
Abstract
Background:
Differences in shoulder range of motion (ROM), shoulder muscle strength, and humeral torsion between left- and right-handed high school baseball pitchers remain poorly characterized.
Hypothesis:
Similar differences in shoulder ROM, strength, and humeral torsion between right-handed pitchers (RHPs) and left-handed pitchers (LHPs) observed in professionals will also be present in high school pitchers, with potential variations due to developmental stages.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
The authors included 921 high school baseball pitchers (706 RHPs and 215 LHPs) and evaluated their age, height, weight, body mass index, baseball experience, shoulder ROM, and muscle strength. Humeral torsion was measured in 211 RHPs and 57 LHPs. The Mann-Whitney U test was performed to determine the differences between the RHPs and LHPs and between the dominant and nondominant sides in each group. Pearson correlation analysis was performed to test the relationship between humeral torsion and shoulder ROM. Logistic regression analysis was conducted to determine the independent factors associated with LHP.
Results:
LHPs exhibited increased nondominant external rotation (ER) (103.1° vs 100.0°; P = .004), dominant horizontal adduction (HA) (23.0° vs 19.6°; P = .015), and side-to-side ratio in prone internal rotation (PIR) strength (107.6% vs 98.3%; P < .001) compared with RHPs. Additionally, LHPs were shorter (171.4 vs 172.9 cm; P = .002) with lower side-to-side differences in ER (5.7° vs 8.9°; P < .001) and HA (–6.5° vs −11.3°; P < .001), dominant prone ER (PER) strength (15.4 vs 16.8 kgf; P = .040), side-to-side ratio in PER strength (93.1% vs 103.7%; P < .001), and side-to-side differences in humeral torsion (5.8° vs 9.9°; P = .011) compared with RHPs. After adjusting for confounding factors, a smaller side-to-side ratio in PER strength (P < .001; OR, 0.911) and larger side-to-side ratio in PIR strength (P < .001; OR, 1.031) were independent factors associated with being an LHP.
Conclusion:
LHPs have a decreased side-to-side ratio in PER strength and increased side-to-side ratio in PIR strength compared with RHPs. These findings suggest that shoulder-related biomechanical differences between right- and left-handed pitchers are evident in high school athletes.
Throwing is one of the most demanding baseball activities. Repeated throwing motions can lead to structural adaptations of the shoulder joint, including changes in the range of motion (ROM) and humeral retroversion.1,10
Previous studies have demonstrated that baseball players’ throwing shoulder (referred to as the dominant shoulder) exhibits greater external rotation (ER) and reduced internal rotation (IR) compared with the nonthrowing (nondominant) shoulder.10,14,24 Additionally, the dominant arm in baseball players exhibits greater humeral retroversion than the nondominant arm. 14 However, studies on the differences in shoulder motion and humeral torsion between right- and left-handed baseball pitchers remain limited.
Existing research on professional baseball pitchers has shown that left-handed pitchers (LHPs) exhibit significantly reduced shoulder ER in their throwing arms compared with right-handed pitchers (RHPs). 7 While LHPs demonstrated significantly greater limitations in shoulder flexion ROM in their throwing arms than RHPs, 7 RHPs showed significant side-to-side differences in humeral retrotorsion, whereas LHPs did not exhibit this asymmetry. 7
A study on collegiate baseball pitchers has indicated the absence of statistically significant differences in the pitching arm ER or total ROM between RHPs and LHPs. 18 However, LHPs exhibited significantly higher pitching arm IR compared with RHPs. 18 In a study on young baseball pitchers (age, 9-12 years), the RHP group demonstrated significantly higher ER and humeral torsion angle in their throwing than in their nonthrowing arms. 20 Conversely, the LHP group exhibited no significant side-to-side differences in ER and humeral torsion angle. 20 Compared with the RHP group, the LHP group exhibited significantly smaller side-to-side differences in humeral torsion angle and reduced side-to-side ER differences. 20 These findings suggest that the adaptations in shoulder joint ROM and humeral torsion may be different between RHPs and LHPs in different age groups. However, to our knowledge, the differences between high school RHPs and LHPs remain ill-defined. Additionally, differences in elbow ROM and shoulder muscle strength between RHPs and LHPs have not been investigated in any age group. Therefore, we aimed to investigate the differences in shoulder and elbow ROM, shoulder strength, and humeral torsion angle between the dominant and nondominant arms of high school RHPs and LHPs. We hypothesized that similar differences in shoulder ROM, strength, and humeral torsion between RHPs and LHPs observed in professionals would also be present in high school pitchers, with potential variations due to developmental stages.
