
Abstract
Background:
Active-duty military servicemembers (ADSMs) exhibit a high prevalence of combined-type shoulder instability. Arthroscopic 270° labral repair has demonstrated promising outcomes at short- and intermediate-term follow-up, but there is a paucity of long-term outcomes data among ADSMs.
Purpose:
To report the outcomes of arthroscopic 270° labral repair at a minimum of 10-year follow-up in ADSMs.
Study Design:
Case series; Level of evidence: 4.
Methods:
A total of 44 ADSMs who underwent arthroscopic 270° labral repair between January 2010 and December 2012 without major concomitant procedures had ≥10 years of follow-up and were deemed eligible for inclusion. Of these, 38 were included in the final outcome analysis.
Results:
Mean follow-up was 140.4 ± 14.4 months. Postoperatively, there was a statistically significant improvement in pain visual analog scale (VAS) scores (8.3 ± 1.3 to 1.63 ± 2.29; P < .0001) as well as American Shoulder and Elbow Surgeons (ASES) Standardized Shoulder Assessment (42.7 ± 12.3 to 87.3 ± 19.0; P < .0001), Single Assessment Numeric Evaluation (SANE) (49.5 ± 18.9 to 91.9 ± 11.3; P < .0001), and Rowe instability (45.3 ± 12.5 to 89.3 ± 19.2; P < .0001) scores. There were no significant differences observed between pre- and postoperative range of motion. At final follow-up, 95% of patients met the minimal clinically important difference threshold for VAS, 89% for ASES, 92% for SANE, and 92% for the Rowe score; 58% met the substantial clinical benefit threshold for VAS, 61% for ASES, 11% for SANE, and 74% for Rowe scores; and 74% met the Patient Acceptable Symptom State threshold for VAS, 76% for ASES, 76% for SANE, and 74% for Rowe scores. At final follow-up, 89.5% of patients (n = 34) either returned to unrestricted duty or left the military for reasons other than continued shoulder-related disability, while 86.8% (n = 33) returned to unrestricted physical training. Two patients (5.3%) underwent reoperation, one requiring revision anterior labral repair and the other Latarjet after a traumatic dislocation of the operative shoulder.
Conclusion:
Arthroscopic 270° labral repair demonstrates favorable clinical outcomes at a minimum 10-year postoperative follow-up in an active-duty military patient population, with clinically and statistically significant improvements in pain, patient-reported outcomes measures, and an overall return-to-duty rate of 89.5%.
Glenohumeral instability represents a significant source of injury and impairment among active-duty servicemembers (ADSMs) in the United States.7,8,12 Compared with their civilian counterparts, ADSMs experience higher rates of recurrent shoulder instability,6,9,16,17,20 with disproportionate representation of multidirectional instability.1,17,23,24 Multidirectional shoulder instability is classically difficult to diagnose; furthermore, 270° labral tears, which span from the anterior and inferior labrum to the posterior aspect of the midglenoid and spare the superior labrum and biceps anchor, are notoriously difficult to diagnose and treat.14,19
Over the past 2 decades, arthroscopic labral repair has replaced open inferior capsular shift or capsular plication for the treatment of 270° labral tears.2,3,11,15 Promising short-term outcomes have been observed among civilian patient populations regarding return to activity and recurrence; however, long-term reported outcomes are limited to civilian cohorts alone.4,13,14,18,20 Due to the unique shoulder burden implicated in active-duty military service and heightened baseline risk of multidirectional instability, understanding long-term outcomes among the ADSM population after 270° arthroscopic labral repair offers significant value in predicting sustained return to duty and overall patient-reported outcome (PRO) measures (PROMs) in a high-demand population.
The purpose of this study is to investigate the clinical outcomes and return-to-duty rates after arthroscopic 270° labral repair among a cohort of active-duty military patients with ≥10 years of follow-up.
