
Abstract
Background:
Open Latarjet (Lt) and arthroscopic Bankart associated with Hill-Sachs remplissage (BHSR) have been commonly proposed to treat anterior shoulder instability.
Hypothesis:
Patients undergoing either Latarjet or arthroscopic Bankart repair with remplissage, when matched according to relevant demographic and injury-specific variables, would have equivalent clinical and radiographic outcomes at a minimum 5-year follow-up.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
In a retrospective multicentric study, including 325 patients treated operatively for primary chronic anterior shoulder instability, 220 patients were reviewed with a minimum follow-up of 5 years. In this database, patients in the Lt and BSHR groups were matched 1 to 1 based on age at surgery, sex, amount of glenoid bone loss, and length and width of the Hill-Sachs lesion. Clinical outcomes were assessed using active range of motion, subjective shoulder value (SSV), Rowe scores, and Walch-Duplay scores. Recurrent instability, postoperative complications, and return to sports (RTS) were compared. Arthritis was evaluated according to the Samilson and Prieto classification.
Results:
A total of 68 patients (34 patients in the Lt group matched to 34 patients in the BHSR group) were analyzed at a mean follow-up of 90 ± 25 months. Preoperatively, the mean age was 25 ± 6.5 years, the glenoid bone loss was <6% (mean, 5.58% ± 5.52%), and the width and depth of the Hill-Sachs lesion were <27 mm (mean, 15.7 ± 6.91 mm) and 5 mm (mean, 4.8 ± 2.41 mm), respectively, in the 2 groups. Postoperatively, 1 hematoma required a revision in the Lt group. The recurrence rate was 6% (n = 2) in the Lt versus 14% (n = 5) in the BHSR group (P = .2) at the final follow-up. RTS at 1 year was higher in the Lt group (82% vs 62%; P < .01). There was no difference in active range of motion, Rowe scores, and Walch-Duplay scores at the last follow-up. However, the SSV was higher in the Lt group (92% vs 81%; P = .003). The arthritis rate was 20% (grade 1: n = 6; grade 2: n = 1) in the LT group versus 3% (grade 1: n = 1) in the BHSR group (P = .054), with no clinical effect on functional scores.
Conclusion:
At >7 years of follow-up, there was no statistical difference in the recurrence rate between patients in the Lt and BHSR groups. However, RTS was greater at 1 year after the Lt procedure. The possibility of degenerative arthritis developing in the Lt group is worrisome and requires a longer follow-up to assess potential clinical impairment.
The surgical technique to treat anterior shoulder instability remains controversial, depending on the disease characteristics and the patient’s profile.3,9,26 Anatomically, the amount of bone loss on the glenoid and/or humeral side is one of the highest determining factors in treatment choice.24,35 Since its first description by Bigliani in 1998, the definition of glenoid “critical” bone loss has varied from 10% to 25% depending on the author.30,36,40,41 Therefore, glenoid reconstruction with bone graft is required to restore shoulder stability above this level of defect 5 . However, in the case of “subcritical” (13% to 15%) or minor (<10%) glenoid bone loss, there is no clear indication for anterior glenoid bone graft or soft tissue procedure, including Bankart repair with or without Hill-Sachs remplissage.8,11,18,30,36
Although the Latarjet procedure has shown excellent long-term clinical results in terms of stability, concerns remain owing to the high complication rates reported in previous series.25,32 On the other hand, the addition of a Hill-Sachs remplissage has been reported to lower the risk of recurrence after a Bankart repair, especially in the setting of minor glenoid bone loss, and can be performed arthroscopically.2,12,14,16,17
Only a few studies have compared these 2 surgical techniques.15,19,20,30,34,44,46 Thus, our study aimed to compare the mid-term results of open Latarjet (Lt) and arthroscopic Bankart Hill-Sachs remplissage (BHSR) for the treatment of chronic anterior glenohumeral instability. We hypothesized that there would be no difference in clinical and radiological outcomes between the 2 techniques.
Methods
This was a matched-cohort retrospective study, performed on a continuous multicenter series (9 centers) of patients managed surgically from 2006 to 2017. This study was approved by the ethics committee (2022-A00373-40), and the patients consented to the use of their clinical and radiological data.
