
Abstract
Background
Venous thromboembolic events (VTEs) are common after total knee arthroplasty (TKA). The rate of VTEs has improved with early mobilization, mechanical prophylaxis, and appropriate chemoprophylaxis. The aim of this study was to analyze the contribution of medical comorbidities to the risk of VTE after TKA
Method
Medicare claims from 2005 to 2014 were queried. International Classification of Diseases, Ninth revision (ICD-9), and Current Procedural Terminology codes were used to identify the diagnoses, procedures, and complications. 157,200 primary TKAs were age, sex, and Elixhauser Comorbidity Index (ECI) matched with 157,200 osteoarthritis controls. First instances of deep venous thrombosis (DVT) and pulmonary embolism were tracked at 90 days and 2 years. Odds ratios (ORs), confidence intervals, and P-values (p) were calculated and used to investigate the contribution of comorbidities.
Results
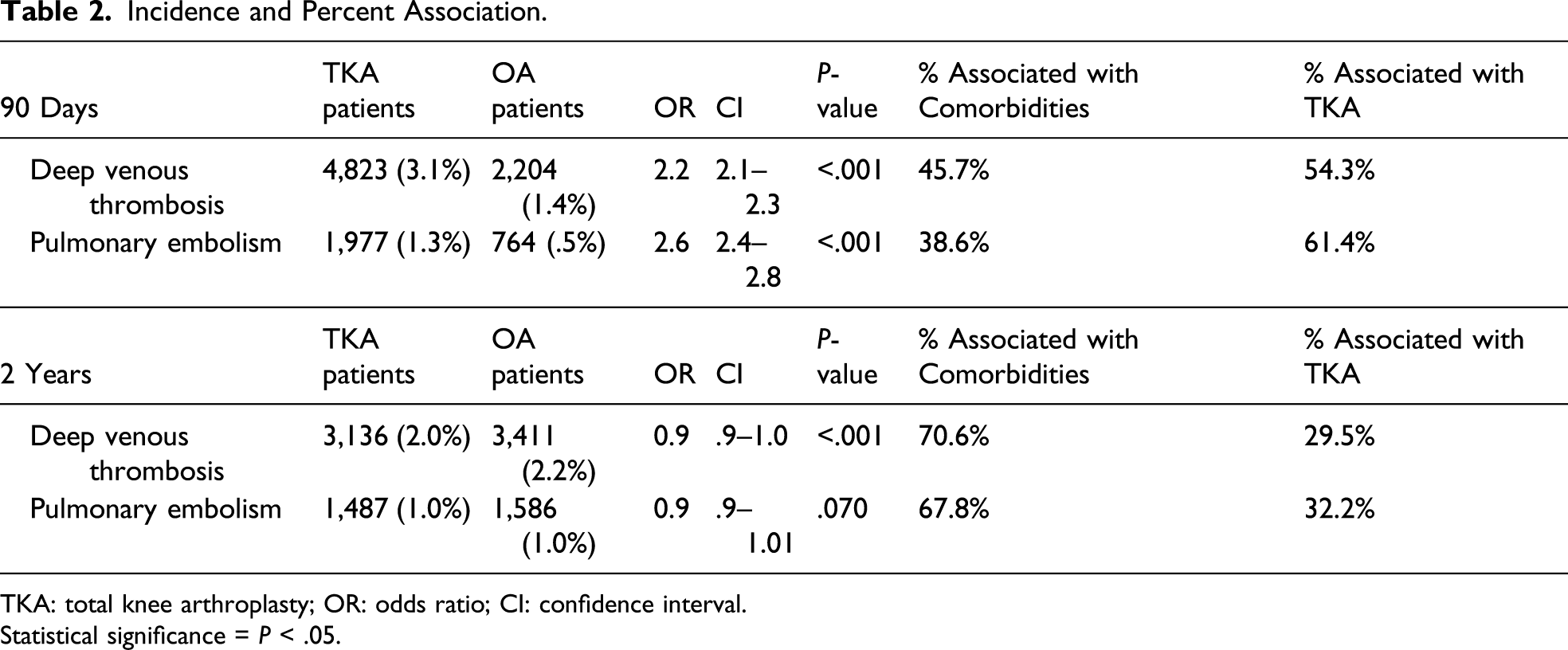
90 days after TKA or OA diagnosis, comorbidities were associated with 45% of the DVT risk, 38% of the PE risk. 1 in 92 patients would be expected to be diagnosed with VTE after TKA and 1 in 136 patients after only the diagnosis of osteoarthritis. After 90 days, medical comorbidities were associated with 70% of the DVT risk, 68% of the PE risk.
