
Abstract
Background:
US military servicemembers experience higher rates of posterior and combined-type instability as compared with their nonmilitary peers.
Purpose:
(1) To determine the prevalence of glenoid bone loss (GBL) in young, active-duty military patients with combined-type shoulder instability who underwent operative shoulder stabilization; (2) to evaluate whether GBL is associated with differences in postoperative outcomes; and (3) to identify factors associated with larger defects.
Study Design:
Case series; Level of evidence, 4.
Methods:
This study included active-duty military patients who underwent primary surgical shoulder stabilization for combined anterior and posterior capsulolabral tears between January 2012 and December 2018. Preoperative magnetic resonance arthrograms were used to calculate anterior, posterior, and total GBL using the “perfect circle” technique. We recorded patient characteristics, revisions, complications, return to duty, range of motion, and scores on multiple outcome measures (visual analog scale for pain, Single Assessment Numeric Evaluation, American Shoulder and Elbow Surgeons, and Rowe). GBL prevalence was compared by time to surgery, glenoid version, history of trauma, and number of anchors used for labral repair. Outcome scores, return to active duty, and revision procedures were compared by degree of anterior or posterior GBL: <13.5% (mild) versus ≥13.5% (subcritical).
Results:
GBL was noted in 28 (77.8%) of the 36 patients. Nineteen (52.8%) patients had anterior GBL, 18 (50.0%) had posterior, and 9 (25.0%) had combined. Four (11.1%) patients had subcritical anterior or posterior GBL. Increased posterior GBL was associated with history of trauma (P = .041), time to surgery >12 months (P = .024), and glenoid retroversion ≥9° (P = .010); increased total GBL was associated with longer time to surgery (P = .023) and labral repair requiring >4 anchors (P = .012); and increased anterior GBL was associated with labral repair requiring >4 anchors (P = .011). There were statistically significant improvements on all outcome measures, with no changes in range of motion postoperatively. No significant difference on any outcome score was observed between patients with mild and subcritical GBL.
Conclusion:
In our analysis, 78% of patients had appreciable GBL, suggesting that GBL is highly prevalent in this patient population. Longer time to surgery, traumatic cause, significant glenoid retroversion, and large labral tears were identified as risk factors for increased GBL.
Members of the US military are known to experience a disproportionately high incidence of shoulder instability. 10,11,18,19,21,22,32 Previous studies have reported the rate of shoulder dislocations among military servicemembers to be 10 times higher than that observed in civilian populations. 21 Furthermore, high shoulder-demand activities such as overhead lifting and push-ups, required as part of military training, repeatedly subject the glenohumeral joint to repetitive load-bearing forces and subsequent degenerative microtrauma. 31 While anterior instability is the most common type of instability diagnosed across all demographics, multiple studies have reported higher rates of posterior and combined anterior/posterior-type instability in military cohorts when compared with nonmilitary patients. 4,22,26,32
Glenoid bone loss (GBL) in the setting of isolated anterior or posterior instability has been well described. 2,3,12,14,27,29,33 A reported 22% of patients have some degree of anterior GBL after an acute anterior instability event, and up to 86% of patients with recurrent anterior instability have appreciable GBL. 9,12 GBL is a well-known risk factor for the failure of arthroscopic shoulder stabilization procedures, 27,29,33 with bone loss >13.5% having been shown to negatively affect functional outcomes after arthroscopic stabilization for anterior instability. 27 Despite the high prevalence of GBL in patients with isolated anterior and posterior instability, as well as the increased incidence of combined instability experienced by members of the military, 4,28,32,34 there remains a paucity of data available on GBL in patients with combined instability.
The purpose of this study was to characterize GBL within a cohort of young, active-duty military patients with combined-type shoulder instability. Additionally, we sought to identify risk factors associated with increased GBL. We hypothesized that the prevalence of GBL in our cohort would be similar to that observed in patients with isolated anterior or posterior instability.
Methods
This study was a retrospective analysis of prospectively collected data of active-duty military patients who underwent primary surgical shoulder stabilization for combined-type instability between January 2012 and December 2018. Institutional review board approval was obtained for the study protocol.
