
Abstract
Background:
Anterior cruciate ligament (ACL) injuries are common among active patients and can be managed with primary repair or reconstruction. The most important predictor of good outcomes after primary repair is a more proximal tear location. Preoperative magnetic resonance imaging (MRI) guides surgical decision making, but the accuracy of MRI in identifying tear location is understudied.
Purpose:
To evaluate the accuracy of preoperative MRI in identifying ACL tear location.
Study Design:
Cohort study (diagnosis); Level of evidence, 2.
Methods:
Patients who underwent ACL reconstruction or repair by 2 surgeons at a single, urban academic medical center between 2019 and 2024 were collected. Exclusion criteria included previous ACL surgery and inadequate preoperative or intraoperative imaging. The location of the ACL tear on preoperative MRI scan was retrospectively graded using the modified Sherman classification in a blinded manner. Reference diagnosis was the tear location as noted in the surgeon’s operative note and confirmed with arthroscopic images. The primary endpoint was the accuracy of MRI for predicting intraoperative tear type.
Results:
A total of 203 patients were included in this study. MRI accurately predicted the ACL tear type seen arthroscopically only 35.5% (72/203) of the time. When MRI did not match the arthroscopic diagnosis, the MRI was within 1 classification grade 74.8% (98/131) of the time. Of the incorrect gradings, 71.0% (93/131) were overclassifications (MRI tear classification more distal than found during arthroscopy). MRI was more sensitive in detecting proximal third (type II) and midsubstance (type III) tears (43.7% and 51.6%, respectively) than it was for detecting proximal avulsion (type I) tears (2.5%).
Conclusion:
MRI was unreliable for determining the precise location of an ACL tear. MRI tended to overestimate how distal a tear was compared with arthroscopic findings, which may influence patient counseling, preoperative planning, and surgical decision making.
The anterior cruciate ligament (ACL) is a double bundle of type 1 collagen that provides restraint against anterior translation and rotation in the native knee. The ACL is most commonly injured during noncontact cutting and pivoting sports but can also be ruptured during a valgus-producing direct blow to the knee. These injuries are common, with up to 200,000 occurring each year in the United States. 3 Complete ruptures of the ACL can occasionally be managed nonoperatively in lower demand, older patients without clinically demonstrable instability. In young, active patients with instability, surgical intervention is a consensus recommendation. 9 ACL reconstruction (ACLR) is the gold standard treatment, with excellent outcomes.4,8
Recently, the literature has witnessed a resurgence of studies regarding primary ACL repair. Large meta-analyses and systematic reviews have demonstrated that primary repair has failure rates equivalent to those of ACLR and excellent functional outcomes, particularly for proximal avulsion type tears.15,17 Given the prognostic effect of tear location on the efficacy of ACL repair, correct preoperative identification of tear location is essential for preoperative planning and patient counseling. Van der List et al 14 modified an existing classification of ACL tear types developed by Sherman et al 10 and validated this grading system for use with magnetic resonance imaging (MRI). Type I is a proximal avulsion, with the tear occurring <10% of the proximal-distal length of the ACL from the femoral insertion. Type II is a proximal tear occurring at 10% to 25% of the proximal-distal length. Type III, which is the most common, is a midsubstance tear located at the middle 25% to 75% of the ligament. Type IV is a distal tear located at 75% to 90% of the proximal-distal length. Finally, type V is a distal avulsion occurring at 90% or greater of the length from the femoral insertion. The authors demonstrated durable interrater reliability in the application of this classification system to the MRI scans of ACL tears. 14
Although the modified Sherman MRI classification is easily applicable, it is not clear whether its interpretation corresponds accurately to the tear encountered arthroscopically and, moreover, whether the surgeon’s surgical plan would remain the same. One study demonstrated that 90% of type I tears and 46% of type II tears designated on MRI could be repaired primarily. 13 However, that investigation did not analyze the agreement between MRI and arthroscopy on the location of the tear. In a study of 34 patients who underwent primary repair of the ACL, all of whom had type I proximal avulsions, MRI was only 9% sensitive for identifying these lesions. 11 Finally, in a study of 71 patients undergoing repair or reconstruction, MRI was shown to be 70% accurate in identifying all tear types encountered arthroscopically. 7 These data suggest that the ability of MRI to identify the precise location of an ACL tear is questionable and that its correspondence to arthroscopic findings is understudied. The senior authors of our study (S.M., J.N.G., and S.G.A) have frequently encountered reparable, proximal avulsion tears that were misidentified as midsubstance on MRI, prompting the current investigation.