Methods
Study Design
This study is a retrospective analysis of prospectively collected data investigating long-term PROs and range of motion (ROM) after arthroscopic 270° labral repair. All patients undergoing arthroscopic 270° labral repair between January 2010 and December 2012 were considered eligible for inclusion. Patients with nontraumatic hyperlaxity and anterior or posterior glenoid bone loss >20% were excluded from analysis. Patients undergoing concomitant procedures, such as rotator cuff repair, glenoid microfracturing, and superior labrum anterior to posterior (SLAP) repair at the time of their index 270° labral repair were also excluded from analysis. Patients who required revision surgery after their index procedure were included as treatment failures but excluded from PRO and ROM analysis to establish the efficacy of arthroscopic 270° labral repair in patients who do not fail treatment. Institutional review board approval was obtained and the reporting of our findings adheres to the Strengthening the Reporting of Observational Studies in Epidemiology recommendations.
Patient Selection
All patients were ADSMs at time of injury and at surgical intervention. In-office physical examination was used to initially examine the amount and direction of instability. Preoperative magnetic resonance arthrogram (MRA), using a 1.5-Tesla magnet, was obtained for all patients. After an in-office assessment and review of diagnostic imaging, patients who were deemed candidates for arthroscopic 270° labral repair were indicated for surgery by the operative surgeon and elected to proceed.
Surgical Procedure
All procedures were performed by the senior author, a shoulder and elbow fellowship-trained orthopaedic surgeon (N.P.). The patient was placed in the beach-chair position using a Spider Limb Positioner (Smith & Nephew). After the induction of general anesthesia but before initiation of diagnostic arthroscopy, an examination under anesthesia was performed to determine the extent of anterior, posterior, and inferior laxity. After the examination under anesthesia, a 30° arthroscope was introduced into the glenohumeral joint via a standard posterior portal. An anterior portal was established low in the rotator interval region. A diagnostic arthroscopy was then performed, and associated intra-articular abnormalities were documented and addressed as indicated. Then, with use of a probe, the labrum was assessed to determine the presence and extent of tearing. Patients were diagnosed with a 270° labral tear when the tear extended from the anteroinferior labrum posteriorly and superiorly to the superior labrum (eg, from 9 o’clock to 12 o’clock for a left shoulder).
Once the presence of a 270° labral tear was verified, a trans–rotator cuff portal was created medial to the rotator cuff cable using a spinal needle as described by Costouros et al. 5 Capsulolabral repair was then performed with double-loaded Gryphon BR biocomposite suture anchors (DePuy Mitek). All knots tied, regardless of the anchor used, were cinch knots.
Subacromial bursectomy and decompression with acromioplasty were routinely performed in all cases, both for visualization and symptomatic management.
With regard to concomitant procedures, subpectoral biceps tenodesis was performed for patients who had tearing of the labrum at the biceps anchor (SLAP) tear. All patients who underwent biceps tenodesis also had preoperative point tenderness to deep palpation in the bicipital groove and a positive Speed, Yergason, and O’Brien test findings and/or pathology noted to the long head of the biceps tendon on arthroscopic evaluation. Acromioclavicular joint resection was performed for patients who had preoperative point tenderness over the acromioclavicular joint and/or a positive cross-body test finding. Remplissage was performed for patients with an off-track Hill-Sachs lesion, and the decision to proceed with remplissage was made preoperatively based off of MRA. 10 At the end of the procedure, adequacy of the repair site was confirmed using a probe. Portal sites were closed using 3-0 nylon sutures. A sterile dressing was applied, and the patient’s arm was placed in a neutral rotation sling.
Postoperative Rehabilitation
The postoperative protocol consisted of immobilization in neutral rotation for 6 weeks, with initiation of formal physical therapy within 2 weeks. Early distal ROM exercises involving the elbow, wrist, and hand were initiated immediately. Passive ROM of the shoulder was started during the first 2 weeks postoperatively, with a gradual progression of forward flexion (FF) from 90° to 150° over 6 weeks. Horizontal adduction and internal rotation (IR) were avoided for the first 10 weeks to protect the posterior capsulolabral repair site. External rotation (ER) was limited to 30° for the first 6 weeks to protect the anterior repair site. Active ROM of the shoulder was initiated at 6 to 8 weeks. A progressive strengthening program was initiated at 12 weeks. Return to unrestricted military activities, including vigorous sports, was permitted at 6 months postoperatively with physician clearance.