The surgical database was queried for all arthroscopic shoulder instability procedures performed over a 7-year period (2012-2018). Operative reports were then reviewed to identify patients with combined anterior and posterior labral tears. All active-duty military patients from a single military base aged 18 to 40 years who underwent a primary arthroscopic surgical procedure for combined-type instability with minimum 3-year follow-up were eligible for inclusion. Final follow-up appointments for all patients were conducted in person or via telehealth on June 22, 2022. Patients with a history of shoulder surgery, full-thickness rotator cuff tears, glenoid osteochondral defects, or multidirectional instability secondary to generalized hyperlaxity (Beighton score >3) rather than discrete labral tears were excluded from the study. All patients had activity-related pain that interfered with military job requirements as well as activities of daily living. All patients had failed a trial of nonoperative management, including nonsteroidal anti-inflammatory drugs, physical therapy, limited-duty profiling, and home exercise programs for a minimum of 1 month.
Surgical Technique
All included patients underwent surgery by 1 of 2 surgeons (N.P. and R.C.T.). Surgical technique did not change markedly throughout the study period. All patients were positioned in a modified beach-chair position after administration of general anesthesia and an interscalene block. An examination was performed under anesthesia to assess range of motion and stability in the anterior and posterior directions. A Spider hydraulic arm holder (Smith & Nephew) was then utilized to stabilize the operative shoulder, and the patient was draped appropriately. Diagnostic arthroscopy of the glenohumeral joint was performed, and the capsulolabral tears were identified.
After the completion of diagnostic arthroscopy, any associated intra-articular abnormalities were documented and addressed as indicated. A transrotator cuff portal was then created medial to the rotator cuff cable (the musculotendinous junction) using a spinal needle as described by Costouros et al, 7 and the torn labrum was mobilized from the glenoid neck. A small shaver was used to create a bed of bleeding bone along the neck of the glenoid. Capsulolabral repair was performed with double-loaded Gryphon BR biocomposite suture anchors (DePuy Mitek) from January 2011 through June 2014 and with 1.9-mm double-loaded Suturefix all-suture anchors from July 2014 (Smith & Nephew). A pilot hole was drilled, and the anchor was positioned into the glenoid. A suture passer was then used to shuttle 1 of the suture limbs through the capsule and labrum. Low-profile sliding knots were tied arthroscopically, with care taken to position the knots away from the glenoid face. After completion of the procedure, adequacy of the repair site was confirmed by using a probe. Portal sites were closed with 3-0 nylon sutures, a sterile dressing was applied, and the patient’s arm was placed in a neutral rotation sling.
Postoperative Rehabilitation
Patients were discharged the same day following their procedure and were instructed to begin pendular shoulder and elbow, wrist, and finger active range of motion exercises without shoulder movement once they experienced complete resolution of their nerve block. Opioid pain medications were prescribed for up to 10 days postoperatively.
All patients attended physical therapy at the same military physical therapy group and followed the same postoperative rehabilitation protocol. Patients were immobilized for 4 weeks in a SmartSling (Ossur). At 4 weeks, immobilization was discontinued, and passive forward flexion was started. Active range of motion and progressive strengthening of the operative shoulder were started at 6 weeks postoperatively. Return to unrestricted activity was allowed at 6 months postoperatively after the patient was cleared by physical therapy.
Data Collection
Patient characteristics, duration of symptoms, preoperative chief complaint, mechanism of injury, pain scores, and outcome scores were obtained routinely during clinic visits. Traumatic cause was defined as symptom onset after a specifically recalled acute event. All patients underwent 1.5-T magnetic resonance arthrogram (MRA) as part of their preoperative evaluation. Operative reports and imaging were reviewed to determine labral tear location, the number of anchors used for repair, concomitant pathologies, and concomitant procedures performed. Medical discharge and reoperation rates were collected as part of postoperative follow-up.
GBL was determined from preoperative MRAs using an adapted method of the “perfect circle” technique 15,29 as described by Hines et al 14 (Figure 1). Data were recorded for anterior, posterior, and total GBL, as well as glenoid version. GBL was reported as a percentage of total glenoid width. All MRAs were evaluated independently by the 2 treating surgeons. For cases where there was a discrepancy between measurements, the MRA was reviewed by a third orthopaedic surgery fellow (J.P.S.).

Magnetic resonance arthrogram image of a right shoulder in a 34-year-old man demonstrating a 3.8% (1.18 mm) anterior glenoid defect and a 5.0% (1.57 mm) posterior glenoid defect measured using the “perfect circle” technique.
