
Abstract
Background:
Patellofemoral osteoarthritis is a recognized complication after anterior cruciate ligament (ACL) reconstruction (ACLR). Nevertheless, previous studies have not adequately addressed the connection between pain severity and the presence of early patellofemoral osteoarthritis during initial rehabilitation exercises after ACLR.
Purpose:
To explore the correlation between knee pain severity during early flexion exercises and chondral changes of the patellofemoral joint.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We included 121 patients who underwent ACLR. Patients were categorized into 3 groups based on their Numeric Rating Scale pain scores during rehabilitation exercises. Group A consisted of pain levels <3 points, group B had scores 4 to 6 points, and group C had scores ranging from 7 to 10 points. Magnetic resonance imaging (MRI) assessments were conducted preoperatively and 3 months postoperatively, utilizing T2-mapping MRI sequences to evaluate the composition of patellofemoral articular cartilage. We also performed subjective assessments using International Knee Documentation Committee (IKDC), Knee injury and Osteoarthritis Outcome Score (KOOS), Lysholm, and Kujala scoring systems preoperatively and postoperatively.
Results:
The T2 values demonstrated statistically significant differences between groups A and C in the trochlear lateral condyle (31.5 ± 3.3 vs 34.8 ± 3.0; P < .01), trochlear groove (32.8 ± 3.4 vs 36.1 ± 4.0; P < .01), lateral surface of the patella (32.9 ± 3.2 vs 35.9 ± 3.7; P < .01), and ridge of the patella (32.6 ± 3.3 vs 36.0 ± 3.9; P < .01) at 3 months postoperatively. Significant differences were also noted between groups A and B in the trochlear lateral condyle (31.5 ± 3.3 vs 32.9 ± 3.0; P < .05), trochlear groove (32.8 ± 3.4 vs 34.7 ± 3.9; P < .05), and ridge of the patella (32.6 ± 3.3 vs 34.2 ± 4.0; P < .05). Comparisons between groups B and C further illustrated differences in the trochlear lateral condyle (P < .01) and ridge of the patella (P < .05). Subjective evaluations revealed significant differences between group A and group C in IKDC, KOOS, Lysholm, and Kujala scores 3 months after surgery.
Conclusion:
This study indicates that knee pain during early rehabilitation exercises after ACL reconstruction is associated with MRI changes in the patellofemoral joint and that more intense pain perception during early rehabilitation exercises is associated with more severe changes.
Keywords
Anterior cruciate ligament (ACL) injury is one of the most prevalent sports injuries, frequently necessitating surgical reconstruction.13,20,22,26 ACL reconstruction (ACLR) proves to be an effective intervention, enhancing quality of life, functional capability, and symptom management compared with nonoperative treatments. 2 Research indicates that the success rates for ACLR are >90%, falling into the good to excellent range for most patients. 6 However, despite these strong outcomes, ACLR is not free from complications. Patellofemoral joint (PFJ) complications, such as patellofemoral pain (PFP) and patellofemoral osteoarthritis (PFOA), are recognized sequelae after ACLR and may emerge shortly after the procedure.9,41
Studies indicate that approximately 6% to 26% of patients who have undergone ACLR have either PFP or PFOA within the first 2 years after surgery.7,19,29,32,41 Further studies have shown a median prevalence of around 50% at 10 to 15 years after ACLR.9,27 Despite the significant occurrence of PFJ complications after ACLR, the primary mechanisms behind these issues remain inadequately explored.
Various factors, such as concomitant damage to articular cartilage, quadriceps muscle weakness, meniscal resection, follow-up duration, sex, age, body mass index, and limitation of knee range of motion (ROM), have been reported as contributors to PFOA development after ACLR.1,8,10 It has also been reported that changes in the PFJ load after ACLR contribute to PFOA, with patients showing altered loading patterns at the knee joint, including increased or decreased stress between the patella and the femoral trochlear groove.11,12,16,31,36 Additionally, a study revealed that individuals with PFOA experience greater sagittal plane patellofemoral stress during the latter half of the stance phase compared with those without PFOA. 35 This finding implies that sagittal plane joint moments may play a significant role in the development of PFOA.
Wright et al 43 reported that the joint-loading patterns of the PFJ after ACLR seem to be established during the initial rehabilitation stages and remain consistent over time. They found that patients who underwent ACLR typically started increasing their exercise levels around 12 weeks postoperatively, engaging in more functional activities such as jogging and single-leg exercises, which led to enhanced loading on the PFJ.33,43 However, in our clinical practice, we have noted that some patients experience degeneration of the PFJ approximately 3 months, or even earlier, after ACLR. By reviewing the rehabilitation journey of these individuals, we have found that some patients have more PFJ pain during rehabilitation and hypothesize that this may be due to early degeneration of the PFJ.