PRO Measures
PROM scores collected included the pain visual analog scale (VAS), American Shoulder and Elbow Surgeons (ASES) Standardized Shoulder Assessment, Single Assessment Numeric Evaluation (SANE), and Rowe instability score (Rowe). ROM values included FF, ER measured with the arm at the side in neutral rotation, and IR measured at the highest vertebral level reached by the patient’s thumb. The present study’s patient cohort represents a similar population to that described by Scanaliato et al, 21 which also examined outcomes among ADSMs undergoing 270º labral repair; subsequently, values for the minimal clinically important difference (MCID), substantial clinical benefit (SCB), and Patient Acceptable Symptom State (PASS) as described by Scanaliato et al 21 were used to evaluate the clinical significance of PROMs in our cohort.
Statistical Analysis
Statistical analyses were conducted using SPSS Statistics (Version 25.0; IBM). Continuous data were described as the mean ± SD. Paired t tests were used to evaluate differences between preoperative and postoperative measures. Chi-square tests were used to analyze categorical variables. Statistical significance was set at P < .05 in all cases.
Results
A group of 59 patients underwent 270° labral repair by the senior author within the study inclusion window with a mean follow-up of 140.4 ± 14.4 months (Figure 1). Of these, 15 underwent concomitant surgical intervention at the time of their index procedure and were excluded from analysis: 5 for concomitant rotator cuff repair, 4 for concomitant debridement and microfracturing of glenoid osteochondral defect, and 6 for concomitant SLAP repair. Of the remaining 44 patients eligible for inclusion after their index procedure, 2 patients were excluded for further operative intervention after their index procedure: 1 for anterior labral repair revision and 1 for revision to a Latarjet after a traumatic dislocation of the operative shoulder. An additional 4 patients were lost to follow-up. Ultimately, of the initial 59 patients, 44 (74.6%) were not excluded for concomitant procedures and 38 (86.4%) of the 44 were ultimately included in the final outcome analysis.

Patient inclusion flowchart. SLAP, superior labrum anterior to posterior.
Patient Demographics and Preoperative Characteristics
The mean age of patients in this cohort at the time of surgery was 28.5 ± 7.8 years (Table 1). The dominant shoulder was implicated in 55.3% of cases. Of total patients included, 63% were infantrymen, which is considered a heavy physical demand military occupation (Tables 1 and 2). All patients included were male. Preoperative physical examination demonstrated anterior apprehension in 76.3% of patients (n = 29) and posterior apprehension in 65.8% (n = 25) of patients. Preoperative MRA demonstrated isolated anterior labral pathology in 23.7% (n = 9), isolated posterior labral pathology in 21.1% (n = 8.0), and combined pathology in 31.6% (n = 12) of patients, while no pathology was identified on preoperative imaging in 23.7% of patients (n = 9).
Patient Demographics a

Data are reported as n (%) or mean ± SD. MRA, magnetic resonance arthrogram.
Military Occupations a

Data are presented as n (%).
Operative Characteristics
The mean duration of surgery was 94.3 ± 28.3 minutes. All patients underwent a concomitant subacromial bursectomy, 6 patients (15.8%) underwent concomitant biceps tenodesis/tenotomy, 4 patients (10.5%) underwent concomitant arthroscopic acromioclavicular reconstruction, 4 patients (10.5%) underwent concomitant remplissage, and 2 patients (5.3%) underwent concomitant rotator cuff debridement (Table 1). On average, 4.0 ± 0.96 anchors were used in 270° labral repair.
Range of Motion
No statistically significant difference was appreciated in postoperative ROM measurements, with postoperative mean FF of 154.7°± 11.1° compared with preoperative mean FF of 155.0°± 9.2° (P = .9108), postoperative mean ER of 64.2°± 6.9° compared with preoperative mean ER of 67.0°± 6.0° (P = .0669), and postoperative mean IR of 9.8°± 2.5° compared with preoperative mean IR of 9.5°± 2.8° (P = .6678) (Table 3).