The inclusion criteria were as follows: (1) surgical management of patients (age >15 years) with chronic unidirectional anterior shoulder instability; (2) treatment with BHSR or Lt; and (3) review after a minimum follow-up of 5 years.
The exclusion criteria were as follows: (1) a missing preoperative computed tomography (CT) scan; and (2) surgical history of the shoulder involved or combined pathological features (eg, rotator cuff lesions, superior labrum anterior to posterior tear, or humeral avulsion of the glenohumeral ligament lesion), or revision surgery. The indication of Lt or BHSR was according to the surgeon’s preference. From the initial database of 325 patients, 220 met the inclusion/exclusion criteria (BHSR group, n = 35; Lt group, n = 185) before pair-matching 1 to 1.
Surgical Procedure
Patients underwent surgery in a beach-chair position under general anesthesia combined with a locoregional analgesic interscalene block.
The BHSR procedure was conducted with a 30° scope, and 3 different portals were used: the posterior viewing portal and 2 (anterosuperior and posterolateral) working portals.
The first step consisted of a glenohumeral exploration and glenoid preparation for Bankart repair: the labrum was mobilized from the glenoid neck, and a temporary suture traction was placed at the 5 o’clock position to shift the capsule. 6 The first simple-loaded anchor was placed at the 5 o’clock position, and the suture was passed through the labrum and anteroinferior capsule as distally as possible. Before tightening the suture anchor, the scope was switched to the anterosuperior portal, and the posterolateral accessory portal was used to perform the Hill-Sachs remplissage. A 6.5-mm working cannula was placed in the subdeltoid space, the Hill-Sachs lesion was prepared, and 2 anchors were inserted through the posterior capsule into the humeral head close to the medial edge of the Hill-Sachs lesion. A bridged construct was then performed for capsulotenodesis fixation and left aside for final tightening at the end of the procedure. The Bankart repair was finalized with 2 additional anchors at the 3- and 4-o’clock positions with capsular shift from south to north.
The Latarjet technique was performed conventionally using the deltopectoral approach. 45 The coracoid process was harvested while preserving the laterally attached coracoacromial ligament. The lower two-thirds of the subscapularis muscle was split, and the glenohumeral joint was exposed through a capsulotomy. The scapular neck was then freshened with an osteotome to flat cancellous bone. Depending on its size, the coracoid was fixed with either two 4.5-mm malleolar screws or two 3.5-mm AO screws. The coracoid was placed flush with the articular surface of the glenoid in the anteroinferior quadrant of the scapular neck. Last, the coracoacromial ligament stump was sutured to the capsule.
Postoperative Care
Each patient received the same analgesic protocol after surgery. The shoulder was placed in a sling in internal rotation for 3 weeks for the Lt group, and 6 weeks for the BHSR group postoperatively, as it is thought that soft tissue procedures require a longer time to heal. Self-rehabilitating pendular exercises were recommended in the immediate postoperative period as well as passive range of motion recovery under the supervision of a physical therapist, protecting external rotation until the sixth week. Thereafter, no restriction in range of motion was required, and muscle strengthening was started. Contact or throwing sports were allowed at the third month postoperatively for the Lt group, and at the sixth month for the BHSR group.
Clinical Assessment
Preoperative epidemiological data and postoperative systematic consultations were analyzed using patients’ medical records. After 5 years, a clinical examination was performed by an independent observer (K.L.) in a face-to-face consultation or via teleconsultation. A medical interview inquired about instability recurrence, defined as a subluxation or a complete dislocation. The time to return to sports (RTS), type, and level of sport were also assessed. Subjective assessment of shoulder function was evaluated using the subjective shoulder value (SSV) scale. 21 Active joint range of motion was measured using a goniometer (manual or digital on picture) in anterior elevation, external rotation with the elbow at the side, at 90° of abduction, and internal rotation. Internal rotation depended on the vertebral level reached by the thumb. These were all converted into points based on the Constant score. 21 Persistent apprehension was considered positive in case of fear of dislocation in overhead activities and/or during the apprehension test. The Rowe and Walch-Duplay scores were also calculated.38,43
Radiographic Assessment
Radiographic measurement was performed by a single shoulder-trained surgeon (K.L.) using previously validated methods.