Conclusion
Nearly 50% of DVTs and 40% of PEs within 90 days of TKA may be related to the baseline health of OA patients. Venous thromboembolic events after TKA are a “never” event according to Center of Medicare and services that appropriate VTE prophylaxis likely cannot be neutralized.
Introduction
Deep vein thrombosis (DVT) and pulmonary embolism (PE), together referred to as Venous thromboembolic events (VTEs), remain common complications after major orthopedic surgery. Venous thromboembolic events are associated with significant morbidity and mortality after total knee arthroplasty (TKA).1,2 The incidence of fatal PE after a TKA has been reported to be 0.15%. 3 Given the seriousness of this potentially preventable complication, venous thromboembolism has been considered a “never” event by the Center of Medicare and services (CMS) who began financially penalizing institutions in 2009.4–6 The baseline prevalence of a VTE remains controversial, but overall has declined in association with implementation of early mobilization mechanical prophylaxis, and routine chemoprophylaxis.7–13
Although major surgery is an independent risk factor for VTE, we must also consider the other characteristics that independently contribute (e.g., body mass index, hospitalization, trauma/fracture, active cancer, transvenous pacemaker, varicose veins, urinary tract infection, neurologic disease with leg paresis). 14 Patients diagnosed with osteoarthritis tend to have more comorbid medical conditions than those without osteoarthritis. 15 In end-stage osteoarthritis patients, advanced age as well as pain is associated with an increased risk of a VTE.16,17 Asymptomatic pre-operative DVTs may even be present in 8–17% of patients prior to TKA.8,9 Little is known about the baseline contribution of a patient’s health to the risk of a VTE after a TKA. We hypothesize that medical comorbidities are a potential factor in 50% or more of the VTEs that occur postoperatively in patients diagnosed with osteoarthritis (OA) that undergo TKA.
The purpose of this study was to quantify the effect of patient comorbidities on the incidence of DVT and PE after TKA by comparing the VTE rate after TKA to a matched cohort of patients newly diagnosed with knee osteoarthritis that have not undergone arthroplasty.
Methods
Elixhauser Comorbidities for Total Knee Arthroplasty and Osteoarthritis Patients.

TKA: Total Knee Arthroplasty; OR; Odds Ratio; CI: 95% Confidence Interval; Significance: p < 0.05
Demographic Characteristics.
TKA: Total Knee Arthroplasty; OR; Odds Ratio; CI: 95% Confidence Interval; Significance: p < 0.05
We identified patients diagnosed with a DVT or PE using their corresponding International Classification of Diseases, Ninth Revision (ICD-9) diagnosis codes (i.e., 453.40 and 415.1). Using this method, the diagnostic labs and tests used to diagnose VTE were not able to be analyzed. Also, postoperative strategies regarding the type, timing, and duration of a VTE prophylaxis used were not reported or analyzed. Only the first instance of DVT or PE were tracked at 90 days and 2 years from the date of TKA or the first-time diagnosis of OA, to prevent any preexisting diagnoses of VTE on the patient’s record from confounding the results.
We used the difference in VTE incidence between the 2 cohorts divided by the VTE incidence in the TKA cohort to assign the percent of VTE incidence associated to TKA alone. The remaining value was assumed to be related to patient comorbidities (Figure 1). Outcomes are presented as proportions with a chi-square test used for comparison. We calculated odds ratios (OR), 95% confidence intervals (CI), and P-values (p) for each DVT and PE complication with statistical significance was set to an alpha error of 3% after a Bonferroni correction for 2 primary outcomes—DVT and PE—that define VTE.
20
Equation used to assign percent incidence of venous thromboembolic events (VTE) associated with total knee arthroplasty (TKA) and patient comorbidities.