Postoperative Outcomes a
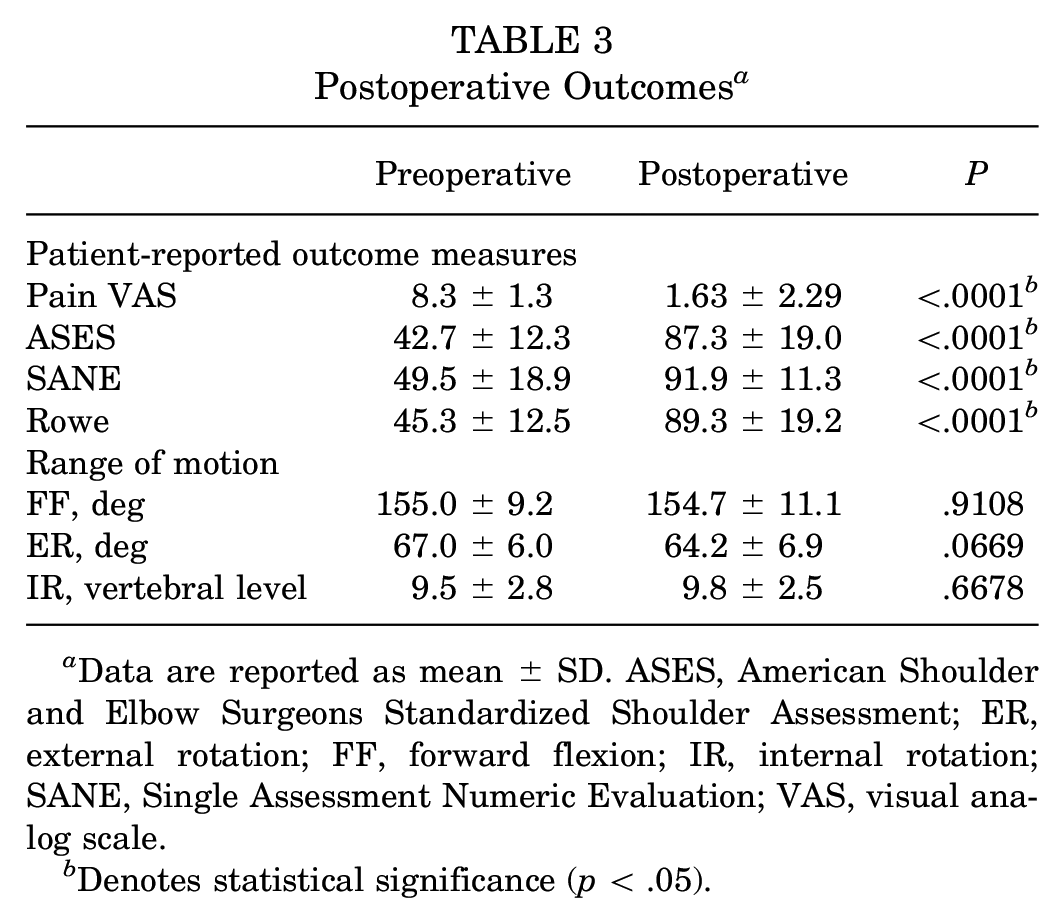
Data are reported as mean ± SD. ASES, American Shoulder and Elbow Surgeons Standardized Shoulder Assessment; ER, external rotation; FF, forward flexion; IR, internal rotation; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale.
Denotes statistical significance (p < .05).
PRO Measures
At long-term postoperative follow-up, PROMs demonstrated statistically significant improvements including a decrease in pain VAS from 8.3 ± 1.3 to 1.63 ± 2.29 postoperatively as well as an increase in ASES, SANE, and Rowe scores from 42.7 ± 12.3 to 87.3 ± 19.0 postoperatively, 49.5 ± 18.9 to 91.9 ± 11.3 postoperatively, and 45.3 ± 12.5 to 89.3 ± 19.2 postoperatively (P < .0001 for all, Table 3). Overall, 95% of patients met the threshold for MCID for VAS, 89% for ASES, 92% for SANE, and 92% for Rowe. Additionally, 58% of patients met the SCB threshold for VAS, 61% for ASES, 11% for SANE, and 74% for Rowe. Ultimately, 74% of patients achieved the PASS threshold for VAS, 76% for ASES, 76% for SANE, and 74% for Rowe. Thresholds for determining the MCID, SCB, and PASS for ASES, SANE, Rowe, and pain VAS were described by Scanaliato et al 21 and extrapolated for use in this military patient cohort (Table 4).