Therefore, the primary purpose of this study was to see if there was a correlation between the severity of pain during early knee flexion exercise and PFJ chondral changes. We hypothesized that knee pain during early rehabilitation exercise after ACLR may be associated with early chondral change of the PFJ and that more intense pain perception during early rehabilitation exercise is associated with more severity of magnetic resonance imaging (MRI) chondral changes of the PFJ.
Methods
Participants
Our study included a total of 121 patients, aged 18 to 40 years, who underwent primary single-bundle hamstring tendon ACLR at our hospital from May 2020 to July 2023. The inclusion criteria were acute unilateral ACL rupture without other ligamentous injury or associated with mild meniscal tear (meniscal tears with little influence on joint stability postoperatively or reparable meniscal tears) or low-grade cartilage injury (mild edema and mild contusion on the cartilage surface) as confirmed by MRI and arthroscopy, a time span of <3 months from injury to surgery, and no history of injury or pain in the PFJ. The exclusion criteria were full-thickness chondral injuries of the knee; severe injury of the medial collateral ligament, lateral collateral ligament, or posterior cruciate ligament; severe meniscal tears, such as a radial split meniscal tear or full-thickness vertical longitudinal tear; a history of knee trauma or surgery. Approval for this prospective study was granted by the ethics committee of our hospital, and all patients provided written informed consent before participation.
Procedures and Postoperative Rehabilitation
All patients received a single-bundle hamstring tendon autograft ACLR, with Endobutton (Smith & Nephew) fixation on the femoral side and absorbable compression screw fixation on the tibial tunnel. An experienced sports medicine specialist (W.L.) performed the procedure arthroscopically, after a previously described surgical technique. 5 All patients underwent the same rehabilitation protocol, including early postoperative rehabilitation exercises guided by the same experienced rehabilitation team (M.Z.) after ACLR.
After the procedure, the knee was stabilized in an extended position with an adjustable brace. The patients returned to the ward and were instructed to begin ankle pump exercises, quadriceps femoris isometric contractions, and hamstring isometric contractions once sensation had returned after anesthesia. Postoperative ice packs helped alleviate knee swelling and discomfort.
Knee flexion exercises initiated at 2 weeks postoperatively. The ROM of the knee joint was expected to reach 90° at 4 weeks postoperatively and 120° at 6 weeks, and it was expected to reach 130° to 150°, aligning closely with normal levels by 12 weeks postoperatively. Full weightbearing was permitted at 6 weeks after surgery. Noncontact physical activities, such as jogging and jumping, were allowed at 3 months after surgery, with gradual resumption of sports activities thereafter.
Patients’ perception of pain during the early knee flexion exercises was documented daily by one professional rehabilitator (M.Z.) up to 6 weeks postoperatively and evaluated using a 10-point Numeric Rating Scale: 0 points, no pain; <3 points, mild endurable pain; 4 to 6 points, moderate pain that affected sleep but could be tolerated; and 7 to 10 points, intense pain that affected the appetite and sleep and was difficult to tolerate.4,37 The mean pain intensity experienced by patients throughout the 6-week rehabilitation program was calculated, and those with pain level <3 points were categorized into group A, those with scores ranging from 4 to 6 points were placed in group B, and individuals with scores between 7 and 10 points were allocated to group C.
Evaluation
An MRI assessment of the damaged knee joint was performed before surgery and 3 months postoperatively to evaluate the cartilage of the PFJ. A 3.0-T MRI scanner with a dedicated 8-channel knee coil was used to perform the examination. The protocol included sagittal and axial T2-weighted sequences with fat suppression and a slice thickness of 3 mm.
The semiquantitative MRI Osteoarthritis Knee Score 17 was used to score the degeneration of the patellofemoral cartilage. 39 This score is a validated tool developed to identify osteoarthritis and has been shown to be potentially more applicable to evaluation of the early stages of osteoarthritis and minor cartilage defects, defined as those with high signal intensity, fraying, or fissuring or hypertrophy. 38 The T2 mapping MRI sequence was used to quantify the cartilage composition. Studies have shown that higher T2 relaxation times indicate a deteriorated biochemical cartilage composition. 24
The presence of edema and high signal intensity changes in the patellofemoral articular cartilage were observed, and the T2-weighted mean relaxation times of specific regions of the patella and femoral trochlea such as the lateral condyle, medial condyle, trochlear groove, and both surfaces of the patella were calculated to evaluate the degeneration of the patellofemoral cartilage (Figure 1). All tasks were performed by 2 experienced blinded musculoskeletal radiologists, and the calculations were repeated at a 2-week interval. The reliability of the measurements and the agreement between the first measurement and the repeat measurement were assessed using the intraclass correlation coefficient (ICC).