Preoperative CT scans allowed measurement of the glenoid and humeral bone defects using Horos (Version 4.0.1) software.
The humeral bone defect was evaluated according to the Cho method. 16 The size of the Hill-Sachs lesion was measured in the axial plane at the level where the size of the lesion was the largest. A virtual circle that included the articular surface of the humeral head was drawn. The width was defined as the distance between both ends of the Hill-Sachs lesion, where the bone defect was located on the circle. The depth was defined as the longest length between the bottom of the lesion and the corresponding arc (Figure 1).
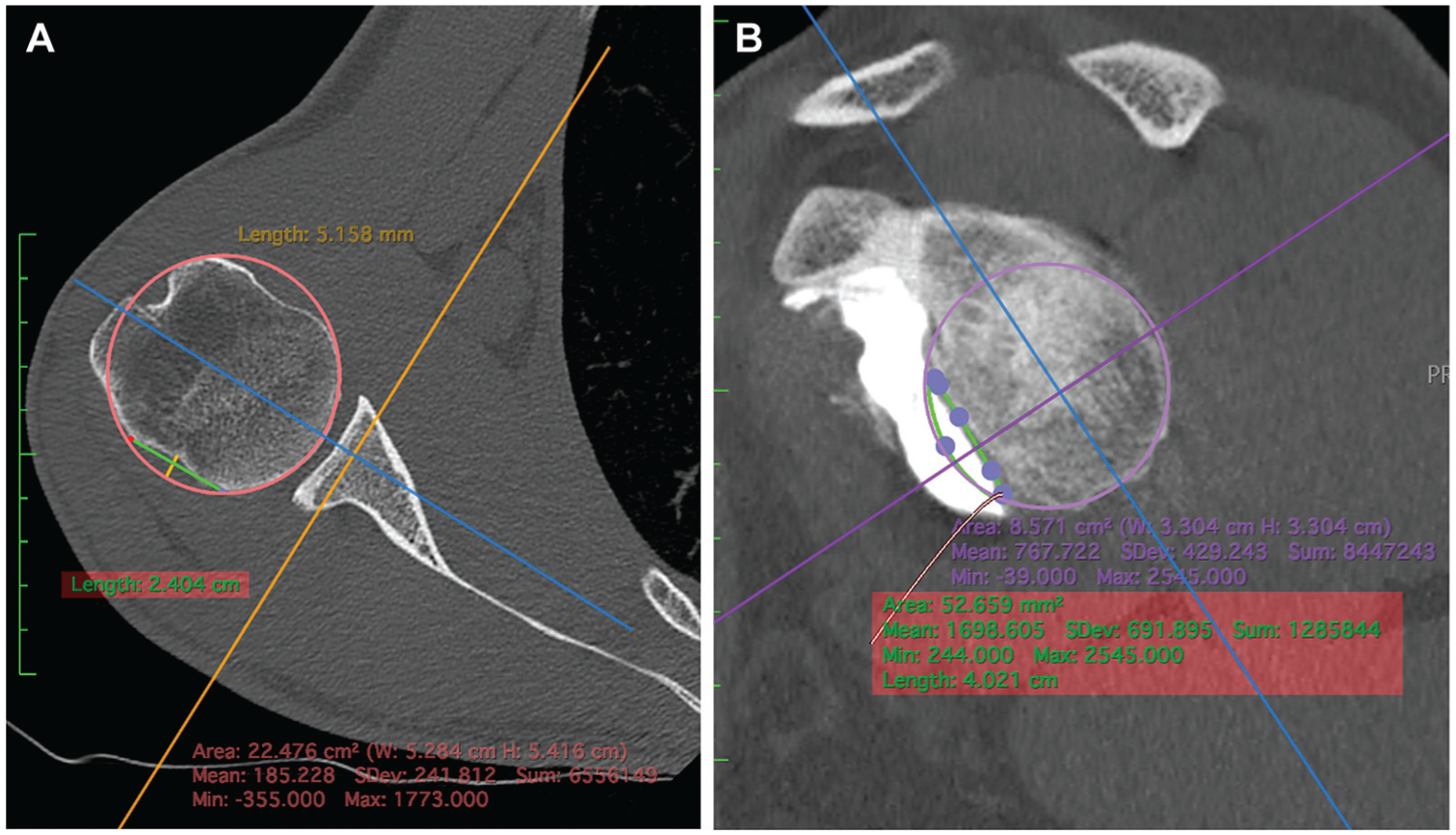
Humeral and glenoidal CT sections: examples of bipolar bone loss measurements, according to the Cho and Huijsmans techniques and using Horos (Version 4.0.1) software. (A) Humeral bone loss measured on axial section at the deepest point of Hill-Sachs lesion (depth and width in mm). (B) Glenoidal bone loss measured on a “face view” according to the “best-fit circle” technique. CT, computed tomography.