Methods
Study Population
This retrospective study included high school baseball pitchers who participated in annual preseason medical checkups conducted in February. Data from preseason medical checkups over a 7-year period (2012-2018) were analyzed. No player participated in multiple years of preseason medical checkups during the study period. Each player was included in the analysis only once, ensuring that all participants are unique.
The study included data from high school baseball pitchers who actively practiced during the preseason and had no limitations on their pitching. 15 Data were excluded if participants had previously injured their throwing arm or were unable to play baseball because of shoulder or elbow issues. 15 The study was approved by our institutional review board, and all procedures were carried out in accordance with applicable guidelines and regulations. Written informed consent was obtained from the parents of all participants.
Preseason Medical Checkups
As reported in previous studies,15-17 preseason medical checkups were performed to assess the participants’ shoulder and elbow status. To avoid bias, the examiners were unaware of the participants’ handedness. The assessments included measuring the participants’ age, body weight, height, body mass index (BMI), baseball history, shoulder and elbow ROM, shoulder muscle strength, and humeral torsion. 25 We used previously established assessment methods for ROM,15-17 shoulder strength,15-17 and humeral torsion. 25
Shoulder and Elbow ROM
According to previous studies,15-17 a certified orthopaedic surgeon used a digital protractor (iGaging) to assess the passive ROM for elbow flexion and extension, as well as the abduction-ER, abduction-IR, and passive horizontal adduction (HA) of the dominant and nondominant shoulders. All measurements were obtained with the participants in the supine position. To measure HA, one certified orthopaedic surgeon (F.I.) stabilized the axillary border of the scapula, and another surgeon (R.M.) placed a digital protractor on the humerus. To measure ER and IR, one certified orthopaedic surgeon (F.I.) applied a posterior force to the coracoid process to stabilize the scapula, and another surgeon (R.M.) placed a digital protractor on the forearm. The total arc for each shoulder was calculated by adding the ER and IR measurements. The difference in each ROM measurement was determined by subtracting the value of the nondominant side from that of the dominant side. In addition to evaluating the dominant (throwing) shoulder, we also assessed the nondominant shoulder to examine potential side-to-side asymmetries. This approach is consistent with previous studies,7,18,20,21 which included both shoulders to provide a more comprehensive understanding of the biomechanical adaptations that occur in baseball players. Side-to-side differences can highlight important asymmetries that may influence injury risk and performance.
Shoulder Strength
According to previous studies,2,15-17 a certified orthopaedic surgeon evaluated the strength of the supraspinatus in the seated position (SS), prone ER (PER), and prone IR (PIR) in both shoulders using a PowerTrack II Commander handheld dynamometer (J-Tech Medical) (Figure 1). SS strength was evaluated with the participants seated on an examination table with their backs against the wall. The participant first abducted the humerus to 90° in the coronal plane and then adducted it horizontally to 45°, with the forearm in a neutral position. The handheld dynamometer was placed 5 cm proximal to the proximal wrist extension crease, and the participants were instructed to raise their arms. To measure the PER strength, a handheld dynamometer was positioned on the dorsal aspect of the forearm, 5 cm proximal to the wrist extension crease. PIR strength was measured in a similar manner; however, the dynamometer was placed on the volar aspect of the distal radius, 5 cm proximal to the proximal wrist flexion crease, as the participant internally rotated their arm with maximum power. Strength measurements were obtained 3 times for each participant, and the median value was used for the analysis. The SS, PER, and PIR strength ratios of the dominant to the nondominant arms were calculated for each participant and expressed as percentages.

