
Abstract
Background:
There is a lack of research specifically looking at the rates of deep vein thrombosis (DVT) and pulmonary embolism (PE) in patients undergoing meniscal repair. Many studies view arthroscopic knee surgery as a single group including meniscal debridement, meniscal repair, and chondral surgery, as well as ligament reconstruction.
Hypothesis:
Patients who underwent meniscal repair, specifically meniscus root repair, at >40 years old would have higher rates of DVT and PE than those who underwent meniscal debridement regardless of age and meniscal repair at ≤40 years old.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This study analyzed patients between the ages of 8 and 80 years who underwent arthroscopic meniscal repair versus meniscectomy at a single center. These 2 groups were then subdivided into patients who were >40 years of age and those ≤40 years of age. The 4 groups then had the rates of postoperative DVT and PE recorded and compared and the risk factors for DVT and PE analyzed.
Results:
Patients who underwent meniscal repair at >40 years of age were found to have significantly higher rates of DVT (P < .01) than those who underwent debridement regardless of age and those that underwent repair ≤40 years old (P = .02). All DVTs and PEs in the meniscal repair group >40 years old were in patients who had meniscus root repairs with a DVT incidence of 10.7% and PE incidence of 3.6%. Risk factors for the development of DVT were age as well as history of DVT.
Conclusion:
Meniscal repairs, specifically root repairs, in patients aged >40 years had high rates of DVT, which has not been documented in the literature.
Meniscal tears are one of the most common soft tissue injuries of the knee.14,18 The meniscus has many functions including force transmission across the knee joint, increasing the surface area for congruity and decreasing contact stress, as well as acting as a secondary stabilizer.2,14 An injury to the meniscus can alter the forces seen by the articular cartilage and lead to accelerated arthritic changes.2,6 Meniscal tears can be treated nonoperatively or with operative intervention including debridement and repair depending on multiple factors.14,18
Some risks of meniscal surgery, although rare, are deep vein thrombosis (DVT) and pulmonary embolism (PE).12,19 The risk of DVT and PE after meniscectomy surgery is <1%.12,19 The reporting of risk of DVT and PE after meniscal repair is limited in the literature and is commonly grouped together with ligament reconstruction and chondral surgery.3,15 Some studies have shown that age can be a risk factor for the development of DVT and PE. 22
Meniscus root tears are a specific type of meniscal tear.1,16 Many of these injuries occur with minimal to no trauma in middle-aged patients and may be a progression of a cascade of age-related changes starting with coronary ligament insufficiency and progressing to root tear.1,16 This group of root tears differs from traumatic root tears seen in younger populations. Many patients have significant pain, weightbearing limitation, and immobility from their tear that can be different from what is seen in most meniscal injury presentation.
At our institution, we noted a higher than expected trend of DVTs and PEs in these patients undergoing meniscus root repair compared with debridement. There is a gap in the literature looking specifically at the incidence of DVT and PE in meniscal repairs including meniscus root repairs. The purpose of this study was to determine if patients were at higher risk of developing DVT and PE when meniscal repair was performed when compared with debridement and if there was a particular association noted with meniscus root repairs. Secondary outcomes included determining whether age, body mass index (BMI), nicotine use, contraceptive medications, and previous DVT history were risks factors for developing DVT and PE. We hypothesized that those aged >40 years with meniscus root repair would be at a higher risk of developing PE and DVT postoperatively compared with meniscal debridement.
Methods
A retrospective chart review was undertaken for patients who underwent arthroscopic meniscal repair or debridement at a single outpatient surgical center between 2017 and 2021. Of note, the surgical center was located at >5000 feet of elevation. Patients were identified by using the Current Procedural Terminology codes for meniscal debridement (29881) or meniscal repair (29882) to search the electronic medical record. Once patients were identified, demographic data including age, sex, and BMI were recorded. Other information including surgery undertaken included repair versus debridement; type of repair; symptomatic postoperative DVT; postoperative PE; type of anticoagulation including drug, dose, and length of anticoagulation; and BMI. In addition, risk factors of DVT/PE were recorded including cancer history, nicotine use, history of DVT/PE, contraception use, or genetic clotting disorders. Tourniquet time and follow-up time were also recorded. Our institution’s postoperative DVT prophylaxis for arthroscopic meniscal surgery was aspirin (81 mg twice a day) for 2 weeks postoperatively with exceptions based on specific patient risk factors. Exceptions included patients already on anticoagulation or those with risk factors including a previous DVT or PE.
Inclusion criteria included patients between the ages of 8 and 80 years of age who underwent arthroscopic meniscal repair or debridement between 2017 and 2021. Exclusion criteria included patients who had concomitant additional surgeries that would increase operative time or change postoperative rehabilitation protocols including ligament reconstruction, osteotomy, or cartilage restoration procedures. Patients required ≥1 postoperative follow-up to be included in the study.