Glenoid bone loss was calculated using a 3-dimensional reconstruction model software, according to the “best-fit circle” technique published by Huijsmans et al. 28 On a sagittal “face view,” a circle was drawn using the posterior and inferior glenoid rims as a reference. The anterior missing surface was measured using a closed polygonal tool, built point by point along the edges of the missing surface to fulfill the initial “best-fit circle.” The percentage of bone loss was then calculated as follows: glenoid bone loss (%) = polygonal area × 100/initial circle area.
Finally, the glenoid track concept was used to classify the Hill-Sachs lesion as “engaging” or “non-engaging.” 17
At the last follow-up, degenerative arthritis was assessed on standard anteroposterior radiographs according to the Samilson and Prieto classification. 39
Statistical Analysis
Statistical analysis was performed using EasyMedStat (Version 3.30.2; www.easymedstat.com). Propensity scores were calculated using a logistic regression model and included the following 5 normalized covariates: age at inclusion; sex; and 3 radiological criteria measured on preoperative CT scans: (1) percentage of glenoid bone loss; (2) depth of the Hill-Sachs lesion; and (3) width of the Hill-Sachs lesion. A 1 to 1 matching was performed, and standardized mean differences (SMD) were calculated to compare baseline characteristics after matching. A postmatching SMD of <0.1 was considered an acceptable difference. The quality of analysis was assessed by a scoring method in percentage. The statistical analysis for clinical outcomes, recurrence, complications, and RTS was tested with the Fisher exact test. The alpha risk was set to .05.
Results
Study Population