The goal of our study was to evaluate the accuracy of preoperative MRI in predicting ACL tear location subsequently identified arthroscopically, as this information may guide patient counseling, preoperative planning, and surgical decision making for surgeons using both repair and reconstruction techniques. We hypothesized that MRI would tend to underestimate the remaining length of ACL stump tissue compared with arthroscopic examination.
Methods
Study Design
This retrospective study was approved by our institutional review board (STUDY-23-01140). Patients undergoing primary ACLR or repair by 2 surgeons (J.N.G and S.G.A) at an urban academic medical center between 2019 and April 2024 were included and identified using Current Procedural Terminology (CPT) code 29888. Patients without adequate intraoperative arthroscopic images or preoperative MRI scans were excluded, as were patients undergoing revision ACLR and patients who had tibial spine avulsion, previous hardware, or a congenital absence of the ACL.
Data Collection
Demographic characteristics, procedure type (repair or reconstruction), and imaging-related time statistics were collected for each patient. Demographic characteristics included patient age at the date of the procedure, sex, and body mass index (BMI). Imaging-related data included the number of days between the patient’s injury and the preoperative MRI scan and the number of days between the patient’s preoperative MRI scan and ACL procedure
ACL stump morphology was assessed on preoperative MRI scans in a blinded manner by the 2 principal investigators (J.N.G and S.G.A) who operated on the patients in this study, both of whom are sports medicine fellowship–trained orthopaedic surgeons with >30 years combined experience. Although imaging was conducted at different sites, all patients were imaged with a 3.0-T MRI machine, and the ACL was analyzed on T1-weighted, T2-weighted, and proton density–weighted sequences in the sagittal, coronal, and axial planes. The tear type was classified by location using the modified Sherman grading system: type I (proximal avulsion, >90% of tibial length remaining), type II (proximal tear, 90%-75% length remaining) type III (midsubstance, 75%-25% length remaining), type IV (distal tear, 25%-10% length remaining), and type V (distal avulsion, <10% length remaining). 14 The reference grade was the arthroscopic assessment of the stump tissue, which was retrospectively gathered from the surgeon’s operative note and cross-checked against the patient’s arthroscopic images. The agreement between classification grades on MRI and arthroscopy was then assessed. Inaccurate MRI predictions were further analyzed for being within 1 classification grade different than intraoperative arthroscopic imaging or >1 grade.
Statistical Analysis
Demographic characteristics, procedure type, and imaging-related characteristics were tabulated for the study population overall, the cohort of patients with accurate MRI predictions, and the cohort with inaccurate MRI predictions. Patient age, BMI, interval between injury and MRI, and interval between MRI and arthroscopy were reported as median with interquartile range (IQR). Mann-Whitney U tests were used to compare continuous data between cohorts, including patient age, BMI, interval between injury and MRI, and interval between MRI and arthroscopy, because the data were not normally distributed. Chi-square tests were used to compare categorical data, including patient procedure type and patient sex. The sensitivity, specificity, positive predictive value, and negative predictive value of MRI were calculated for each tear type. Data analysis was performed using IBM SPSS Statistics Version 24.
Results
A total of 276 consecutive patients were identified using the CPT code 29888 in the practices of 2 senior authors over the last 5 years. After we excluded 37 patients with inadequate arthroscopic images for review, 17 patients who had undergone revision ACL surgeries, 15 patients with inadequate or inaccessible MRI scans, 2 patients who had bony avulsions of the tibial spine, 1 patient who had previous hardware that obscured imaging review, and 1 patient who had a congenitally absent ACL, the final sample size was 203 patients (Figure 1).

CONSORT (Consolidated Standards of Reporting Trials) diagram. ACL, anterior cruciate ligament; MRI, magnetic resonance imaging.
The median patient age at the time of surgery in our sample was 29 years (IQR, 13 years). The median BMI was 25.1 (IQR, 6.1). The median time from injury to MRI was 12 days (IQR, 36 days), and the median time from MRI to surgery was 43 days (IQR, 72 days). In total, 46.3% of the sample population was female, and 73.9% underwent ACLR, whereas 26.1% received a primary repair. No significant differences were found across any of these demographic parameters for the cases in which MRI correctly identified the tear type compared with when it did not. These data are summarized in Table 1.