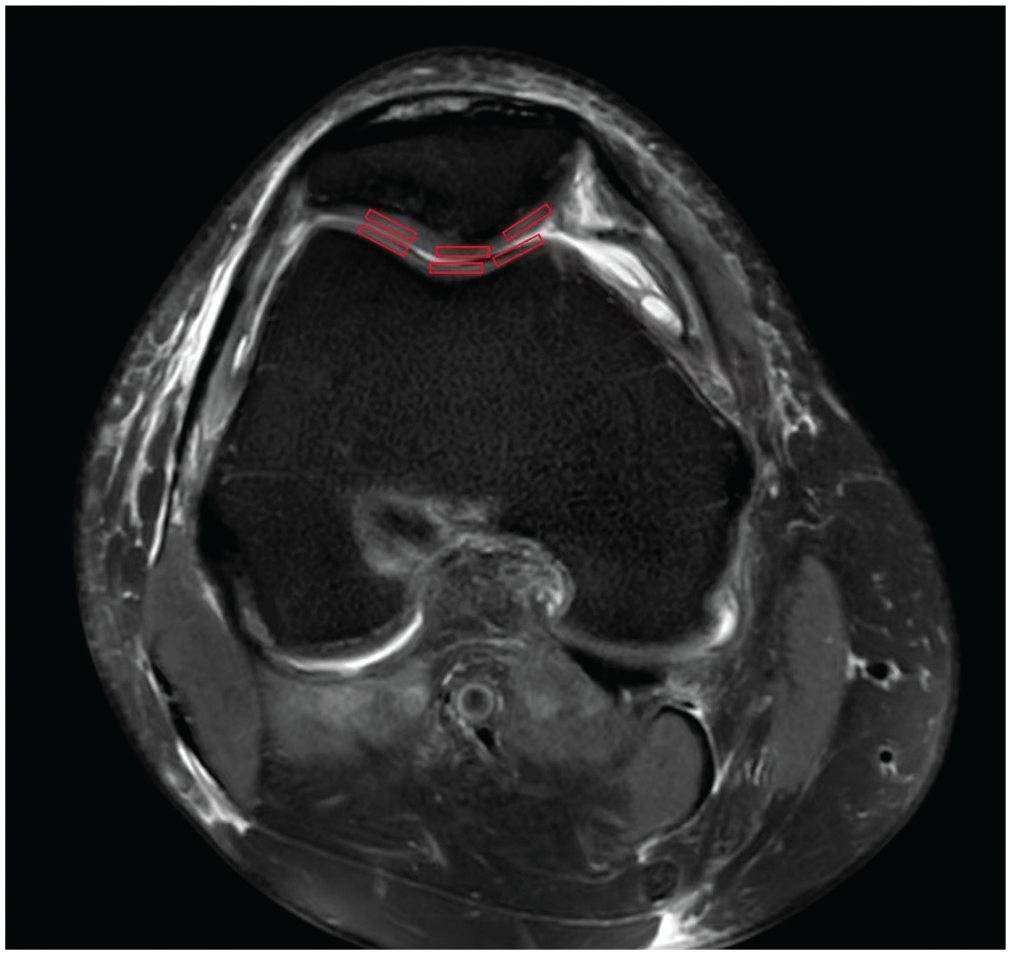
The specific regions of the patella and femoral trochlea (lateral surface of the patella and lateral condyle, ridge of the patella and trochlear groove, medial surface of the patella and medial condyle) as indicated by the red rectangles.
Subjective evaluations included preoperative and 3-month postoperative calculation of the International Knee Documentation Committee (IKDC) score, Knee injury and Osteoarthritis Outcome Score (KOOS), Lysholm score, and Kujala score. The IKDC score was used to evaluate the subjective and objective function of the knee joint after ACL injury and reconstruction. The KOOS score was used to evaluate the pain, symptoms, daily activities, sports, and recreational function of the knee after ACL injury and reconstruction. The Lysholm score was used to assess knee dysfunction in patients with ACL injury and reconstruction. The Kujala score was used to evaluate the pain around the knee after ACL injury and reconstruction.