Measurement strengths of prone external rotation (PER) and prone internal rotation (PIR) in the shoulders.
Humeral Torsion
Humeral torsion was assessed using an indirect ultrasonographic method, as previously described.12,23 All measurements were performed by a certified orthopaedic surgeon (T.T.) who had received >5 years training and had experience with orthopaedic ultrasound procedures. As previously reported, 25 the examiner positioned a multifrequency 12-MHz linear array transducer (LOGIQ e; GE HealthCare) with a standard coupling gel on the participant's anterior shoulder. The transducer was positioned perpendicularly to the horizontal plane, as confirmed by the bubble level. The examiner passively rotated the participant's humerus until the bicipital groove was centered in the ultrasound image, with the line connecting the peaks of the greater and lesser tubercles aligned parallel to the horizontal plane. Finally, the angle between the forearm and horizontal plane was measured using a digital inclinometer.
Statistical Analysis
Continuous data are reported as mean ± standard deviation, and group differences were assessed using the Mann-Whitney U test. We used logistic regression analysis to account for potential differences between right- and left-handed pitchers, including group size imbalances. Logistic regression allows us to adjust for variability and identify independent factors associated with handedness while controlling for confounding variables. This approach ensures that, despite the larger number of RHPs, the statistical analysis provides a robust comparison between the groups. For logistic regression analysis, explanatory variables were selected based on P values from the univariate analysis using a cutoff of P < .05. Multicollinearity among the independent variables was evaluated using variance inflation factors (VIFs), with a value >3 indicating multicollinearity. Lastly, logistic regression analysis was conducted to determine the independent factors associated with being an LHP and to calculate the corresponding odds ratios and 95% confidence intervals. All statistical analyses were conducted using the IBM SPSS Statistics Version 29 software program (IBM Japan, Ltd), with a significance level of P < .05. Prism Version 8 (GraphPad Software) was used to perform Pearson correlation analysis to investigate the relationship between humeral torsion and ER/IR differences and to generate Figures 2 and 3.

Relationship between differences in humeral torsion and external rotation (ER). LHP, left-handed pitcher; RHP, right-handed pitcher.

Relationship between differences in humeral torsion and internal rotation (IR). LHP, left-handed pitcher; RHP, right-handed pitcher.
Results
This study included 921 high school baseball pitchers between 2012 and 2018, including 706 RHPs and 215 LHPs. Humeral torsion data were collected only during the 2014 and 2015 seasons, yielding 268 measurements from 211 RHPs and 57 LHPs.
Baseline Characteristics
The RHPs were significantly taller than the LHPs, with mean heights of 172.9 cm and 171.4 cm, respectively (P = .002). However, the 2 groups did not differ significantly in age, weight, BMI, or baseball experience (Table 1).
Characteristics of Right- and Left-handed High School Pitchers a

Bold P value indicates statistical significance. BMI, body mass index; LHP, left-handed pitcher; RHP, right-handed pitcher.
Comparison of Shoulder ROM, Shoulder Strength, and Humeral Torsion Between RHPs and LHPs
Laterality Effect (RHPs vs LHPs)
Our findings are summarized in Table 2. LHPs demonstrated significantly higher values of nondominant shoulder ER (103.1° vs 100.0°; P = .004) and dominant shoulder HA (23.0° vs 19.6°; P = .015) than RHPs. The dominant PER strength of LHPs was significantly lower than that of RHPs (15.4 vs 16.8 kgf; P = .040). Regarding the ROM differences or strength ratios between dominant and nondominant arms, the LHPs exhibited significantly smaller differences for shoulder ER (5.7° vs 8.9°; P < .001), shoulder HA (–6.5° vs −11.3°; P < .001), PER strength ratio (93.1% vs 103.7%; P < .001), and humeral torsion (5.8° vs 9.9°; P = .011) than RHPs. The PIR ratio was significantly higher in LHPs than in RHPs (107.6% vs 98.3%; P < .001). There were no significant differences in other ROM measurements or strength ratios between the 2 groups.