Results
Within 90 days
54% of the DVT rate was associated with the TKA and 46% with baseline medical comorbidities (Figure 2). There was a doubling of the odds of a DVT (OR 2.2, CI 2.1-2.3, P < 0.001) associated with a TKA. The elevation in absolute risk of a DVT associated with a TKA was 1.7%. Therefore, 1 in 59 patients would be expected to be diagnosed a DVT related to their TKA alone and 1 in 71 related to their medical comorbidities (Table 3). 61% of the PE rate was associated with the TKA and 39% with baseline medical comorbidities (Figure 2). There was a doubling of the odds of a PE (OR 2.6, CI 2.4-2.8, P < 0.001) associated with a TKA. The elevation in absolute risk of a PE associated with a TKA was 0.8%; therefore, 1 in 125 patients would be expected to be diagnosed with PE related to their TKA alone and 1 in 200 related to their medical comorbidities (Table 3). For VTE (DVT and PE), 1 in 92 patients would be expected to be diagnosed with VTE after TKA and 1 in 136 patients after only the diagnosis of osteoarthritis. The percentage of venous thromboembolic events (VTE, * = deep vein thrombosis or pulmonary embolism) associated with patient comorbidities (orange) of total knee arthroplasty (TKA, blue) at 90 days. Rates were calculated by dividing incidence of VTE in osteoarthritis group (OA, No TKA) by rate in TKA group, then subtracting from 100. Incidence of Deep Venous Thrombosis and Pulmonary Embolism as well as the Percent Association with TKA or Baseline Medical Comorbidities. TKA: Total Knee Arthroplasty; OR; Odds Ratio; CI: 95% Confidence Interval; Significance: p < 0.03

After 90-days
30% of the DVT rate was associated with the TKA and 70% to the patients’ baseline medical comorbidities (Figure 3). There was a slight decrease of the odds of a DVT (OR 0.9, CI 0.9–1.0, P < 0.001) associated with a TKA (Table 3). 32% of the PE rate was associated with the TKA and 68% to the patients’ baseline medical comorbidities (Figure 3). There was no statistically significant difference in the odds of a PE (OR 0.9, CI 0.9–1.0, P = 0.070) associated with a TKA (Table 3). The percentage of venous thromboembolic events (VTE: * = deep vein thrombosis or pulmonary embolism) associated with patient comorbidities (orange) of total knee arthroplasty (TKA, blue) at 2 years. Rates were calculated by dividing incidence of VTE in osteoarthritis group (OA, No TKA) by rate in TKA group, then subtracting from 100.
Discussion
To our knowledge, this represents the largest database study on the contribution of baseline health status to the risk of VTE after TKA on standard chemoprophylaxis. A total number of 157,200 patients who underwent TKA were compared to a matched cohort of 157,200 who received the diagnosis of OA. Within 90 days of a TKA, almost half of the VTE rate appear to be related to the patients baseline medical comorbidities. However, 90 days after a TKA, the likelihood of a VTE returns to the baseline established by comorbid medical conditions.
It is well established that patients with more comorbid conditions are at higher risk of VTE. In an extensive review of the literature, Goldhaber et al. concluded that hospitalized patients with a history of major surgery, cancer, congestive heart failure, chronic obstructive pulmonary disease, and chronic kidney disease were especially susceptible to VTE. In the community, incidence of VTE increased significantly with age, venous insufficiency, pregnancy, trauma, frailty, and immobility. 21 Specifically looking at knee OA patients in a retrospective single-center study, Jiang et al. reported that pre-operative d-dimer >0.5 mg/mL and age >75 were independent risk factors for pre-operative DVT. They also cited literature reporting significantly higher risk of a VTE in women undergoing TKA. Their study confirms this our findings. 7
Patients with a diagnosis of OA also tend to have more comorbid medical conditions. In a meta-analysis of 42 observational studies from 16 countries by Swain et al., they found that 67% of individuals with osteoarthritis had at least 1 other chronic condition, 20% higher than those without OA. The body systems most likely to be affected by comorbidities in individuals with OA were upper gastrointestinal, psychological, cardiovascular, and endocrine. Stroke, peptic ulcer, and metabolic syndrome were the most common comorbidities in osteoarthritis. 15 These comorbid conditions likely drive an increased baseline VTE risk that cannot be neutralized with standard VTE prophylaxis used in the TKA peri-operative period.