Characteristics of Patient Cohorts With Accurate Versus Inaccurate Preoperative MRI Predictions of ACL Tear Type Observed Intraoperatively a

Data are expressed as median (interquartile range) unless otherwise noted. ACL, anterior cruciate ligament; MRI, magnetic resonance imaging.
When diagnosing the injuries arthroscopically, we found 40 type I tears (19.7%), 87 type II (42.9%), 62 type III (30.5%), 12 type IV (5.9%), and 2 type V (0.99%). A representative image of each tear type as seen arthroscopically is shown in Figure 2. In comparison, MRI predicted 6 type I tears (2.96%), 86 type II (42.4%), 94 type III (46.3%), 17 type IV (8.37%), and 0 type V. A representative image of each tear type as seen on MRI is shown in Figure 3.
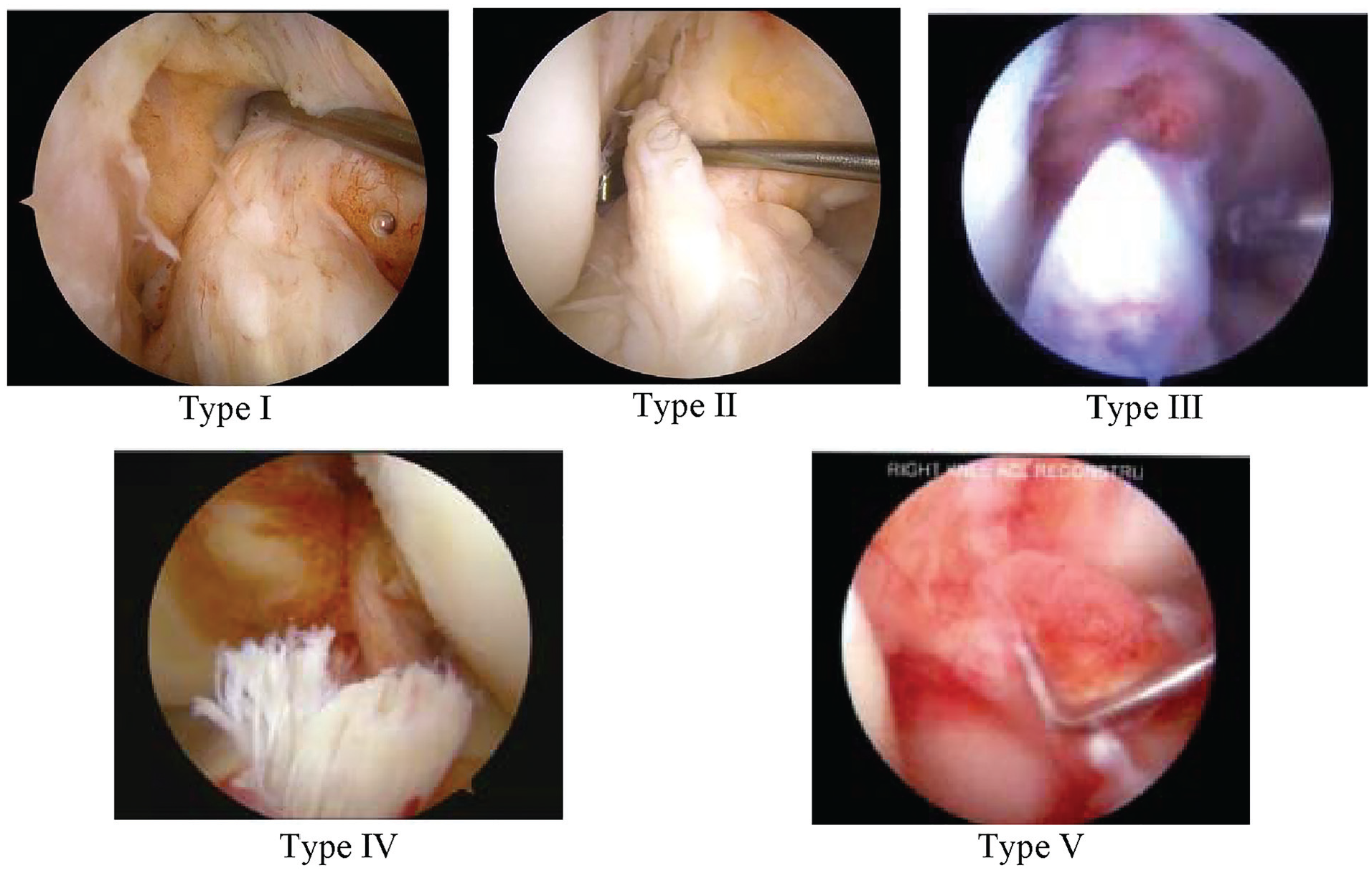
Arthroscopic image representation of each modified Sherman tear type.