Patients were categorized into 2 groups based on their degree of anterior or posterior GBL. Total GBL was not used to categorize degree of bone loss. Patients with ≥13.5% anterior or posterior GBL were considered to have subcritical GBL, and those with <13.5% were placed into the minimal bone loss group. Pre- and postoperative outcomes were compared for all patients. Additionally, outcomes were compared between groups by amount of GBL.
Statistical Analysis
Statistical analyses were performed with SPSS (Version 20; IBM). Student t tests were used to compare continuous data series with a normal distribution of variance. Chi-square tests were used to compare categorical variables. The Pearson correlation coefficient (r) was used to assess the linear relationship between time to surgery and GBL. P < .05 was used to determine statistical significance for all comparisons. Interrater reliability was determined by calculating intraclass correlation coefficients based on the average of 3 measurements for each of the 2 investigators. Intrarater reliability was also determined from separate sets of measurements from each investigator performed 2 weeks apart.
Results
Between January 2012 and December 2018, 44 patients underwent arthroscopic shoulder stabilization procedures for combined-type shoulder instability. Three patients had concomitant glenoid osteochondral defects, 2 had full-thickness rotator cuff tears, and 3 were subsequently lost to follow-up, leaving 36 patients available for final analysis (Figure 2). All patients had positive examination and magnetic resonance imaging findings for a combined instability pattern, and anterior and posterior capsulolabral tears were present on diagnostic arthroscopy. All patients were active-duty military at the time of surgery. The mean age was 28.3 (range, 18-39), and 100% of patients were male. The mean follow-up was 92.03 months (43-126), and the mean time to surgery was 27.08 months (2-96) (Table 1).
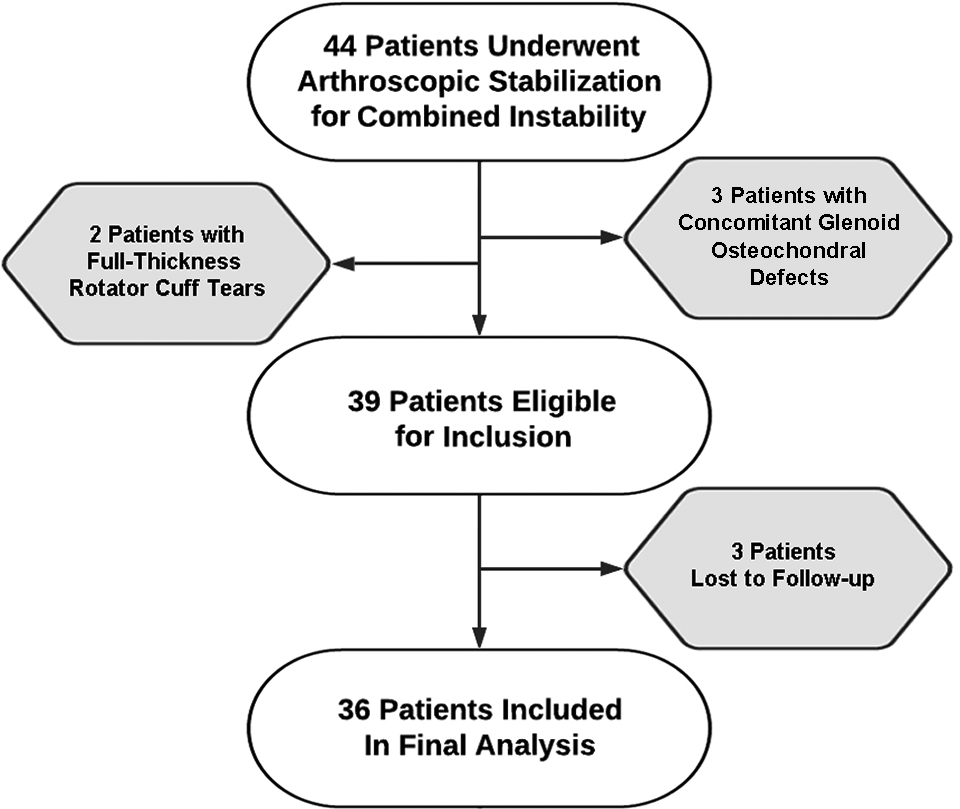
Patient selection.