Patients were then divided into 2 groups, those who underwent meniscal repair (A) versus those that underwent meniscal debridement (B). These groups were then subdivided based on age of >40 years (1) versus those ≤40 years (2) (Table 1). The rates of DVT and PE 120 days postoperatively were recorded among the groups and subgroups.
Patient Groups Based on Age and Meniscal Surgery

At our institution, the postoperative weightbearing protocol for meniscectomy was weightbearing as tolerated without a brace. The postoperative weightbearing protocol for meniscal repairs varied from weightbearing as tolerated to partial weightbearing for 6 weeks with a Bledsoe brace unlocked 0° to 90°. Meniscus root repair weightbearing protocol was touchdown weightbearing for 6 weeks in a brace unlocked 0° to 90°.
All data analysis was performed using SPSS Statistics Version 24 (IBM Corp) software. Alpha was set at .05 with a P < .05 considered statistically significant. Student t test and logistic regression were used to analyze continuous parametric samples, while the Fisher exact test was used for categorical data.
Results
A total of 595 patients and 623 surgeries were included in the study, after 56 patients were excluded based on exclusion criteria. By group, 62 surgeries were included in group A1, 54 were included in A2, 280 were included in B1, and 227 were included in B2. There were 19 male and 43 female patients in group A1, 28 male and 26 female patients in group A2, 157 male and 123 female patients in group B1, and 149 male and 78 female patients in group B2. There was a significant difference for sex between repair and debridement, with more female patients undergoing repair and more male patients undergoing debridement (P < .01). There was a longer tourniquet time in the repair versus debridement group (61 vs 28 minutes; P < .01). There was no difference between BMI and age between repair and debridement groups. The incidence of DVT in the meniscal repair group was 6 (5.17%). All the DVTs in the repair group were seen in patients undergoing root repairs over the age of 40 years with an incidence of 10.7%. The incidence of DVTs in the meniscal debridement group was 4 (0.79%). The incidence of PEs in meniscal repair group was 2 (1.72%). Both PEs seen in the meniscal repair group were root repairs in patients >40 years of age with an incidence of 3.6%. There were 3 PEs in the meniscal debridement group, 0.59% (Tables 2 and 3).
Number of Surgeries and Percentage of DVT/PE Within Each Group a

Bold indicates statistical significance. DVT, deep vein thrombosis; PE, pulmonary embolism.
Root vs Nonroot Repair in Relation to Age With Number of Patients and Percentage of DVT/PE Within Each Group a

DVT, deep vein thrombosis; PE, pulmonary embolism.
The mean time from surgery to DVT diagnosis was 40.2 days for the debridement group and 43.3 days for the repair group. The mean time from surgery to PE diagnosis was 19 days for the debridement group and 27.5 days for the repair group. The anticoagulation for patients with DVTs in the debridement group included 2 patients with aspirin (acetylsalicylic acid [ASA]) for either 2 weeks or 45 days, one with enoxaparin (Lovenox) for 2 weeks, and one with no documented DVT prophylaxis. One of these patients had a history of a DVT. For those with PEs in the debridement group, 2 patients were on Lovenox for 2 weeks while the other patient was not on documented DVT prophylaxis. Two of these patients had a history of DVTs. For those with DVTs in the repair group, 4 patients were on ASA for 2 weeks, 2 patients were on apixaban for 2 weeks then transitioned to ASA for 2 weeks. Two of these patients had a history of breast cancer on estrogen modulators, 2 were on oral contraceptive pills, and the other 2 did not have risk factors other than lower extremity surgery (Tables 4 and 5). For those with PEs in the repair group, one patient was on apixaban for 2 weeks then transitioned to ASA for 2 weeks while the other patient was on ASA for 2 weeks. One of these patients was on a breast cancer estrogen modulator while the other had no risk factors.