Patient-Reported Outcome Measure Thresholds a
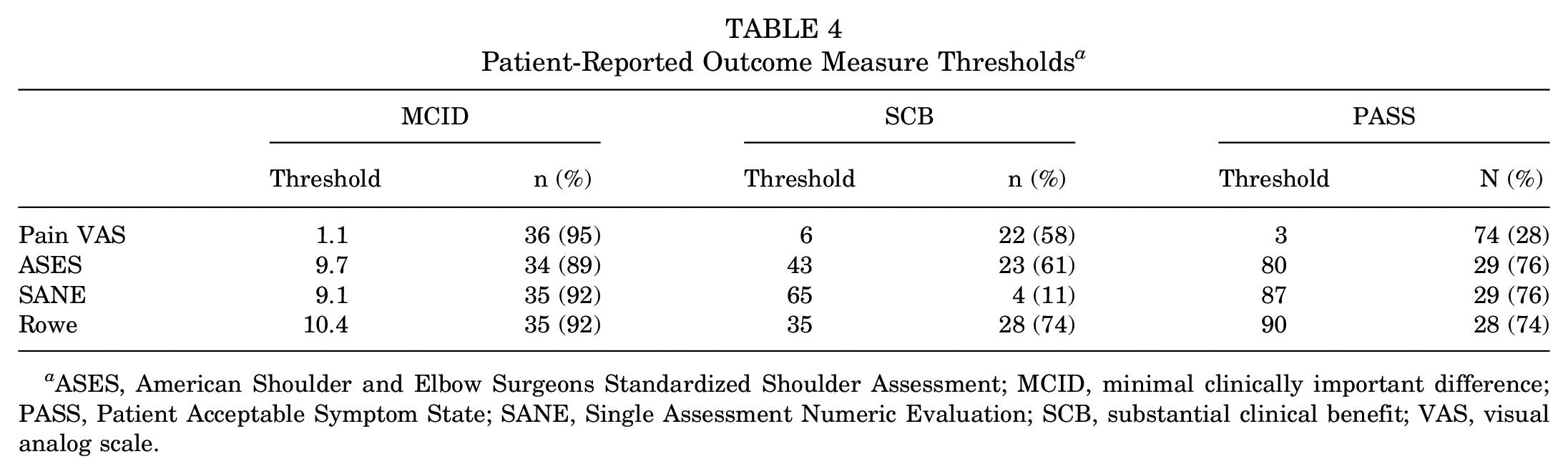
ASES, American Shoulder and Elbow Surgeons Standardized Shoulder Assessment; MCID, minimal clinically important difference; PASS, Patient Acceptable Symptom State; SANE, Single Assessment Numeric Evaluation; SCB, substantial clinical benefit; VAS, visual analog scale.
Return to Activity
At a minimum of 10 years of follow-up, 34 patients (89.5%) either retained their military duty status and returned to work or underwent discharge from the military for reasons other than continued shoulder-related disability. In total, 33 patients (86.8%) returned to participation in sports and physical training and were able to successfully complete push-ups without hindrance.
Reoperation
Two patients of the 40 that underwent isolated 270° labral repair and were not lost to follow-up (5% of 40) underwent further operative intervention after their index arthroscopic 270° labral repair: 1 required revision anterior labral repair revision and 1 required revision to a Latarjet after a traumatic dislocation of the operative shoulder. Postoperatively but before revision surgery, the patient who underwent anterior labral repair experienced a VAS change from 9 to 7, ASES from 47 to 35, SANE from 65 to 70, and Rowe from 50 to 25, while the patient who underwent Latarjet experienced a VAS change from 8 to 7, ASES from 50 to 37, SANE from 70 to 70, and Rowe from 50 to 25. Both patients retained military duty status and returned to unrestricted activity at final follow-up after revision surgery.