Overall Patient Characteristics (N = 36)

a Data are reported as mean (range) or No. (%) of shoulders unless otherwise indicated.
b Percentage of total glenoid area.
c Negative number indicates retroversion.
GBL was noted in 28 (77.78%) patients. Nineteen (52.78%) had anterior bone loss, 18 (50%) had posterior GBL, and 9 (25%) had anterior and posterior GBL. The mean amount of anterior bone loss was 4.98% (1.52 mm), and the mean posterior bone loss was 4.86% (1.43 mm) (P = .927). Mean total bone loss was 9.84% (2.96 mm). Four (11.11%) patients had anterior or posterior bone loss ≥13.5%. Mean glenoid version ranged from –15.0° to 5.0° with a mean of –5.4° (Table 2). Intra- and interrater reliability values for GBL measurements were 0.96 and 0.89, respectively.
Patients Ranked by Percentage of Total Bone Loss

a Percentage of total glenoid area.
b Returned to active-duty military service after revision procedure.
Patients with a history of trauma had greater posterior bone loss when compared with those who did not report a traumatic cause (mean ± SD, 6.78% ± 5.42% vs 2.94% ± 5.43; P = .041). Anterior and total bone loss did not differ significantly by cause (P = .890 and P = .170) (Table 3). Posterior (2.86 ± 4.95 vs 7.09 ± 5.76; P = .024) and total bone loss (7.08 ± 7.86 vs 12.93 ± 6.70; P = .023) were significantly greater in patients with a time to surgery >1 year, and a significant correlation was observed between posterior GBL and time to surgery (r = 0.3743; P = .025) (Table 4). Patients with glenoid retroversion ≥9° had increased posterior GBL when compared with those with <9° (8.01 ± 5.74 vs 3.08 ± 4.93; P = .010). Finally, patients with labral tears requiring >4 anchors for repair (n = 18) had significantly more anterior and total bone loss than patients with smaller labral tears (P = .011 and P = .012).
Comparison of Glenoid Bone Loss by Variable a

a Data are reported as mean ± SD. Bold P values indicate statistically significant difference between groups (P < .05). Dashes indicate areas not applicable.
b Percentage of total glenoid area.
Correlation Between Time to Surgery and Glenoid Bone Loss a

a Bold P value indicates statistical significance (P < .05).
With regard to postoperative outcomes, statistically significant improvements in all outcome measures were noted. Mean visual analog scale scores for pain decreased from 7.9 ± 1.7 to 1.7 ± 2.3 (P < .0001); mean American Shoulder and Elbow Surgeons scores increased from 46.8 ± 14.6 to 87.3 ± 19.3 (P < .0001); Single Assessment Numeric Evaluation scores rose from 55.2 ± 19.3 to 92.0 ± 11.6 (P < .0001); and mean Rowe scores improved from 49.0 ± 13.3 to 89.6 ± 19.6 (P < .0001). Range of motion did not change significantly in any direction (Table 5). There were no statistically significant differences in any functional outcome scores between patients with subcritical GBL ≥13.5% (n = 4; 11%) and those with minimal bone loss. A total of 33 (91.67%) patients had returned to active-duty military service at latest follow-up; 3 patients (8.33%) were medically discharged; and 2 patients (5.56%) underwent revision Bankart and remplissage procedures and remained in the military (Table 1).