Types of Prophylaxis Between Surgical Groups a
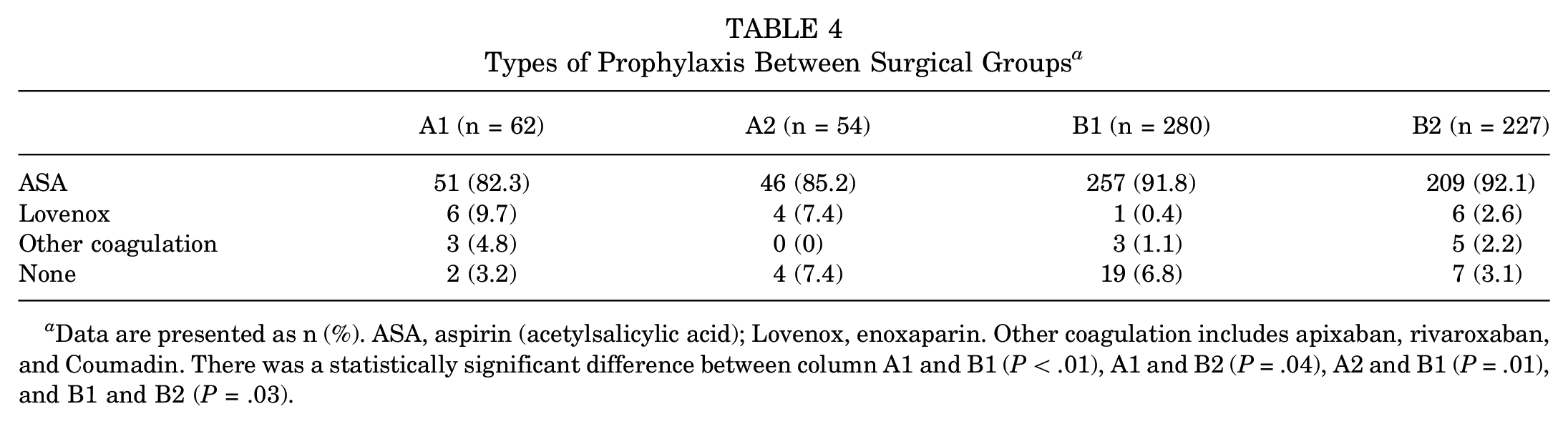
Data are presented as n (%). ASA, aspirin (acetylsalicylic acid); Lovenox, enoxaparin. Other coagulation includes apixaban, rivaroxaban, and Coumadin. There was a statistically significant difference between column A1 and B1 (P < .01), A1 and B2 (P = .04), A2 and B1 (P = .01), and B1 and B2 (P = .03).
Patients Who Developed DVT Postoperatively Including Surgery, DVT Prophylaxis, Risk Factors, and Days Postsurgery When DVT Was Found a

ASA, aspirin (acetylsalicylic acid); BID, twice a day medication frequency; DVT, deep vein thrombosis; Lovenox, enoxaparin; OCP, oral contraceptive pill; PE, pulmonary embolism.
Patients who underwent meniscal repair were more likely to develop a DVT compared with the debridement group (P < .01). There was no difference between patients ≤40 years of age when comparing debridement with repair for the development of DVT (P ≥ .99). Patients >40 years of age had a higher incidence of DVT when undergoing repair compared with debridement (P < .01). Patients who were >40 years of age had a higher incidence of DVT compared with those ≤40 years of age when undergoing repair (P = .02). There was no difference in DVT incidence between those >40 years old compared with younger when undergoing debridement (P = .60). Logistic regression found that age was a significant factor in developing a DVT while undergoing arthroscopic meniscal surgery, although this may be skewed by a significant difference found in the repair group (P = .02). Our study was underpowered to compare rates of PEs across groups, although we found no difference across groups.
Nicotine use was not associated with the development of DVT in the debridement or repair groups (all P ≥ .99). BMI was not associated with the development of DVT in the debridement or the repair group (P = .59; P = .66; P = .10; P = .40). Sex and use of oral contraceptive or birth control implants (P = .30; P ≥ .99) were not associated with the development of DVTs. History of a DVT was associated with the development of DVT when repair and debridement data were combined (P = .03), but not when repair and debridement groups were analyzed individually.
Discussion
Our study found that meniscal repair, specifically meniscus root repairs, in patients >40 years of age are associated with a higher incidence of DVT compared with meniscal debridement, but no difference in PEs. This is the first study that we are aware of that has looked specifically at the risk of DVT and PE in meniscal repairs compared with meniscal debridement. The incidence of DVT in the meniscus root repair group >40 years of age was 10.7% while the incidence of PEs was 3.6%. Our study was underpowered to make conclusions regarding PE rates across groups and would require a larger sample size for meaningful analysis. These rates of DVT and PE are high compared with what is typically assumed with meniscal surgery in general.12,19 When compared with the orthopaedic trauma literature for pelvic and acetabular fractures, one study noted a DVT rate of 4% and of PE, 2.8%. 10 Our study had similar PE rates, but the DVT rate was over twice as high. Our rate of DVT and PE for the debridement group is on par with what is stated in the literature.3,12 There are a variety of factors that could have contributed to the high rates of DVT and PE including tourniquet times, postoperative weightbearing, the high altitude of our institution’s location, and age.