Discussion
The results of the present study indicate that high-demand active-duty military patients undergoing 270° labral repair can expect sustained reductions in pain, improvements in function, and return to activity. Among this patient population, 89.5% returned to full military duty or left the military for reasons unrelated to shoulder disability and 86.8% ultimately returned to sports and push-ups. In a pathology as rare and challenging to diagnose as 270° labral tears, these results are critical to counseling active-duty patients who incur higher risks of shoulder injury and greater rates of shoulder demand on postoperative expectations, both from the individual patient and from the patient’s military command.
From their development, 270° labral tears represent a challenging pathology to diagnose and manage, with many either initially missed or misclassified during preoperative clinical examination and imaging.1,14,19 In their study evaluating the variability of labral tear patterns, Alexeev et al 1 found that radiologists and surgeons reached an accurate preoperative diagnosis in 30% of cases regarding the specific type of labral tear; similarly, that 23.7% of the patients in the present study did not have MRA findings suggestive of any labral pathology. Classically, MRAs have been shown to increase diagnostic sensitivity in detecting subtle labral tears by improving contrast and visibility of intra-articular structures 22 ; however, many remained undiagnosed preoperatively in this patient cohort. Given how difficult diagnosis of this pathology is truly highlights the importance of careful intraoperative visualization and assessment of the labrum. Further complicating management is the fact that not only have ADSMs been shown to demonstrate higher rates of combined-type shoulder instability but they may also experience a greater burden secondary to this pathology due to the high-demand nature of their occupations.
In the present study, long-term outcomes among ADSMs who underwent arthroscopic 270° labral repair demonstrated statistically and clinically significant improvements with respect to PROMs—namely, pain VAS, ASES, SANE, and Rowe scores. A study by Scanaliato et al 20 reporting outcomes among the same cohort of ADSMs with ≥24 months (mean, 78 months) of follow-up offers a comparison of how these patients fared in the midterm versus the long term. At midterm follow-up, patients achieved an ASES of 89.3 ± 16.9, SANE of 93.2 ± 10.2, and Rowe of 91.34 ± 16.8, all reflecting significant increases from preoperative variables with P < .0001 that are similar to the final postoperative outcomes obtained in the present study (ASES, 87.3 ± 19.0; SANE, 91.9 ± 11.3; Rowe, 89.3 ± 19.2). Based on a comparison of these results, clinical benefits achieved secondary to 270° labral repair appear to remain sustained between midterm and long-term follow-up among the same cohort of ADSMs. While the values described by Scanaliato et al 21 for the MCID in the previously mentioned PROMs were attained from a separate cohort of military patients undergoing posterior labral repair afford a reasonable baseline to assess PROMs in those ADSMs undergoing 270° labral repair, these 2 patient populations may not be exactly the same with respect to the MCID for their PROMs.
Similarly, a study of long-term results after 270° labral repair in 21 civilian patients with ≥10 years of follow-up demonstrated similar rates of improvement, with final pain VAS noted at 0.5 ± 1.1, ASES at 91.8 ± 10.8, SANE at 91.5 ± 8.3, and Rowe at 88.7 ± 8.9. 4 Interestingly, a comparison of civilian patients’ preoperative PROM scores with the scores reported by ADSM in the present study indicated higher levels of function and lower pain among civilian patients for all measures other than SANE (VAS, 2.5 ± 2.6 vs 8.3 ± 1.3; ASES, 72.9 ± 18.4 vs 42.7 ± 12.3; SANE, 24.0 ± 15.2 vs 49.5 ± 18.9; Rowe, 53.9 ± 11.4 vs 45.3 ± 12.5 for prior civilian literature vs present ADSM data, respectively). One possible explanation for this discrepancy lies in the limited ability of ADSMs to self-regulate their physical training, occupational requirements, or deployment schedules secondary to shoulder pain and may reflect the comparatively decreased functional status they experience as a result; however, the nearly twice as high SANE score evident among ADSM may indicate that they self-judge their shoulder function as better than their civilian counterparts regardless.