Comparison of Pre- and Postoperative Outcomes a
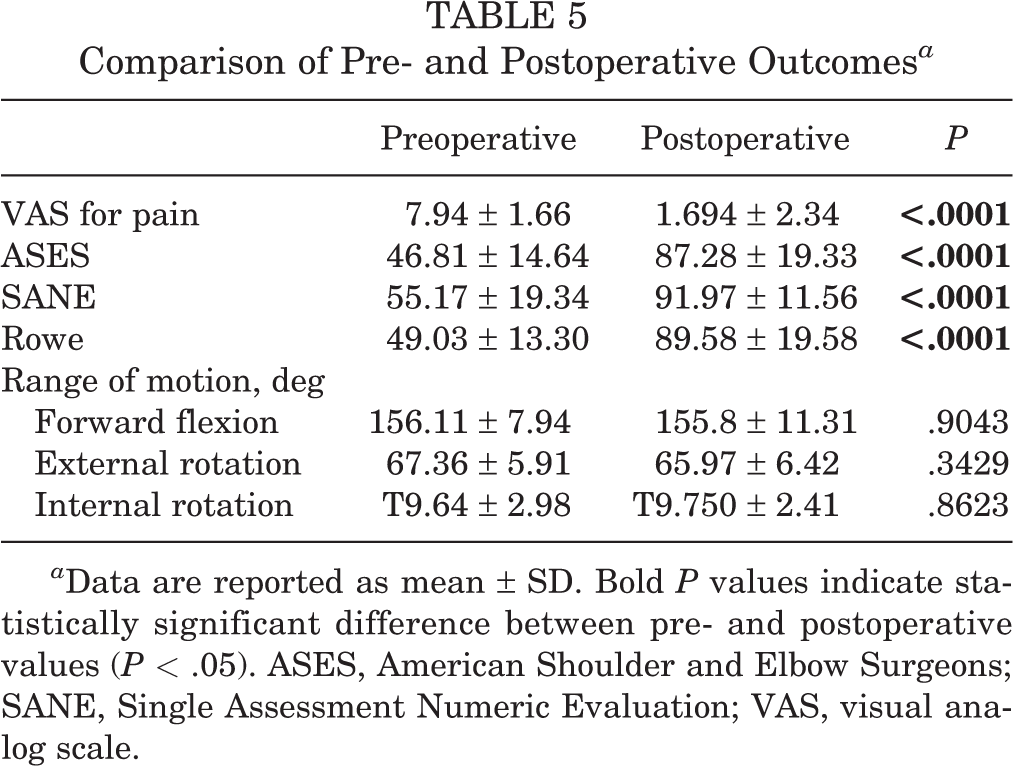
a Data are reported as mean ± SD. Bold P values indicate statistically significant difference between pre- and postoperative values (P < .05). ASES, American Shoulder and Elbow Surgeons; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale.
Discussion
The purpose of this study was to characterize GBL in a cohort of young, active-duty military patients with combined-type glenohumeral instability. Additionally, we sought to identify risk factors for greater GBL. To our knowledge, no previous studies have independently assessed GBL in a cohort of patients undergoing combined anterior and posterior labral repair. Our findings suggest that anterior and posterior GBL is highly prevalent in military patients with combined instability, with 77.78% having appreciable GBL and 11% having subcritical anterior or posterior GBL ≥13.5%. Additionally, our results suggest that time to surgery >12 months, glenoid retroversion ≥9°, and traumatic cause represent risk factors for greater GBL.
While recently published studies have found combined-type instability to account for >30% of all surgically treated cases of instability, 17,30,34 there remains a paucity of data available on GBL in patients with combined instability. With regard to anterior instability, existing literature suggests that a mean GBL of 6.8% may be seen after an acute anterior instability event and that measurable GBL may be found in up to 86% of patients with recurrent anterior instability. 8,12 Similarly, Hines et al 14 reported measurable bone loss in 69% of patients with isolated posterior instability, with >20% of patients having subcritical bone loss >13.5%. Wolfe et al 33 noted similar rates in their cohort of 66 military patients with posterior labral tears, with 86% of shoulders found to have minimal posterior GBL and 14% having subcritical GBL. These findings are in alignment with the results of our study, which suggested that >75% of patients with arthroscopically treated combined instability have appreciable GBL. Furthermore, 11% of patients had anterior or posterior bone loss ≥13.5%. Interestingly, while our sample size was limited, statistically significant improvements in all outcome scores were observed postoperatively, with no differences in functional outcomes, revisions, or return to active duty between patients with subcritical anterior or posterior GBL and those with GBL <13.5%. This contrasts with the findings of Hines et al, who observed lower rates of return to active duty among patients with subcritical posterior GBL, albeit with no appreciated differences in complication rates and number of revision procedures. However, Shaha et al 27 noted anterior GBL >13.5% to correlate with clinically significant decreases in all outcome scores after Bankart repair, even in patients who did not experience a recurrence of their instability, and Arner et al 2 reported a 10-fold higher surgical failure rate among patients with ≥11% posterior GBL. While further research is needed to fully elucidate the effect of GBL on functional outcomes in patients with combined instability, as well as to definitively establish the degree of bone loss that warrants conversion to bony reconstruction, our findings suggest that arthroscopic stabilization may represent an appropriate treatment option for patients with minimal to subcritical GBL in the setting of combined instability.