After a 1-to-1 matching of BHSR and Lt groups, the EasyMedStat quality scoring method was found to be high (81.8%), and 34 patients were matched for each group (Figure 2). Postmatching SMD was <0.1 for age, glenoid bone loss, and depth and width of the Hill-Sachs lesion (Table 1).

Flow chart. BHSR, Bankart associated with Hill-Sachs remplissage.
Matching Variables a
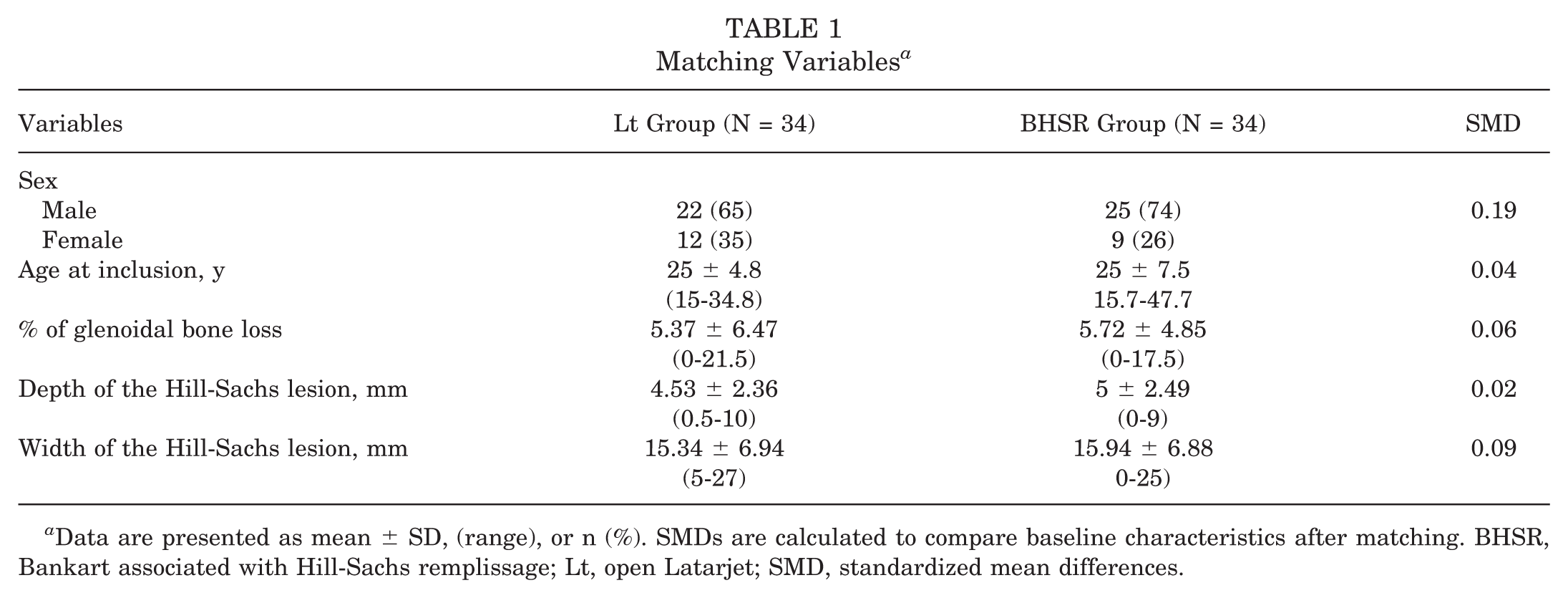
Data are presented as mean ± SD, (range), or n (%). SMDs are calculated to compare baseline characteristics after matching. BHSR, Bankart associated with Hill-Sachs remplissage; Lt, open Latarjet; SMD, standardized mean differences.
Initial demographic characteristics were assessed in Table 2. Preoperatively, the mean age was 25 ± 6.5 years, the glenoid bone loss was <6% (mean, 5.58% ± 5.52% ), and the width and depth of the Hill-Sachs lesion were <27 mm (mean, 15.7 ± 6.91 mm) and 5 mm (mean, 4.8 ± 2.41 mm), respectively, in the 2 groups. There was no significant statistical difference between groups except for sport level, which was higher in the Lt group, with 16 athletes practicing in competition (57%) (P < .001).
Demographic Characteristics of the 2 Groups a

Data are presented as mean ± SD or n (%). The bold P value indicates significance. BHSR, Bankart associated with Hill-Sachs remplissage; Lt, open Latarjet.
Shoulder hyperlaxity is defined as passive external rotation 1 (elbow at side) >85°.
Range of Motion and Functional Scores
At a mean follow-up of 90 ± 25 months, no significant statistical differences were found in active range of motion between the 2 groups (Table 3). Despite a higher rate of preoperative hyperlaxity (external rotation >85°) in the BHSR group, similar results were found in external rotation with the elbow at the side and 90° of abduction. Regarding functional scores, the SSV was the only one with a significant statistical difference between the 2 groups (Lt: 92%; BHSR: 81%; P = .003) (Table 3).