Comparison of Shoulder ROM, Shoulder Strength, and Humeral Torsion Between Right- and Left-handed Pitchers a

Bold P values indicate statistical significance. Dom, dominant throwing arm; ER, external rotation; HA, horizontal adduction; IR, internal rotation; LHP, left-handed pitcher; NDom, nondominant arm; PER, prone external rotation; PIR, prone internal rotation; RHP, right-handed pitcher; SS, seated supraspinatus.
Difference is defined as the Dom minus the NDom.
Total arc is defined as the sum of the ER and IR values.
Ratio is defined as the Dom divided by the NDom multiplied by 100.
Dominance Effect (Dominant vs Nondominant) in LHPs
The dominant shoulder ER (108.8° vs 103.1°; P < .001), PIR strength (19.1 vs 17.8 kgf; P < .001), and humeral torsion (75.0° vs 69.2°; P < .001) in LHPs were significantly higher than in their nondominant sides (Table 2). By contrast, LHPs exhibited significantly lower dominant shoulder IR (42.1° vs 50.3°; P < .001), shoulder HA (23.0° vs 29.6°; P < .001), and PER strength (15.4 vs 16.8 kgf; P < .001) compared with their nondominant sides. No significant differences were observed in LHPs between dominant and nondominant shoulders in shoulder total arc of motion and SS strength.
Dominance Effect (Dominant vs Nondominant) in RHPs
The dominant shoulder ER (108.9° vs 100.0°; P < .001), PER strength (16.8 vs 16.2 kgf; P < .001), SS strength (14.7 vs 14.5 kgf; P = .043), and humeral torsion (78.0° vs 68.2°; P < .001) in RHPs were significantly higher than in their nondominant sides (Table 2). By contrast, RHPs exhibited significantly lower dominant shoulder IR (43.0° vs 51.9°; P < .001), shoulder HA (19.6° vs 30.9°; P < .001), and PIR strength (18.4 vs 18.9 kgf; P < .001) compared with their nondominant sides. No significant differences were observed in RHPs between dominant and nondominant shoulders in shoulder total arc.
Correlation Between Humeral Torsion and Shoulder ROM
In the entire cohort, humeral torsion difference was significantly correlated with ER difference (r = 0.190; P = .002) (Figure 2). However, no significant correlation was found (r = 0.105; P = .086) between the degree of side-to-side torsion and IR difference (Figure 3).
Logistic Regression Analysis
Based on the results of the univariate analysis for the laterality effect (RHPs vs LHPs), height, nondominant-side ER, ER difference, dominant-side HA, HA difference, dominant-side PER strength, PER ratio, PIR ratio, and humeral torsion difference were selected as candidate explanatory variables in the multivariate logistic regression analysis. To evaluate the VIFs, we performed multicollinearity analysis, and the results showed that no variables had a VIF >3, indicating no pronounced multicollinearity. The final logistic regression analysis model showed that a lower PER ratio (P < .001; OR, 0.911; 95% CI, 0.885-0.939) and higher PIR ratio (P < .001; OR, 1.031; 95% CI, 1.013-1.049) were independent factors associated with being an LHP (Table 3).
Results of the Logistic Regression Analysis a

Bold P values indicate statistical significance. ER, external rotation; HA, horizontal adduction; PER, prone external rotation strength; VIF, variance inflation factor.
Difference is defined as the Dom minus the NDom.
Ratio is defined as the Dom divided by the NDom multiplied by 100.