Statistical Analysis
All statistical analyses were performed using SPSS Version 26.0 statistical software (IBM Corp). Descriptive statistics were used to summarize the data. We used the Shapiro-Wilk test to evaluate the normality of the distribution of each variable and Levene test to evaluate the homogeneity of the variance. Demographic data, scores, and functional performance test results were compared among the 3 groups using the chi-square test or one-way analysis of variance. A P value of <.05 was considered statistically significant.
Results
A total of 121 patients (82 men, 39 women) participated in our study. Their mean age at the time of ACLR was 26.9 ± 6.3 years. There were 36 patients categorized as group A, 52 patients as group B, and 33 patients as group C. There were no significant differences in the patients’ baseline characteristics among the 3 groups (Table 1). The MRI examination revealed that 3 (8.3%) patients in group A, 8 (15.4%) patients in group B, and 13 (39.4%) patients in group C exhibited edema and high signal intensity changes (Figure 2) in the patellofemoral articular cartilage at 3 months postoperatively. There were significant differences between groups A and C (P < .01) and between groups B and C (P < .05).
The Baseline Characteristics of the 3 Groups a

Data are presented as mean ± SD, n (%), or n. P1 represents the difference between group A and group B; P2 represents the difference between group A and group C; and P3 represents the difference between group B and group C. BMI, body mass index; ns, nonsignificant difference.

Cartilage degeneration occurred 3 months after anterior cruciate ligament reconstruction as indicated by the red arrows.
Compared with preoperatively, the T2 relaxation time of the femoral trochlear lateral condyle, trochlear groove, lateral surface of the patella, and ridge of the patella were significantly increased, especially in groups B and C, at 3 months postoperatively (Table 2). The T2 values of the femoral trochlear lateral condyle in groups A, B, and C were 31.5 ± 3.3, 32.9 ± 3.0, and 34.8 ± 3.0, respectively, at 3 months postoperatively. There were significant differences between groups A and B (P < .05), groups A and C (P < .01), and groups B and C (P < .01). The T2 values of the ridge of the patella in groups A, B, and C were 32.6 ± 3.3, 34.2 ± 4.0, and 36.0 ± 3.9, respectively, at 3 months postoperatively. There were significant differences between groups A and B (P < .05), groups A and C (P < .01), and groups B and C (P < .05). At 3 months postoperatively, the T2 values of the trochlear groove in groups A, B, and C were 32.8 ± 3.4, 34.7 ± 3.9, and 36.1 ± 4.0, respectively. There were significant differences in the T2 values between groups A and B (P < .05) and between groups A and C (P < .01). The T2 values of the lateral surface of the patella in groups A, B, and C were 32.9 ± 3.2, 34.4 ± 4.3, and 35.9 ± 3.7 at 3 months postoperatively. There were significant differences in the T2 values between groups A and C (P < .01) (Table 2). However, the changes in the femoral trochlear medial condyle and the medial surface of the patella were not significant at 3 months after the operation, and there were no significant differences among the 3 groups (Table 2). Excellent interobserver and intraobserver reliability was found for all measurements, with an ICC ≥ 0.78 (Table 3).
T2 Values of the Patella and Femoral Trochlea in the 3 Groups Preoperatively and at 3 Months Postoperatively a

Data are presented as mean ± SD. P1 represents the difference between group A and group B; P2 represents the difference between group A and group C; and P3 represents the difference between group B and group C. ns, nonsignificant difference.
Indicates significant difference between preoperatively and postoperatively (P < .05).
Intraobserver and Interobserver Reliability of T2 Value Measurements of Patella and Femoral Trochlea a

ICC, intraclass correlation coefficient.
The subjective evaluation showed that the knee function in the 3 groups was significantly improved compared with preoperatively and that the knee pain was significantly reduced (Table 4). However, the IKDC score, KOOS, Lysholm score, and Kujala score in group C were lower than those in groups A and B (especially group A), and there were significant differences between groups A and C (Table 4).
The IKDC, KOOS, Lysholm, and Kujala Scores Preoperatively and at 3 Months Postoperatively a

Data are presented as mean ± SD. P1 represents the difference between group A and group B; P2 represents the difference between group A and group C; and P3 represents the difference between group B and group C. IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; ns, nonsignificant difference.
Discussion
The most important finding of our study is that knee pain during early rehabilitation exercises after ACLR may be associated with severity of MRI appearances of the PFJ chondral changes and that more intense pain perception during early rehabilitation exercise is associated with more severity of MRI chondral changes of the PFJ.