Clinical Results at the Follow-up a
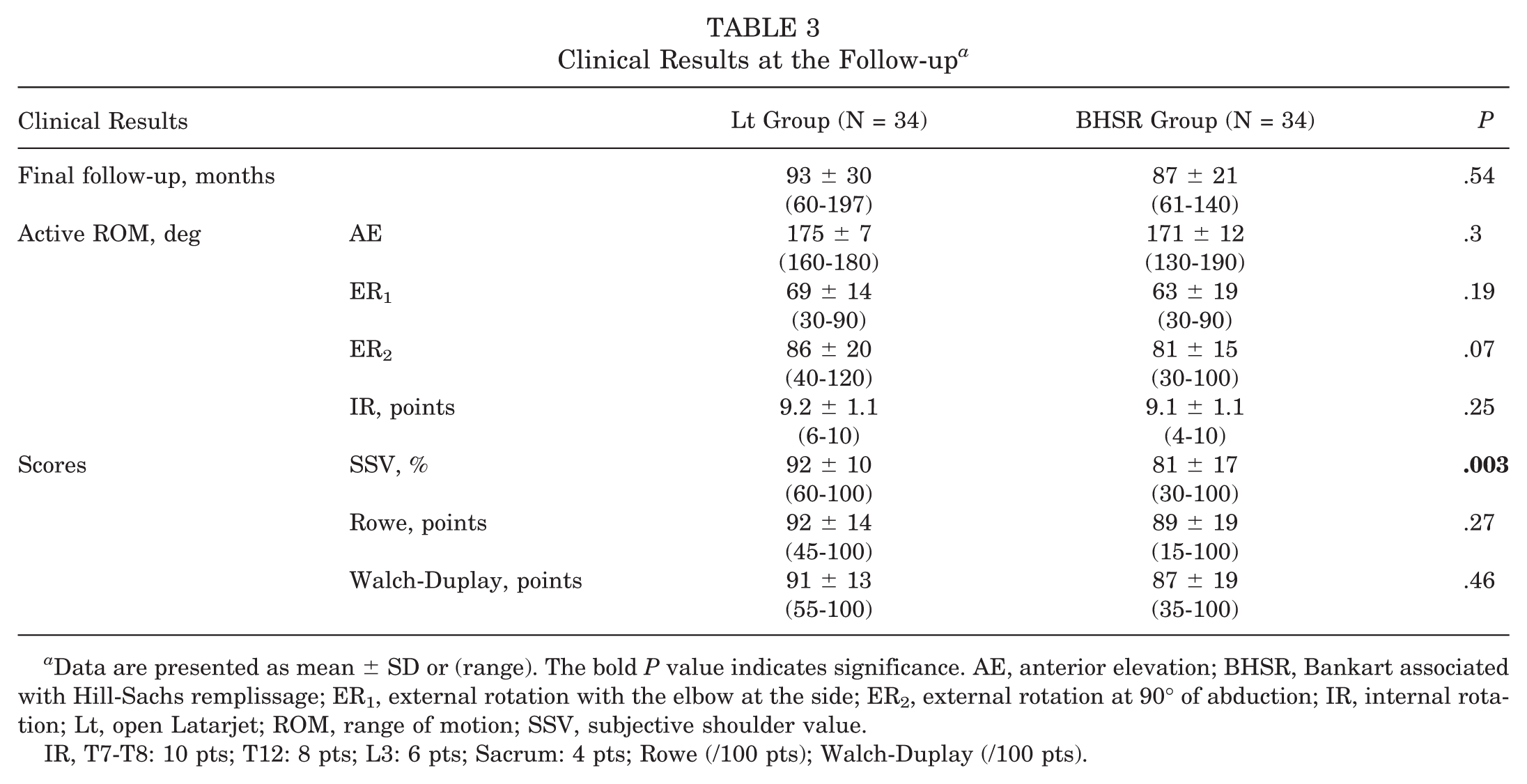
Data are presented as mean ± SD or (range). The bold P value indicates significance. AE, anterior elevation; BHSR, Bankart associated with Hill-Sachs remplissage; ER1, external rotation with the elbow at the side; ER2, external rotation at 90° of abduction; IR, internal rotation; Lt, open Latarjet; ROM, range of motion; SSV, subjective shoulder value.
IR, T7-T8: 10 pts; T12: 8 pts; L3: 6 pts; Sacrum: 4 pts; Rowe (/100 pts); Walch-Duplay (/100 pts).