Discussion
The main findings of this study were that high school LHPs in our cohort had significantly higher nondominant ER, dominant HA, and side-to-side ratio in PIR strength compared with RHPs. Additionally, LHPs were significantly shorter and exhibited lower side-to-side differences in ER and HA, dominant PER strength, side-to-side ratio in PER strength, and side-to-side differences in humeral torsion than RHPs. After adjusting for confounding factors, a lower side-to-side ratio in PER strength and a higher side-to-side ratio in PIR strength were found to be independent factors associated with being an LHP. To the best of our knowledge, this is the first study to identify specific factors for LHPs among high school baseball pitchers. Studying high school athletes, who are still in the process of physical development, is crucial for understanding how shoulder biomechanics change with growth. The mean age of 16.5 years reflects a critical period in which athletes are still maturing. Our findings should be interpreted in the context of developmental differences across various age groups, as comparisons were made not only with older, more developed athletes (eg, professional pitchers) but also with younger, less developed players. These comparisons highlight the dynamic changes in physical characteristics and performance metrics that occur throughout the stages of athletic development. These findings can serve as a reference for the implementation of age-specific training and injury prevention strategies.
LHP and RHP Height and Weight
Previous studies have shown that LHPs are significantly shorter and lighter than RHPs among professional baseball pitchers3,5 and cricketers in England. 13 However, other studies have shown that there were no significant differences in height and weight between left- and right-handed baseball players in college or amateur teams 19 and young players aged 9 to 12 years. 20 In the present study, high school LHPs were found to be significantly shorter than RHPs, despite no significant weight difference between the 2 groups.
One possible explanation for these findings is the positional specialization in baseball. Left-handed players are often steered toward playing pitcher, first base, or outfield, where their handedness can offer strategic advantages. In contrast, right-handed players have more positional flexibility, which could result in different physical demands and anthropometric profiles being selected for other positions. Additionally, these differences might reflect the natural variation in physical maturation and development across different age groups or the inclusion of nonpitcher players in certain cohorts.
Our findings align with those of previous studies; however, inconsistencies remain. The reasons for these discrepancies could also be attributed to variations in the study cohorts, such as differences in age, developmental stages, or the specific inclusion criteria for players. Further research is required to better understand these trends and the factors driving positional and anthropometric differences among left- and right-handed players.
Differences in Shoulder ROMs Between LHPs and RHPs
Studies have indicated significant differences in shoulder ROMs between the LHPs and RHPs (Table 4).
Comparison of Current Results and Previous Studies in Shoulder ROMs a

Bold P values indicate statistical significance. Diff, difference; ER, external rotation; IR, internal rotation; LHP, left-handed pitcher; NDom, nondominant arm; RHP, right-handed pitcher. Dashes indicate P > 0.05.
Difference is defined as the Dom minus the NDom.
Total arc is defined as the sum of ER and IR values.
Shoulder ER
Previous studies have shown that there was no difference in the dominant shoulder ER between LHPs and RHPs in collegiate18,21 and youth 20 pitchers. However, Harris et al 7 found that LHPs had significantly smaller dominant shoulder ER compared with RHPs in professional baseball pitchers. Consistent with some prior studies on collegiate18,21 and youth 20 pitchers, the present study found no significant difference in dominant shoulder ER between LHPs and RHPs. By contrast, previous studies have demonstrated that LHPs have significantly higher nondominant shoulder ER than RHPs among professional 7 and collegiate 21 pitchers. These findings are in agreement with the current study. Conversely, no difference in nondominant shoulder ER between LHPs and RHPs was observed in previous studies of youth 20 and collegiate 18 pitchers. The current study revealed a significantly smaller side-to-side difference in shoulder ER between dominant and nondominant sides in LHPs than in RHPs, which is consistent with the previous study of youth pitchers. 20
One possible explanation for the ER differences observed in professional pitchers but not in younger players is the cumulative effect of repetitive throwing. Professional pitchers have a longer pitching history and higher throwing volume, leading to adaptive changes in shoulder structures over time. In contrast, younger players may not have developed these adaptations due to their shorter exposure to high-intensity throwing. Additionally, younger athletes often engage in multiple sports, reducing the repetitive stress on the shoulder compared with professional pitchers, who undergo intense, position-specific training. These factors could explain why ER differences emerge only at the professional level.
