
Abstract
Background:
Recovery from orthopaedic surgery in the adolescent population can be complicated by socioeconomic barriers and known health care disparities prevalent among racial/ethnic groups. Such barriers can negatively affect patient outcomes, particularly if accessibility to postoperative physical therapy (PT) is affected.
Purpose:
To determine the effect of race, ethnicity, language spoken, or Child Opportunity Index (COI) on recovery from glenohumeral labral repair in the pediatric population.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients who underwent glenohumeral labral repair at a single center between September 2009 and December 2018 were reviewed. The inclusion criteria were pre- and postoperative data available at the time of chart review, with a minimum of 2 postoperative appointments with the surgeon. Charts were reviewed to gather demographic and clinical data, including age, sex, race, ethnicity, pre- and postoperative visits with the surgeon, and PT data. Cohorts of Hispanic or Latino (HL) and non-Hispanic (NH) were analyzed along with COI classification levels and outcomes.
Results:
A total of 132 patients met the inclusion criteria—61(46%) women and 40 (30%) HL patients—with a mean age of 15.5 years. There was no difference between HL and NH patients regarding the time from injury to initial visit, the time from initial visit to surgery, and the number of postoperative clinic visits with the surgeon (P > .05). The NH cohort had more PT sessions completed postoperatively (24 sessions) than the HL cohort (19 sessions) (P = .024). There was a significant difference in the rate of PT cancellations based on COI, with the high and very high opportunity groups having the most cancellations (P = .029). When COI was added as a covariate, no differences were observed based on ethnicity regarding any of the outcome variables (P > .05).
Conclusion:
Ethnicity appears to independently factor into postoperative PT session attendance. Patients living in areas with the highest opportunity index had higher rates of postoperative PT cancellations. Future studies should focus on longer-term outcomes, rather than the ability to attend postoperative PT, to further identify whether ethnicity is truly a factor for any discrepancies in health care related to glenolabral repair in the pediatric population.
Keywords
Access to health care has been identified in the literature as a factor that can negatively affect pediatric outcomes. 9 Poor access to health care tends to be correlated with minority populations and with those who have government insurance. 8 Most pediatric studies have focused on knee pathology, such as anterior cruciate ligament (ACL) and medial patellofemoral ligament reconstructions.4,8,16,17 Regarding ACL injuries, Black and Hispanic patients have longer delays to surgery, worse pathology at presentation, fewer physical therapy (PT) visits, and greater residual weakness at 9-month follow-ups. 8 Government insurance has also been correlated with delays in orthopaedic care and greater risk for more advanced pathology at the time of presentation.4,16,17 Government-insured adolescent patients with shoulder instability have higher rates of postoperative shoulder dislocations than their privately insured counterparts.11,13 Studies on shoulder instability and insurance type have also been performed; nevertheless, they have not concurrently evaluated other aspects of one’s surrounding environment, such as educational opportunities or the health of one’s community.
In the adult population, PT has been established as a mainstay in recovery for glenohumeral labral repair, and utilization of PT is higher in those with private insurance compared with those with government insurance.5,14 In addition to insurance type, language spoken may also affect quality of care, as it has been demonstrated that the use of an interpreter improves patient communication, utilization of health care, clinical outcomes, and satisfaction with care in adult patients. 12 To address these disparities in care, specifically in the pediatric population, the Child Opportunity Index (COI) has been developed as a measure of neighborhood-based conditions and resources conducive to healthy child development and may be used to inform community interventions.1,2 The COI is a validated approach to social determinants of health in the pediatric population that assesses 3 domains of a community: education, health and environment, and social and economic.1,2 High opportunity neighborhoods are defined as those with quality schools, parks and playgrounds, clean air, access to healthy food, health care, and safe housing, whereas low opportunity neighborhoods lack those resources. Understanding the interplay between various factors that influence access to care, quality of care, and utilization of resources such as PT is crucial for optimizing outcomes for individuals from diverse backgrounds.
This study aimed to determine the effect of ethnicity, language spoken, and COI on the ability to attend postoperative PT after glenohumeral labral repair in the pediatric population. Our primary aim was to determine whether ethnicity or COI could independently explain any disparities noted in access for our pediatric population with this pathology. We hypothesized that ethnicity and/or COI would contribute to disparities in the adolescent patients’ ability to attend postoperative PT for shoulder instability. The secondary aim was to confirm the historical findings regarding presurgical access to health care related to these known risk factors in our cohort of patients.