We found the rate of VTE after TKA in our population to be around 4% at 90 days; this aligns with those previously cited in the literature;10,22,23 however, in patients with only the diagnosis of OA, our population demonstrated a lower VTE rate of 2% at 90 days. In a retrospective study spanning 10 years with over 9,000 patients undergoing primary TKA who received either low (81 mg twice daily) or high (325 mg twice daily) dose aspirin for VTE prophylaxis, the median time to VTE was 8 days (interquartile range [IQR] 2-15.5). 24 Given that our study examined TKA patients at 90 days, it is reasonable that this may be an overestimate of VTE incidence in this group that is required/tolerated because of bundled payment models.
Jiang et al. examined 521 patients with knee degenerative OA scheduled to undergo TKA with ultrasonography and found an incidence of pre-operative DVT just under 7%. 7 Wakabayashi et al. performed a retrospective single center study in which 17% of 322 TKAs had a DVT prior to surgery. 8 Of note, over one-third of revision TKAs as well as patients with comorbid rheumatoid arthritis had a pre-operative DVT. 8 In a pro-spective study, Watanabe et al. examined 71 TKAs with 16 row multidetector computed tomography for asymptomatic pre-operative VTE and found 8% of the patients had a DVT with no history of a disease known to cause thrombosis. 9 We believe the variability in sample sizes, and method of VTE diagnoses, as well as different levels of evidence account for the discrepancy in detectable VTE rates when compared to our rate. The median time to VTE after diagnosis of OA is not clearly defined in the literature; therefore, evaluating this group at 90 days may also be an overestimation. In our study, uniform methodology and matching of both groups help to negate the potential overestimation in the absolute value of the VTE incidence and substantiate the overall result that almost 50% of the VTE rate may be related to medical comorbidities alone.
Limitations
This is a retrospective database study that has limitations when compared to retrospective and prospective chart review in that it relies on the accuracy, precision, and inclusiveness of coding. Full patient histories and physical exams cannot be collected; therefore, it is unclear if the VTEs were symptomatic. Peri-operative data such as the type of anesthesia, duration of surgery, tourniquet use, pain control, and speed of mobilization were not reported or analyzed. Diagnostic labs and tests to detect/diagnose VTE such as ultrasound, computed tomography, and d-dimer were not reported or analyzed. The type, timing, and duration of VTE prophylaxis used were not reported or analyzed. Taken together, these findings can only highlight possible associations and cannot establish causation between TKA, OA, or medical comorbidities and the diagnosis of VTE. We analyzed patients from 2005–2014; any advancements related to VTE prevention and management since this time were not captured in this study. All of the matched comorbidities in the ECI are not necessarily independent risk factors for VTE events. Even with the ECI and demographic data matched for the cohorts, a multivariate analysis would be difficult to perform as no individualized data is available to allow further stratification to determine the specific impact of TKA. This type of study, nevertheless, has been shown to be useful in the TKA literature: even though the data may be incomplete, it has been reported to be accurate. 25 There continues to be a growing use of large databases to answer clinical questions and trends related to TKA that would have otherwise been very difficult to answer without large numbers. The study does not take account of potential ascertainment bias. After surgery, physicians actively look for VTE as a known complication of TKA, whereas after a diagnosis of OA the diagnosis of a VTE is only likely to be made if the patient presents with active symptoms.
Conclusion
While VTEs are considered a “never” event according to CMS, this study suggests that not all VTEs in the postoperative period are the result of TKA alone as it demonstrates that nearly 50% of DVTs and 40% of PEs within 90 days of TKA may be related to the baseline health of OA patients. Appropriate VTE prophylaxis likely does not neutralize all baseline medical risk of a VTE, and a significant number of patients may have had a VTE event regardless of their TKA. Given the limitations of this type of study, we can only highlight possible associations and cannot establish causation. Therefore, future studies via retrospective, randomized, or observational scrutiny should explore the details surrounding the VTE events in both cohorts and how modern anticoagulation protocols impact the baseline VTE risk.
Footnotes
Author’s Note
Investigation performed at Stanford Health Care, Palo Alto, California, USA.
Authors Contributions
K.O., A.B., and D.F.A. contributed to the design and implementation of the research, analysis of the results and writing of the manuscript. All authors read and approved the final manuscript.
Declaration of Competing Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Dr. Amanatullah is supported by the NIH-NCATS KL2 Award (KL2TR003143).
Ethical Approval
This study involves the analysis of public use data sets; therefore, it is exempt from review by our institutional review board.
Informed Consent
All Authors read and approved the final article.