Shoulder IR
Previous studies have revealed no differences in the dominant and nondominant shoulder IR between LHPs and RHPs in collegiate 21 and youth 20 pitchers. However, other studies found that LHPs had significantly greater dominant and nondominant shoulder IR compared with RHPs in professional 7 and collegiate 18 pitchers. Consistent with prior studies on collegiate 21 and youth 20 pitchers, here we found no significant difference in dominant shoulder IR between LHPs and RHPs. In contrast to previous studies on professional pitchers 7 that found that LHPs exhibited smaller side-to-side differences in shoulder IR compared with RHPs, our work revealed that LHPs had no significant side-to-side difference in shoulder IR between their dominant and nondominant sides compared with RHPs.
Once again, a possible explanation for the differences observed in professional pitchers is the cumulative effect of repetitive throwing over longer careers. Professional pitchers may develop adaptive changes, such as increased capsular laxity or muscular flexibility, due to prolonged high-intensity throwing. In contrast, younger pitchers, with less exposure to repetitive stress and specialization, may not exhibit such adaptations. Additionally, differences in training focus or mechanics between age groups could contribute to these discrepancies.
Shoulder Total Arc
Previous studies have revealed no differences in the dominant and nondominant shoulder total arc between LHPs and RHPs in professional 7 and collegiate 18 pitchers. Consistent with these studies, we found no significant difference in the dominant shoulder total arc between LHPs and RHPs.
It is important to distinguish between the total arc in individual shoulders (dominant or nondominant) and the side-to-side differences in total arc between the dominant and nondominant shoulders. While previous studies demonstrated that LHPs exhibited greater side-to-side differences in shoulder total arc compared with RHPs, 7 our work revealed that LHPs had no significant side-to-side difference in total arc between their dominant and nondominant sides compared with RHPs. These findings suggest that, while the total arc of individual shoulders may not differ significantly between LHPs and RHPs, the way these arcs differ between the dominant and nondominant sides may vary depending on the cohort or competitive level.
Shoulder HA
No previous study has examined the differences in shoulder HA ROM between LHPs and RHPs. The present study indicated that LHPs had significantly higher dominant shoulder HA and lower side-to-side differences in shoulder HA than RHPs. A previous biomechanical study on pitching mechanics between LHPs and RHPs suggested that the former exhibit less HA from foot contact through ball release than the latter, suggesting that LHPs maintain their throwing arm in a different orientation and alignment compared with RHPs. 18 Also, a previous biomechanical study performed during pitching showed that the peak angular speed of shoulder HA was lower for LHPs compared with RHPs. 21 The higher dominant shoulder HA and smaller side-to-side HA differences observed in LHPs may be related to lower shoulder HA stress during pitching. Previous research has associated increased shoulder HA and peak shoulder HA angular velocity with elevated shoulder distraction stress in collegiate pitchers. 22 Therefore, the differences in shoulder HA characteristics found for LHPs in our study suggest they may experience reduced shoulder distraction stress compared with RHPs. However, no study comparable to the current one has been published to date, and further research is required.
Differences in Humeral Torsion Between LHPs and RHPs
Previous studies have reported conflicting results regarding the differences in humeral torsion between LHPs and RHPs (Table 5).