PFP and PFOA are recognized complications after ACLR. Research indicates that the median prevalence of PFOA reaches nearly 50% within 10 to 15 years after ACLR.9,27 Many factors have been reported to contribute to PFOA after ACLR, including concomitant damage to the articular cartilage, quadriceps muscle weakness, meniscal resection, follow-up duration, sex, increased age at primary surgery, body mass index, and limitation of knee ROM.8,10,21 The progression of cartilage lesions in the PFJ after ACLR reportedly arises from biochemical and biomechanical alterations. 10 Altered PFJ loading in patients suffering from PFP and PFOA has been suggested to contribute to the development of these abnormalities.14,42 Lee et al 21 identified diminished quadriceps strength after ACLR as a significant risk factor for PFP and PFOA. Weakened quadriceps strength can easily cause instability of the PFJ, leading to subsequent development of PFOA.
In the current study, patients underwent division into 3 categories after ACLR based on pain intensity during rehabilitation exercises. MRI assessments indicated evidence of PFJ cartilage deterioration 3 months after ACLR. Notably, increased pain during rehabilitation correlated with a greater prevalence of cartilage damage. Because of alterations in cartilage composition during the early phases of osteoarthritis, the utilization of quantitative MRI metrics has been recommended as a reliable indicator for early osteoarthritis investigations.15,23 The T2 relaxation time serves as a crucial imaging indicator for the quantitative assessment of macromolecules in early osteoarthritis, 28 and research indicates that patients with early osteoarthritis exhibit significantly elevated T2 values. 34 In our study, the T2 values of the femoral trochlear lateral condyle, trochlear groove, lateral surface of the patella, and ridge of the patella were significantly increased, especially in groups B and C, at 3 months postoperatively compared with preoperatively. Additionally, the T2 values of the femoral trochlear lateral condyle, trochlear groove, lateral surface of the patella, and ridge of the patella were higher in group C than in groups A and B. Heightened pain perception during rehabilitation exercises correlated with increased degeneration of the PFJ. We attribute this primarily to the intense contraction of the quadriceps femoris muscle triggered by painful stimuli during initial knee flexion exercises. This contraction sharply elevates stress on the PFJ. Research indicates that enhanced contraction force of the quadriceps femoris during knee flexion results in heightened PFJ stress. 18 A prevailing theory holds that PFP develops in response to increased PFJ stress.11,16,25,30 Our research indicated that the T2 values for the medial condyle of the femoral trochlea and the medial surface of the patella did not undergo significant alterations by 3 months postoperatively. Furthermore, there were no notable differences among groups A, B, and C. These findings suggest that the initial degeneration in the PFJ primarily occurs in the lateral condyle of the femoral trochlea and the lateral surface of the patella. This phenomenon may relate to the patellar tracking and inclination during knee flexion. Research has demonstrated that the lateral articular surface of the patella first engages with the lateral side of the femoral trochlea during knee flexion, and when knee flexion surpasses 45°, the medial articular surface begins to interact with the medial surface of the femoral trochlea.3,40
The subjective evaluation showed that in all 3 groups, knee function was significantly improved compared with the preoperative period, and knee pain was significantly reduced. However, the functional and pain scores in the patients who experienced severe pain during rehabilitation exercises were lower than those in the patients with mild pain. These results indicate that patients with higher pain scores may have slower functional recovery and tend to have poorer function in the early postoperative period.
Limitations
Our study had 3 main limitations. First, we did not analyze the causes of the patients’ pain. There were numerous potential causes of the pain experienced during the rehabilitation exercises: the tightness of the ACL graft was not appropriate and may have affected the results of the study. Second, the follow-up period was relatively short, and although MRI showed abnormalities in the patellofemoral articular cartilage, the patients showed no obvious symptoms of patellofemoral arthritis. The correlation between early changes and the later incidence of patellofemoral arthritis requires further investigation. Third, we did not directly measure the strength of the quadriceps femoris muscle and the pressure changes of the PFJ during the early knee flexion exercises of the patients after ACLR.
Conclusion
Our study indicates that knee pain during early rehabilitation exercises is associated with MRI changes in the PFJ, and more intense pain perception during early rehabilitation exercises is associated with more severe change.
Footnotes
Acknowledgements
The authors would like to thank the hospital for supporting this study and our colleagues at the MRI room of Hardison International Peace Hospital for their help.
Final revision submitted January 15, 2025; accepted February 11, 2025.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Harrison International Peace Hospital (2022-3-023).