Recurrence
In the Lt group at a mean follow-up of 93 months (mean ± SD, 93 ± 30; range, 60-197 months), the recurrence rate was 6% (n = 2), with 1 case (3%) occurring between 1 and 3 years and the other case (3%) at >5 years postoperatively. These recurrences were both classified as subluxations. In the BHSR group, at a mean follow-up of 87 months (mean ± SD, 87 ± 21; range, 61-140 months), 5 patients (14%) had a recurrence of instability, with dislocation (n = 4;12%) or subluxation (n = 1; 3%) occurring for all between 1 and 5 years after surgery. No recurrences were found after 5 years in the BHSR group. No significant statistical difference was found when comparing recurrence rates between the 2 groups (before the 5-year follow-up, P = .2; after the 5-year follow-up, P > .9) or persistent apprehension at 5 years (Lt: 6/34 [18%]; BHSR: 10/34 [29%]; P = .25).
Return to Sports
After surgery, RTS was higher at 1 year in the Lt group, (Lt: 28 [82%]; BHSR: 21 [62%]; P = .048), with more patients having returned to the same sport (Lt:27 [79%] vs BHSR: 6 [18%]; P = .01) and at the same level (Lt: 24 [71%] vs BHSR: 3 [9%]; P = .007). Those differences were no longer significant at 5 years (P = .28). When patients changed sport type postoperatively, the reason was independent of the shoulder involved for all of them in the Lt group (100%). On the contrary, in the BHSR group, the involved shoulder was the cause of sport change in 7 cases (21%)—2 cases (33%) due to stiffness, especially in external rotation at 90° of abduction, 1 case (16%) due to persistent pain, and 4 cases (66%) due to persistent apprehension (P < .001).
Complications and Reoperation
Two early complications (5.9%) were reported in the Lt group: 1 immediate hematoma was evacuated, and 1 bone block required revision (repositioning and refixation of the index graft) for displacement that occurred in a traumatic context without recurrent instability (P = .49).
Because of recurrent instability, 1 patient underwent arthroscopic Bankart repair in the Lt group (3%), and 4 patients underwent Latarjet procedures in the BHSR group (12%) (P = .35).
Radiological Analysis
No preoperative arthritis was observed. The analysis showed signs of degenerative arthritis in 7 patients (21%) in the Lt group (grade 1: n = 6; grade 2: n = 1) and 1 patient (grade 1 [3%]) in the BHSR group (P = .054) at the final follow-up.
Discussion
This matched-control study reported similar scores for most outcome measures at a minimum 5-year follow-up after Lt or arthroscopic BHSR to treat anterior shoulder instability. However, RTS at the same level was higher at 1 year after Lt. Failure to resume sport was more often due to the shoulder involved in the BHSR group. There was no significant difference in recurrence rates between the 2 procedures.
To date, without any consensus established, the choice of a suitable surgical technique depends on a multifactorial analysis of a patient’s characteristics (age, sex, hyperlaxity, occupation, and sports) and bipolar bone loss assessment. 5 Several other studies have compared Latarjet to arthroscopic remplissage, but only a few have had precise and similar bone loss assessment.1,15,22,27,29,30,34 Preoperative CT scans that we used seem to be highly recommended for bone loss evaluation, and therefore, avoid any bias in patient selection. 4 The glenoid track concept, which takes into account the engagement of the Hill-Sachs lesion, would provide another option; nonetheless, it remains exposed to criticism without any automated software. 33
In a systematic review published in 2020, Gouveia et al 22 found similar functional results between the 2 procedures, with a trend toward more complications for the bone block techniques, and a higher recurrence rate after Hill-Sachs remplissage in case of a glenoid bone loss of >10%. However, the compared studies included various bone block procedures (coracoid, iliac, or tibial), a large range of bone loss (up to 25%), and no precise data regarding the humeral bone defect. This limits the ability to clinically interpret these findings to define the best surgical strategy for a given patient. Still without matching for bone loss, similar results were found by Paul et al 34 in a series of 43 patients, in addition to a higher persistence of apprehension after remplissage. In our study, the SSV score was also found to be significantly better in the Lt group, in contrast to the Rowe and Duplay scores. Similar outcomes to our study were reported recently by Charles et al, 14 when comparing Bankart repair with remplissage to Latarjet in both primary and revision settings. For a glenoid bone loss of >15%, Horinek et al 27 reported similar clinical outcomes, RTS, and satisfaction scores at a very short-term (2 years) follow-up in both techniques in a series of 47 patients. However, active external rotation was slightly favored over the Latarjet procedure. In our study, the similar ranges of motion found between the 2 procedures at the 5-year follow-up need to be balanced for the external rotation with the elbow at the side, given the initial higher hyperlaxity (>85°) occurrence in the BHSR group. This may suggest that there is indeed a slight external rotation deficit after a remplissage procedure, which has been reported to occur between −2° and −10° in the literature, and accounts for one of the main clinical limitations reported for arthroscopic BHSR procedures.7,11,37