Comparison of Humeral Torsion Between the Present and Previous Studies a
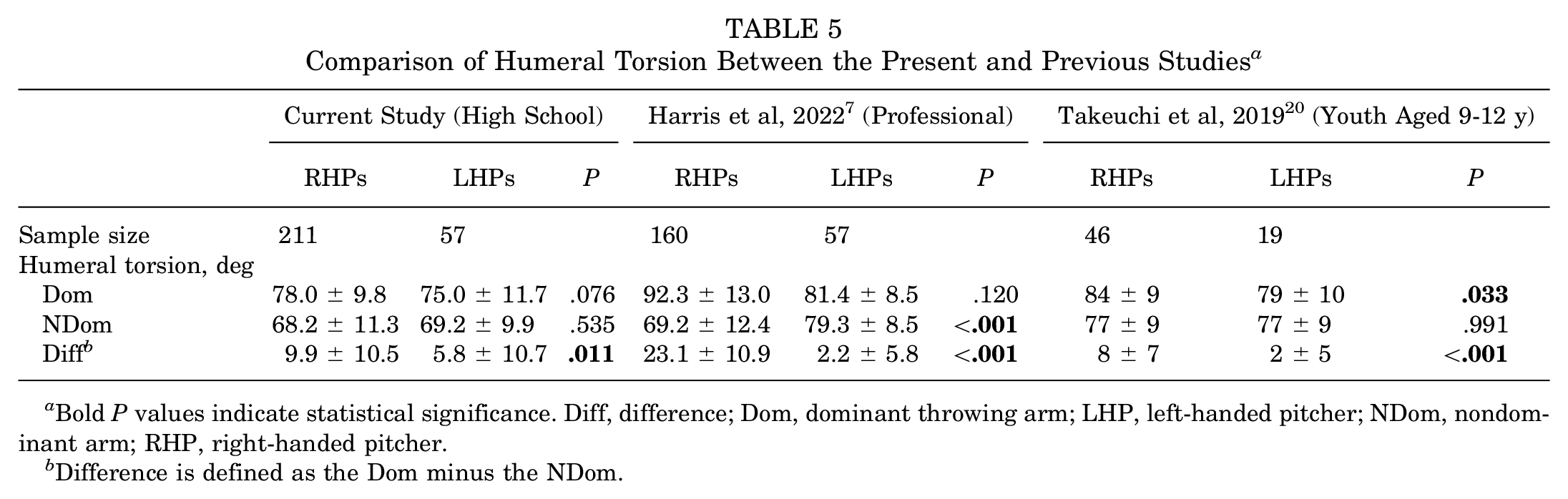
Bold P values indicate statistical significance. Diff, difference; Dom, dominant throwing arm; LHP, left-handed pitcher; NDom, nondominant arm; RHP, right-handed pitcher.
Difference is defined as the Dom minus the NDom.
Youth LHPs have significantly smaller dominant humeral torsion than RHPs, 20 but this difference has not been observed in professional pitchers. 7 Conversely, professional LHPs have been found to have significantly greater nondominant humeral torsion than RHPs, 7 although this difference was not observed in youth pitchers. 20 Additionally, both professional 7 and youth 20 LHPs have exhibited significantly smaller side-to-side differences in humeral torsion between their dominant and nondominant arms compared with RHPs. Here, we found no difference in humeral torsion between LHPs and RHPs regarding both their dominant and nondominant arms, which is partially consistent with previous research on professional 7 and youth 20 pitchers. Nevertheless, it revealed that LHPs had a significantly smaller difference in humeral torsion between their dominant and nondominant arms compared with RHPs, which is consistent with previous research on professional 7 and youth 20 pitchers.
Increased humeral torsion in professional pitchers has been demonstrated to be positively correlated with higher ER.4,7,11 Our study corroborated these findings, showing that increased humeral retrotorsion is associated with higher ER. Additionally, several studies have found associations between retrotorsion and decreased IR (glenohumeral IR deficit [GIRD])6-9; however, in the present study, there was no significant correlation between humeral torsion and GIRD, suggesting that factors other than humeral torsion may contribute to the development of GIRD in both LHPs and RHPs.