Methods
A retrospective review of patients who underwent glenohumeral labral repair at a standalone tertiary pediatric referral center between September 2009 and December 2018 was performed. To reflect all labral pathology types equally (posterior, superior labrum anterior posterior [SLAP], multidirectional instability, and anterior) without an emphasis on anterior pathology, 4 separate, formerly developed datasets were utilized in a combined fashion for this project. Each dataset was created by identifying patients via hospital electronic medical records and a search for Current Procedural Terminology codes 29806 and 29807, and then excluding other labral pathologies. The SLAP dataset included those between January 2011 and January 2018 without a previous history of ipsilateral shoulder surgery (48 patients). The posterior labrum dataset included 48 patients found between January 2011 and January 2018 with isolated injury. The multidirectional instability dataset included 42 patients seen between September 2009 and April 2017. Multidirectional instability was defined as the presence of a positive sulcus sign, a capacious capsule identified by a radiologist on magnetic resonance arthrogram and/or intraoperatively, and a drive-through sign on arthroscopy. The fourth dataset included all labral pathologies (including anterior) for those children treated between 2013 and 2018 who had patient-reported outcome scores preoperative and at 3 months postoperatively (95 patients). This original dataset was created to assess the minimal clinically important difference for shoulder outcomes. Thus, a final cohort was created that included a relatively symmetric sample size of all pathologies without an overemphasis on any unidirectional tear pattern.
The exclusion criteria involved those with a known collagen disease, such as Ehlers-Danlos syndrome, or surgical intervention at a different facility before presentation at our institution. Further exclusion criteria were applied, including insufficient information available about the PT course at the time of chart review, as this was a primary aim of this study, and loss to follow-up as indicated by <6 weeks of postoperative follow-ups or <2 postoperative clinic visits with the surgeon (intended to assess the initial prescription for PT without being limited by variable patient recovery, while capturing early PT that was initiated 2 weeks after surgery).
All patient charts from this combined dataset were then reviewed to gather demographic and clinical data, including age, sex, race, ethnicity, patient ZIP code, pre- and postoperative clinic visits attended, and PT data. Specific PT data included several visits, as well as a conversion of subjective information into an objective value entitled PT scheduling issues. These scheduling issues were identified through direct verbiage in electronic health record notes that indicated a patient was having difficulty scheduling or attending PT visits. Several attended/missed preoperative PT visits were not used in calculations.
Two ethnic cohorts were then developed, Hispanic or Latino (HL) and non-Hispanic (NH), for statistical comparisons based on ethnicity. Likewise, 2 primary language cohorts were developed for statistical comparisons, based on the child’s primary spoken language, which did not necessarily correlate with the primary language spoken at home, but for patients <18 years, most likely reflected the parents’ preferred language. Finally, COI classifications (generated by the COI 2.0 database reports) were applied to the children, grouping them as “very high,”“high,”“moderate,”“low,” and “very low” opportunity. Groups were compared utilizing analysis of variance for continuous outcomes and a chi-square test for categorical outcomes. A generalized linear model was utilized to analyze ethnicity with COI as a covariate. The alpha was set at P < .05 to declare significance. Statistical analysis was performed with SPSS Version 28 (IBM Corp).
Results
A total of 132 patients met the inclusion criteria—61 (46%) women and 71 (54%) men; mean age, 15.5 ± 1.8 years. Also, 40 (30%) patients were identified as HL, and 92 (70%) patients were identified as NH. A total of 125 (94%) patients spoke English as their primary language, and 7 (5%) children spoke Spanish as their primary language. There was no difference between HL patients and NH patients regarding the time from injury to initial visit, the time from injury or initial visit to surgery, or the number of pre- or postoperative visits (Table 1). There was a difference between HL and NH patients with regard to PT sessions completed postoperatively (Table 1).
Demographic Characteristics, Pre- and Postoperative Data, and PT Data for the 2 Groups a

Data are presented as mean ± SD. HL, Hispanic or Latino; NH, Non-Hispanic; Post, postoperatively; Pre, preoperative; PT, physical therapy.
Further analysis of COI and ethnicity revealed a difference in ethnicity distribution among COI groups (P = .047) (Table 2). A difference in PT cancellations was noted among COI classifications, with the high and very high COI groups having the highest rates of PT cancellations (P = .029) (Tables 3 and 4). The descriptive data for the rate of PT sessions completed postoperatively are also demonstrated in Table 4, which demonstrates that the high and very high groups had the highest rate of completion, although this did not reach statistical significance (P = .054). When adding COI as a covariate, no difference was observed based on ethnicity regarding any of the outcome variables (P > .05).