The tourniquet time for the repair group was twice as long as the debridement group, which was expected. However, studies have shown that tourniquet times >60 minutes increase the risk of venous thromboembolism (VTE).8,21,23 There is prolonged stasis with higher tourniquet times, and the avascularity may promote inflammation, which may increase the risk of blood clot formation.22,23 In addition, patients with meniscus root repairs often present preoperatively with injury-related activity modification and limited weightbearing and are touchdown weightbearing postoperatively for 6 weeks, which may also contribute to increased risk. One study showed that patients after anterior cruciate ligament reconstruction were at higher risk of DVT when made nonweightbearing postoperatively. 13
Our institution is also at >5000 feet of elevation with some patients living at altitudes >7000 feet. One study found that an altitude of >4000 feet of elevation significantly increased the risk of DVT development after knee arthroscopy compared with patients at ≤100 feet of elevation. 5 In addition, age has been shown to be a risk factor for VTE development and this was also shown in our study. One study found that patients aged >40 years had a higher risk of developing DVTs in elective arthroscopic knee surgery. 22
The mean time to DVT diagnosis was 43 days for the repair group. Typical follow-up times were 2 weeks, 6 weeks, 3 months, 6 months, and 1 year. Of the 6 patients with DVTs in the repair group, 4 patients were on ASA for 2 weeks postoperatively while the other 2 patients were on apixaban for 2 weeks then ASA for 2 weeks. There may be some validity to prolonging the course of DVT prophylaxis until patients are fully weightbearing, which would be at the 6-week mark. However, there is controversy with DVT prophylaxis for knee arthroscopy surgery as to whether treatment is needed and for how long, as well as what type of medication is appropriate.9,15 One review notes patient-specific factors including BMI, age, and history of DVT, as well as other factors that should be taken into account as to whether a patient should be placed on DVT prophylaxis after knee arthroscopy; the study, however, does not specify on weightbearing status, type of surgery, or length of prophylaxis. 9 Some studies have shown that low-dose heparin lowers the risk of DVT development after knee arthroscopy.4,25 Another study found that ASA is a cost-effective treatment for preventing VTE in knee arthroscopy. 20 There was a difference in our study between the type of DVT prophylaxis used between some of the groups. This difference can be largely attributed to the fact that those >40 years of age typically have more comorbidities compared with those <40 years old, leading to more alternative anticoagulation outside of ASA. In addition, there is a set protocol for anticoagulation after meniscal surgery, but surgeons deviate from this more commonly after meniscectomy, with more patients given no DVT prophylaxis after surgery. The type of anticoagulation after meniscal surgery is controversial and no standard has been set in the literature.
There is a gap in the literature when looking at VTE incidence in meniscal surgery. Many studies look at knee arthroscopy as a whole, which leads to a heterogeneous group that potentially includes patients at varying risk and of varying numbers.3,11,15,17,19,24 Anterior cruciate ligament reconstruction, meniscal debridement, and meniscal repairs are all different surgeries with different postoperative physical therapy protocols as well as length of surgery. Our study is the only study that compares debridement with repair for meniscal surgery.
Other risk factors for DVT development in patients undergoing knee arthroscopy include an elevated BMI, sex, nicotine use, contraceptive medications, and history of VTE.3,7,11,19 All these factors were found to not be associated with an increased incidence of VTE except for a personal history of DVT. Two of the 6 patients in the repair group had a history of DVT. Despite anticoagulation, these patients developed a VTE, although their prophylaxis was for 4 weeks.
Limitations
Limitations of this study include a small sample size in the meniscal repair group, which could introduce statistical fragility into the findings. This is a retrospective study that relies on documentation in the chart for analysis. We do not know if all patients completed their DVT prophylaxis. In addition, some patients could have been seen outside of our hospital system for their diagnosis and treatment of DVTs and PEs, which would not have been captured in our data.
Conclusion
Our study serves as a good pilot study for a large database retrospective or prospective study. We found a high incidence of DVT and PE in patients >40 years of age who underwent meniscus root repair. Factors that may have contributed to this high rate of VTEs include longer tourniquet times, living at altitude, weightbearing status before and after surgery, length of DVT prophylaxis, and type of DVT prophylaxis. These factors may explain a 10.7% incidence of DVT, but this high rate warrants further investigation. In addition, further studies are needed to determine proper treatment including medications and duration, as meniscus root repair patients >40 years of age are at a high risk of VTE.
Footnotes
Acknowledgements
Dr. Laurie Wells was the statistician on this study and completed all of the data analysis.
Final revision submitted December 7, 2024; accepted February 11, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.K. has received education payments from Arthrex/Gemini Mountain Medical. C.S. has received hospitality payments from Stryker and Arthrex/Gemini Mountain Medical, education payments from Smith & Nephew and Southtech Orthopedics, and a grant from Arthrex. G.T. receives educational support from Arthrex and has received hospitality payments from Arthrex/Gemini Mountain Medical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto
Ethical approval for this study was obtained from the University of New Mexico (No. 22-023).