In a meta-analysis, Griesser et al 23 reported a high risk of complications (30%), revisions (7%), and recurrences (3%) after an Lt procedure. In our series of Latarjet, there was only 1 early postoperative hematoma in addition to 1 mechanical failure with bone block migration. In the longer term, 1 revision for recurrent instability (3%) was performed. Revision surgery was only required for instability recurrence (14%) in the BHSR group, but the Lt group did not significantly differ from the BHSR group, possibly due to a limited sample size. This recurrence rate remains similar to the most recent data10,31,37 reported in the literature, with a rate ranging from 0% to 15%. In their series of 133 patients with more significant bone loss undergoing Bankart repair with remplissage, Cavalier et al 13 found a significant increase in recurrence risk correlated to glenoid bone loss (>10%) and age (>23 years). Moreover, it seems that soft tissue procedures in general had an increased failure rate with time in an unselected population, even over a 5-year follow-up. 42 Thus, it reinforced our choice to perform a matched-cohort analysis based on at least age and glenoid bone loss.
In a recent meta-analysis, Ahmed et al 2 demonstrated that, compared with isolated Bankart procedures, the addition of a remplissage decreased failure and revision rates and increased RTS at every level. In our study, worse results were found for the BHSR group at 1 year regarding RTS. Cavalier et al 13 also found that one-third of their study population failed to RTS at 4 years, including the same sport and level for athletes practicing high-risk sports, independent of a shoulder estimated clinically stable otherwise. In our study, the number of high-level athletes, however, especially in the Lt group, may represent a selection bias leading to this difference. In addition, persistent apprehension was the reason for failure to RTS in the BHSR group for 66% of patients. However, our study finding was no longer significant after 5 years of follow-up, with similar RTS rates between the 2 groups at the mid-term.
Strengths and Limitations
The main limitations of this study are its retrospective design and limited sample size. Unfortunately, the database did not allow for the construction of a BHSR group of >35 patients, as some centers always performed a Latarjet in case of anterior shoulder instability. However, the number of patients included remained similar to other studies on this subject.22,29 Moreover, there was a selection bias to perform Latarjet for competitive athletes that may have affected the RTS timeframe. Beighton scores were not calculated, and hyperlaxity was determined only on the external rotation measurement.
Nevertheless, to our knowledge, this study was the first to perform a comparison after matching on 5 criteria between arthroscopic BHSR and Lt. Quality was reinforced by a precise assessment of glenoid and humeral bone loss on CT for both groups, in addition to the fact that measurement was only performed by a single examiner. We determined the matching criteria based on the literature data; nonetheless, other criteria, such as the level of sports, could have also been discriminant. Lastly, external rotation restriction was evaluated using preoperative data and based on the prerequisite that range of motion was symmetrical. However, it would be more accurate to compare the opposite healthy side if we highlight that 1 procedure is more likely to cause stiffness.
Conclusion
In our matched cohort study, Lt and BHSR procedures had similar clinical outcomes in cases of minimal glenoid bone loss. However, a faster return to the same sport at the same level after an Lt in the early postoperative period was highlighted; nevertheless, this trend did not continue over 5 years. There was no statistical difference regarding recurrence rate between the 2 groups. Degenerative arthritis remained worrisome after Lt and should be evaluated in a larger cohort with a longer follow-up time.
Footnotes
Final revision submitted March 14, 2025; accepted March 31, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: N.B. has received royalties from SBM and Move Up; and consulting fees from Conmed, SBM, and Move Up. L.N. has received royalties from Stryker and consulting fees from Stryker and Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the ethics committee CPP Ile de France VI (2022-A00373-40)