Differences in Shoulder Strength Between LHPs and RHPs
No previous studies have examined the differences in shoulder strength between LHPs and RHPs. In the present study, LHPs exhibited a significantly smaller dominant PER strength and side-to-side ratio in PER, as well as a greater side-to-side ratio in PIR strength, compared with RHPs. Furthermore, a smaller PER and a larger PIR ratio were identified as independent factors associated with LHP.
Limitations
Although our study provides valuable insights, it is limited by its cross-sectional design, which precludes causal inferences. Additionally, the focus on high school pitchers may limit the generalizability of our findings to other competitive levels. Furthermore, while we identified differences between left- and right-handed pitchers, there is likely a wide range of variability within the larger group of RHPs that may impact individual training and rehabilitation strategies. Another limitation is that we did not assess participants’ handedness beyond their throwing hand for everyday tasks, such as writing. A more detailed handedness assessment, such as the Edinburgh Handedness Inventory, could provide further insights. This is especially pertinent for LHPs, where the dominant hand for daily activities and the throwing hand may differ. Future studies should focus on more individualized assessments to account for this variability and develop tailored training approaches for all throwers, regardless of handedness. Longitudinal studies are also needed to examine the long-term effects of biomechanical differences on performance and injury outcomes. Future research should explore the underlying mechanisms driving these adaptations and their implications for training and rehabilitation.
Conclusion
To the best of our knowledge, this is the first study to comprehensively examine the differences in shoulder ROM, strength, and humeral torsion between high school LHPs and RHPs. LHPs have a decreased side-to-side ratio in PER strength and an increased side-to-side ratio in PIR strength compared with RHPs. Our findings suggest that shoulder-related biomechanical differences between right- and left-handed pitchers are evident in high school athletes.
Authors
Hitoshi Shitara, MD, PhD (Department of Orthopaedic Surgery, Gunma University Graduate School of Medicine, Gunma, Japan); Tsuyoshi Tajika, MD, PhD (Department of Orthopaedic Surgery, Gunma University Graduate School of Medicine, Gunma, Japan); Tsuyoshi Ichinose, MD, PhD (Department of Orthopaedic Surgery, Gunma University Graduate School of Medicine, Gunma, Japan); Tsuyoshi Sasaki, MD, PhD (Department of Orthopaedic Surgery, Gunma University Graduate School of Medicine, Gunma, Japan); Noritaka Hamano, MD, PhD (Department of Orthopaedic Surgery, Gunma University Graduate School of Medicine, Gunma, Japan); Masataka Kamiyama, MD (Department of Orthopaedic Surgery, Gunma University Graduate School of Medicine, Gunma, Japan); Ryosuke Miyamoto, MD (Department of Orthopaedic Surgery, Gunma University Graduate School of Medicine, Gunma, Japan); Kurumi Nakase, MD (Department of Orthopaedic Surgery, Gunma University Graduate School of Medicine, Gunma, Japan); Fukuhisa Ino, MD (Department of Orthopaedic Surgery, Gunma University Graduate School of Medicine, Gunma, Japan); Takuma Kachi, MD (Department of Orthopaedic Surgery, Gunma University Graduate School of Medicine, Gunma, Japan); Yuhei Hatori, MD (Department of Orthopaedic Surgery, Gunma University Graduate School of Medicine, Gunma, Japan); Koichiro Yanai, MD (Department of Orthopaedic Surgery, Gunma University Graduate School of Medicine, Gunma, Japan); Atsushi Yamamoto, MD, PhD (Department of Orthopaedic Surgery, Gunma University Graduate School of Medicine, Gunma, Japan), Kenji Takagishi, MD, PhD (Department of Orthopaedic Surgery, Gunma University Graduate School of Medicine, Gunma, Japan); and Hirotaka Chikuda, MD, PhD (Department of Orthopaedic Surgery, Gunma University Graduate School of Medicine, Gunma, Japan).
Footnotes
Acknowledgements
Final revision submitted December 6, 2024; accepted January 9, 2025.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Gunma University Hospital (No. 1003).