the revision ACLR. Three patients in group NR and 2 in group R had traumatic events. Four patients underwent revision ACLR and 2 await revision surgery in group NR. Two patients underwent revision ACLR in group R.
Effect of the Degree of Initial Graft Coverage
Concerning the preoperative Lachman and pivot-shift tests, the linear-by-linear association showed no significant differences between the 2 subgroups and group NR (P = .179 and .147, respectively). However, the postoperative Lachman test showed a significant difference between the 2 subgroups and group NR (P = .035). A significant difference in the Telos stress device SSD was observed preoperatively (P = .002) among the groups (Table 3), which was also observed postoperatively among the groups (P = .001). The post hoc test indicated that the postoperative Telos SSD in subgroup SP significantly outperformed that in group NR (P = .001), although no significant difference existed between subgroup IP and group NR (P = .850).
Effect of the Degree of Initial Graft Coverage Between the 2 Subgroups and Group NR a

a Data are presented as mean ± SD or absolute values. Boldface P values indicate a statistically significant difference between groups (P < .05). IP, insufficiently preserved; NR, no remnant; SP, sufficiently preserved; SSD, side-to-side difference.
Evaluation of Remnant Tissue
From the review of arthroscopic pictures and medical records, 8 patients had Crain type 1 remnants, 41 patients had type 2 remnants, 2 patients had type 3 remnants, and 23 patients had type 4 remnants. All Crain type 4 remnants were sacrificed, and 1 of type 1 and 2 of type 2 remnants were also sacrificed due to insufficiency for preservation. There was a significant difference with respect to Crain type between groups R and NR (P <.001).
The evaluation of remnant graft coverage revealed that groups SP, IP, and NR comprised 25, 23, and 26 patients, respectively. The intraobserver reliabilities for patient classification of groups SP, IP, and NR were 0.93 (95% CI, 0.87-0.96) for observer 1 and 0.91 (95% CI, 0.86-0.94) for observer 2. The interobserver reliability was 0.85 (95% CI, 0.74-0.92).
Discussion
The main finding of the present study is that vertical remnant preservation in revision ACLR may benefit postoperative knee anteroposterior stability and reduce graft failure rates. To our knowledge, studies that compare clinical results between remnant-preserved and NR groups after revision ACLR are rare. This study’s results showed that the degree of initial graft coverage with remnant tissue significantly affected postoperative knee stability. The subjective and functional clinical outcomes did not significantly differ between the 2 groups. Although knee stability significantly improved in the vertical remnant-preserved group, it did not result in significantly better results on subjective clinical outcomes. Therefore, the long-term results of future studies may be helpful because the significantly improved knee stability in the vertical remnant-preserved group may affect the long-term clinical outcomes related to postoperative meniscal injury and cartilage degenerations.
There was a report of an operative technique for the existing vertical graft, which appears intact and well integrated on MRI. 3 This technique left the original reconstructed vertical ACL graft in place, and a second additional graft was created by placing a new tibial tunnel anterior to the original and the new femoral tunnel lateral to the original. This technique may benefit those with an intact primary vertical graft and rotational instability more than those with translational instability. Notably, the clinical and functional results of remnant-preserving primary ACLR have been reported. 7,11,15,16,19 Although previous studies have reported similar clinical outcomes and stability of remnant-preserving primary ACLR, the outcomes of remnant-preserving revision ACLR have rarely been reported. This study suggested that remnant vertical tissue with sufficient graft coverage may favor stability and reduce the failure rate of revision ACLR, although further studies should be performed to confirm the results.
In the present study, a significant difference was seen in preoperative laxity SSD between the remnant-preserved and NR groups. The remnant tissue of the previous ACL graft was bridged from the tibia to the femur, affecting preoperative stability more than in group NR. A previous study also reported a significant difference in preoperative knee laxity according to remnant tissue type. Crain et al 5 recommended caution in resecting the torn ACL or scar tissue because removing this tissue contributed to increased anterior laxity in some ACL-deficient knees. Maeda et al 13 assessed knee laxity before and after resection of the ACL remnant using a navigation system. They reported that the mean anterior tibial translation at 15° of knee flexion before resection significantly increased after resection in Crain type 3 knees. Nakamae et al 15 evaluated the biomechanical function of ACL remnants in anterior and rotational knee stability in a complete ACL injury. They found that ACL remnants contributed to anteroposterior knee stability evaluated at 30° of knee flexion for up to 1 year after injury. However, another study reported no significant difference in preoperative knee laxity according to Crain type in primary ACLR, 11 after comparing types 1, 2, and 3 knees with type 4 knees. They concluded that the ACL remnant does not play a major role in knee stability. In the present study, the remnant tissue type of the previous ACL graft affected preoperative knee stability. The sufficiently preserved ACL remnants had better preoperative and postoperative anteroposterior knee stability than group NR.
The subgroup analysis revealed that only remnants with good graft coverage favored stability. The degree of initial graft coverage with remnant tissue could affect clinical outcomes and stability in ACLR. Kim et al 10 divided patients into 2 groups according to whether the amount of preserved remnant exceeded 50% or not. They reported that >50% remnant preservation positively affected graft synovialization and clinical outcomes. Kondo et al 11 divided patients into sufficiently and insufficiently preserved subgroups by the proportion of graft surface covered with the remnant tissue and reported that the degree of initial graft coverage significantly affected postoperative knee stability. This suggests that the quantity and quality of preserved remnant tissue after primary ACLR are important factors for clinical outcomes. The present study suggests that preserving remnant tissue in revision ACLR may favor knee stability if the initial coverage of the remnant graft is sufficient.
Several explanations may be possible for how postoperative knee stability was significantly improved by the sufficient preservation of the ACL remnant tissue. First, because the preoperative SSD on Telos radiographs was significant between the 2 groups, remnant tissue may contribute to anteroposterior knee stability. Second, because ACL graft remnants have varying degrees of synovium and vascularity in their fibers, remnant preservation in revision ACLR may promote revascularization and biologic healing of the revised ACL graft. Third, the graft failure rate of group NR exceeded that of group R. In the present study, most patients in group NR had no remnant to preserve, and they had more graft failures than the remnant-preserved group.
Limitations
This study has several limitations. First, this was a retrospective study with a small number of patients, which may have led to a lack of significant differences between certain variables. Second, although many factors contributed to the results of the revision ACLR, we focused mainly on remnant preservation. However, this is a common limitation in a clinical study, and we believe that the design of this comparative study is acceptable for clinical research. We also believe that this study will be helpful as the first clinical research on remnant preservation in revision ACLR. Third, some previous details regarding primary ACL surgery were missing. The details of the initial graft choice, prior meniscectomy, and prior articular cartilage injuries were not described in this study. However, we confirmed that no significant differences existed between the groups in the preoperative demographic. Fourth, the clinical failure rate was determined by the need for additional surgery after the revision ACLR. The decision of revision surgery could be affected by the surgeon’s selection bias. However, this is a common definition of graft failure, which was frequently used in previous studies. We believe that the definition of graft failure is acceptable for clinical research. Fifth, the follow-up period was insufficient to evaluate long-term outcomes. Therefore, further evaluation is needed to confirm whether there will be differences between the 2 groups in long-term clinical outcomes.
Conclusion
The remnant preservation of the primary vertical graft in revision ACLR may result in better anteroposterior stability. However, subjective outcomes in group R did not exceed those of group NR. The subgroup analysis revealed that only sufficiently preserved remnants demonstrated better anteroposterior stability.
Footnotes
Final revision submitted August 12, 2022; accepted September 8, 2022.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Kangbuk Samsung Hospital (reference No. KBSMC 2022-04-002).