Rates of return to activity were high in the present study, with 89.5% of patients returning to duty and 86.8% of patients returning to unrestricted physical training. While the return-to-duty milestone may be obfuscated by factors such as confounding career interests or variable occupational requirements, the high rate of return to duty and unrestricted physical training at >10 years of follow-up is reassuring that a patient’s ability to remain in a military career and participate in unrestricted physical training is not limited by a history of arthroscopic 270° labral repair. At ≥2 years of follow-up, Scanaliato et al 20 found that 92.3% of patients remained on active duty (although notably 1 of the 4 patients who did not return to duty left the military to pursue an alternative career, unrelated to shoulder pathology). When compared with return-to-duty rates at midterm follow-up, long-term follow-up reveals similarly high rates of retention. When compared with a civilian population of athletes, ADSMs demonstrate higher rates of return to unrestricted activity; among 25 civilian athletes, 21 of whom participated at the competitive level, Pounder et al 18 found a return-to-sport rate of 76% at a mean follow-up of 3.5 years, which remains lower than the 86.8% return to unrestricted activity observed among our cohort of ADSMs. While the physical and occupational demands of military physical training vary as compared with a competitive civilian athlete, these high rates of return to activity remain important counseling components for ADSMs before 270° labral repair.
Reoperation rates in our patient population were lower than what has previously been reported in the literature following 270° labral repair. In this cohort, 2 patients of the 40 that underwent arthroscopic 270° labral repair without major concomitant procedures and had at least 10 years of recorded follow-up (5% of 40) underwent reoperation after their index procedure, 1 for revision labral repair and 1 for a Latarjet procedure after sustaining a repeat traumatic dislocation to the operative extremity. Berthold et al 4 reported a complication rate of 14.2% in their civilian patient population cohort undergoing 270° labral repair with minimum 10-year follow-up, aside from 1 incident of transient axillary nerve palsy; specifically, they identified a single episode of repeat subluxation, 1 episode of persistent instability, and 1 traumatic dislocation. While several factors may play into the differences in reported complication rates between our military patient population cohort and the civilian patient, one plausible explanation for the differences may be the fact that ADSMs may be able to be placed on a limited duty status while they recover postoperatively, which may in turn lead to a lower complication rate when compared with civilians who may not be afforded the same recovery period. Furthermore, through the Military Health System, ADSMs are often able to more readily access high-quality postoperative physical therapy, an asset with which their civilian counterparts may not be as easily able to establish care. Additionally, a mean of 4.0 ± 0.96 suture anchors were used for labral repair in the present study which, based postoperative improvements and low rates of recurrent instability, appeared to provide appropriate stabilization to prevent recurrent instability. While some literature advocates for the use of additional anchors to enhance stability, the outcomes of the present study suggest that fewer anchors can achieve favorable long-term results.2,4,14,18
Limitations
Our study is not without limitations. First, postoperative outcomes among an ADSM population may not be readily extrapolated to a civilian population because of a number of psychosocial and environmental factors. Second, given that this study is predicated on retrospective analysis of prospectively collected data, there exists the possibility of selection bias in those patients who ultimately were included in our analysis. Third, excluding patients who experienced failure from the analysis of PROMs and presenting their PROMs separately inherently biases the results toward more favorable outcomes. Finally, while overall follow-up rates were >90% at 10 years, a total of 4 patients (9.1% of 44) were lost to follow-up.
Conclusion
Arthroscopic 270° labral repair demonstrates favorable clinical outcomes at a minimum 10-year follow-up in an active-duty military patient population, with clinically and statistically significant improvements in pain, PROMs, and an overall return-to-duty rate of 89.5%.
Footnotes
Final revision submitted January 15, 2025; accepted February 19, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.P.S. has received hospitality payments from Stryker Corp and Encore Medical. N.P. has received consulting fees from Medical Device Business Services Inc and DePuy Synthes Products and has received consulting fees from DePuy Synthes Products. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Carthage institutional review board (No. 2024-0004).