Distribution of Race and Ethnicity Across COI Groups a

Data are presented as n (%). The bold P value indicates significance. COI, Child Opportunity Index; HL, Hispanic or Latino; NH, Non-Hispanic.
Demographic Characteristics, Pre- and Postoperative Data, and PT Data for Patients Undergoing Glenohumeral Labral Repair Stratified by the COI Classification Using ANOVA a

Detailed numeric data for each COI classification (very low, low, moderate, high, very high) was removed for brevity for nonsignificant findings, as only the mean and standard deviation are reported here. Bold P values indicate significance. ANOVA, analysis of variance; COI, Child Opportunity Index; Post, postoperatively; Pre, preoperatively; PT, physical therapy.
PT Cancellations Postoperatively Stratified by COI Classification a
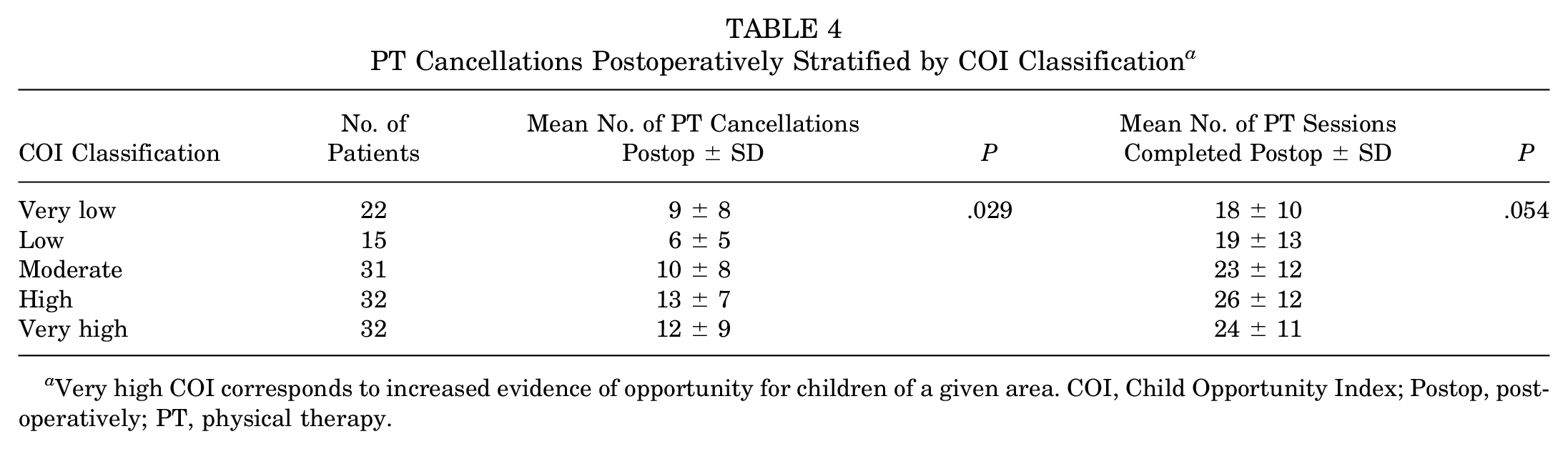
Very high COI corresponds to increased evidence of opportunity for children of a given area. COI, Child Opportunity Index; Postop, postoperatively; PT, physical therapy.
Discussion
Ethnicity may affect certain aspects of recovery in the pediatric population regarding arthroscopic management of glenolabral pathology, such as the number of PT sessions completed postoperatively. The highest COI groups demonstrated the highest rates of PT cancellations; however, the COI (as a proxy for social determinants of health) was not confirmed as a historical risk factor related to presurgical access to health care. Therefore, the hypothesis that ethnicity and COI would contribute to disparities in the adolescent patients’ ability to access care for shoulder instability is rejected. Both variables appear to correlate with rehabilitation attendance, but not necessarily in the expected manner. These findings suggest that perhaps a more complex interplay exists for ethnicity and opportunity in terms of access to care and behavior in scheduling and completing postoperative therapy.
There was a significant difference in the number of PT cancellations across COI groups, with the high and very high opportunity groups having greater rates of PT cancellations. This may be attributed in part to competing factors for those patients who live in areas with higher opportunity indices, being “too busy.” However, despite the differences in cancellation rates, there was a trend for the highest COI groups to have the most PT sessions completed postoperatively, suggesting that the cancelled PT sessions were made up on a different date. The present study design prevents further exploration of this discrepancy; nonetheless, it provides data for future research into this study question.