This study sought to identify independent variables associated with greater GBL. In our cohort, patients who had a time to surgery >12 months had significantly more posterior and total bone loss when compared with those who underwent operative treatment within 1 year of symptom onset. Furthermore, a significant correlation was found between posterior GBL and time to surgery. Recent evidence supports shorter time to operative stabilization in young, active patients, with timely operative intervention shown to improve functional outcomes and decrease the risk of recurrent instability. 1,2,5,6,23,25 However, military patients often face long delays from diagnosis to definitive management because of factors such as deployment and base transfers. 32 This was evident in our cohort, which had a mean time to surgery >2 years. Our findings indicate that such delays in care may place patients at risk not only for poor functional outcomes and higher rates of recurrent instability but also for greater GBL and subsequent need for open bony augmentation procedures. 1,2,12,23,27 Interestingly, we noted that patients with a traumatic mechanism of injury had significantly greater posterior GBL than patients who did not recall an acute traumatic event. This finding was unexpected as posterior labral tears are widely accepted to most often result from a “wear and tear”–type mechanism rather than discrete trauma. 24 However, these data suggest that surgeons should maintain a high level of clinical suspicion for posterior GBL when evaluating patients who present with combined instability resulting from an acute traumatic event.
With regard to glenoid version, retroversion is known to be a risk factor for the development posterior instability. 20 Owens et al 20 reported that for every degree of increased retroversion, patients had a 17% increased risk of subsequent posterior instability. However, while mild retroversion of 4° to 8° may predispose patients to instability events, our results suggest that only significant retroversion >9° correlates with increased GBL in patients with combined instability. This finding is in accordance with that of Bedrin et al, 3 who noted glenoid retroversion ≥10° to be associated with greater posterior GBL after a posterior instability event. Furthermore, Wolfe et al 33 found significantly more retroversion in patients with subcritical posterior GBL than those with GBL <13.5%, as well as higher failure rates after arthroscopic stabilization. The last variable that we observed to correlate with increasing GBL was the number of anchors utilized for labral repair, with patients who required >4 anchors having significantly more anterior and total bone loss. This finding suggests that larger labral tears are associated with greater GBL. When taken altogether, the results of this study provide a framework to help identify risk factors for increased GBL in the setting of combined instability. Recognizing and properly quantifying GBL in patients with shoulder instability is necessary to identify patients at risk for failure after arthroscopic soft tissue stabilization and therefore is imperative to selecting the most appropriate treatment option for each patient.
Limitations
This study was not without its limitations. The retrospective design of this study and its small sample size introduce inherent bias to our analysis. Our cohort was composed of entirely male, active-duty military patients, potentially limiting the generalizability of our findings to other populations. Measurements obtained from preoperative MRAs by the 2 treating surgeons were used to determine GBL and glenoid version. While some have suggested that computed tomography may be the most accurate imaging modality for assessing GBL, several studies have shown magnetic resonance imaging to be a reliable and consistent method. 13,14,16,27 With regard to the nature of our database collection, specifics regarding mechanism of injury (eg, number of instability events) and limited-duty profiling were not available for this analysis. Our cohort included only 4 patients with subcritical GBL, increasing the likelihood of a type II error in our comparison of postoperative outcomes. Last, this study was limited to patients who underwent arthroscopic stabilization procedures and therefore did not include patients with significant GBL who required open bony augmentation.
Conclusion
In our cohort of 36 military patients who underwent arthroscopic stabilization for combined-type shoulder instability, 78% had measurable GBL, suggesting that GBL is highly prevalent in this population. Furthermore, our findings suggest that time to surgery >1 year, traumatic cause, significant glenoid retroversion, and large labral tears are associated with increased GBL. Ultimately, understanding the prevalence of GBL, as well as these risk factors, may help to guide surgeons’ clinical decision-making when treating young, active patients with combined-type shoulder instability.
Footnotes
Final revision submitted February 19, 2023; accepted March 2, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.C.D. has received hospitality payments from Stryker. N.P. has received consulting fees from Mitek. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Carson-Carthage (No. 2022-04).