With regard to Hispanic ethnicity, without the COI covariate, the present study found that the number of PT sessions cancelled postoperatively was negatively affected by Hispanic ethnicity. The difference in PT visits may be attributed to logistical difficulties faced by HL patients in navigating health care systems, as described by Sealy-Jefferson et al,12,18 such as language barriers, bias, and culture. In this cohort, however, ethnicity did not affect the number of postoperative visits with the surgeon, which may suggest that the barriers facing this group of patients are most prominent outside of the primary patient and surgeon relationship.
The existing literature has established that insurance type and ethnicity can contribute to delays in accessing care.4,6,15,16,17 Bokshan et al 7 found that factors such as White race were associated with undergoing surgical stabilization within the same calendar year, and patients with higher incomes were more likely to have surgery within 30 days. Other studies suggest that minority race is associated with an increased number of preoperative dislocations, and patients with government insurance have a lower likelihood of undergoing surgical stabilization of glenohumeral instability compared with patients with commercial insurance.3,10 In this study, we specifically investigated the effect of ethnicity on access to care. There was no significant difference between HL and NH patients regarding the time from injury to first visit, the time from injury to surgery, or the time from first visit to surgery (see Table 1). While this study did not directly analyze insurance type as it relates to access to care, the COI may be used as a proxy for a broader approach to social determinants of health in this setting. As such, this population of patients did not experience delays in care as a result of their COI (see Table 3). These results may be a result of our local demographics (percentage of health care workers who speak the same language and are culturally part of the same patient population) or may potentially be related to the concerted efforts and investments in resources that have been undertaken by our facility to address this well-known disparity. No data are available to analyze the causative etiology.
Limitations
There are a few limitations associated with the retrospective design of this study and its small sample size. One limitation involves how PT scheduling issues were identified. Because of the limitations of the electronic health record system, more patients may have experienced scheduling issues, but they either did not convey it during their visit, or it was not recorded in the note. Further, because of the small sample size and relative distribution of the COI in the area, there were not enough COI numbers within each ethnicity to evaluate the COI as a categorical factor. Thus, we were unable to differentiate between each COI class (moderate, high, very high, et cetera) and were only able to evaluate as an ordinal trend based on increasing COI class. Related to patient selection, this presented cohort of patients contains a relatively equal distribution of posterior, superior, anterior, or multidirectional instability, which contrasts with the known percentages seen in the established literature regarding anterior instability as the most common shoulder instability type. Therefore, this study may represent a subset of patients whose instability direction and rehabilitation course may not be entirely generalizable to the pediatric shoulder instability population as a whole. 19 However, as the intent was to develop a more global understanding of all possible glenolabral pathology (not just anterior), the study design successfully achieved that outcome. Another limitation was the minimum follow-up criteria being defined as at least 2 postoperative clinic appointments attended, which achieved the goal of having values for at least 1 course of postoperative PT, but otherwise, it did not accurately depict the full recovery course. The listed preferred language in the chart most likely represented the parent/guardian’s preferred language in those <18 years, as they would have been the ones engaging with patient access representatives. The limitation is our inability to confirm this datapoint, or whether or not the patient would have changed the preferred language listed in the chart at the age of 18 years. A final limitation is that the present cohort percentages for ethnicity may not be generalizable to the United States as a whole, although they likely reflect the Southwestern region. Moreover, the high percentage of Hispanics and Spanish-speaking providers and support staff in our health care system could hypothetically augment the ability of Hispanic patients (with the means to do so) to achieve equal access to postoperative care for their glenohumeral labral repairs.
Conclusion
Ethnicity may affect certain aspects of adolescent shoulder instability surgery recovery, even though the more historically observed risk factor of disparity, represented by the COI in this investigation, had a minimal overall effect. Hispanic ethnicity had lower rates of completed postoperative PT sessions. Future studies should focus on longer-term outcomes to further delineate whether any of the observed discrepancies in care related to these predisposing risk factors truly contribute to repeat dislocation events or repeat surgery.
Footnotes
Final revision submitted January 31, 2025; accepted March 10, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: E.W.E. is a paid presenter or speaker for Arthrex; is a board or committee member of the Pediatric Orthopaedic Society of North America; and has received research support from RTI Surgical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of California, San Diego, Human Research Protections Program (Project #192008).