Magnetic resonance image representation of each modified Sherman tear type.
The primary endpoint of this study was the accuracy of MRI in diagnosing the correct tear type discovered during surgery. Of the 203 patients in this study, MRI correctly identified the tear location in 35.5% (n = 72). When it failed to identify the correct tear type, MRI was within 1 tear classification grade 74.8% of the time (98/131). When it was incorrect, MRI overestimated the classification grade (perceived the tear to be more distal) 71.0% of the time (93/131). These data are depicted in Table 2. Further stratified by each tear type, MRI was more sensitive in detecting type II (43.7%) and type III tears (51.6%) than proximal avulsions (2.5%). These statistics are displayed in entirety in Table 3.
Accuracy of Preoperative MRI Predictions of ACL Tear Type Observed Intraoperatively a

ACL, anterior cruciate ligament; MRI, magnetic resonance imaging.
Distribution of ACL Tear Type Classifications From Preoperative MRI Scans and Intraoperative Arthroscopic Images a

ACL, anterior cruciate ligament; MRI, magnetic resonance imaging; NPV, negative predictive value; PPV, positive predictive value.
Proximal tears (types I and II) have historically been considered better candidates for repair. We studied how often MRI predicted a midsubstance or distal tear, which was subsequently found to be proximal during surgery. Of 111 midsubstance to distal tears diagnosed on MRI, 64 (57.7%) were found to be proximal tears during diagnostic arthroscopy. This suggests that relying on preoperative MRI alone to recommend ACLR for a midsubstance to distal tear would result in a missed opportunity to use ACL preservation techniques more than half the time.
Discussion
This study aimed to evaluate how reliable preoperative MRI scans are in classifying the location of ACL tears, as this information can be used to help plan surgeries and make treatment decisions. In our group of patients, arthroscopic examination showed that most ACL tears were type II (42.9%), type III (30.5%), or type I (19.7%). These proportions have been seen in previous studies as well.7,14 The MRI correctly identified the type of ACL tear in only 35.5% of cases but predicted the tear to be within 1 classification grade 74.8% of the time. Patient characteristics like age, BMI, time to MRI, and time to surgery did not show significant differences between tears that MRI accurately and inaccurately identified.
It was anticipated that MRI would underestimate the remaining length of the tibial stump, and the results supported this, as MRI incorrectly classified the tear type in 71.0% of cases. When MRI failed to identify the correct tear location, the MRI classification was typically more distal than discovered during arthroscopy. Additionally, sensitivity, specificity, positive predictive value, and negative predictive value were calculated for each tear type. MRI had the highest sensitivity for predicting type III (56.61%) and type II (43.68%) tears. In contrast, MRI was poorly sensitive for detecting type I tears (2.5%). This is even lower than the 8.8% sensitivity published previously. 11
Although MRI is both a sensitive and a specific test for diagnosing complete ACL tears, 2 the literature has shown that MRI has a diminished ability to identify nuances in injuries to the ACL. Multiple studies assessing complete versus partial ACL tears have found limitations including poor accuracy and low sensitivity of MRI in distinguishing between the two.6,12,16,19 Shu et al 11 conducted a retrospective review similar to the present study to assess whether preoperative MRI could predict ACL tear type later identified arthroscopically. The accuracy and sensitivity of MRI for type I tears were just 8.8% and 9%, respectively, compared with a sensitivity of 2.5% in the present study. Their investigation had a smaller cohort of patients (N = 34) and included only patients who received ACL repair, and all tears were found to be type I proximal avulsions. Most similar to our investigation, Mehier et al 7 analyzed 71 patients who underwent ACL repair or reconstruction and retrospectively compared the MRI tear location to the arthroscopic reference diagnosis. Those authors reported a 70% diagnostic accuracy of MRI when the images were read by musculoskeletal radiologists with a minimum of 10 years of experience. However, the sample size in that investigation was smaller than our study, and the authors did not comment on which direction MRI erred when it failed to correctly identify the tear location.
The principal finding of the current study is that ACL tear location and stump morphology are difficult to assess accurately on preoperative MRI. This is significant because this information is critical in determining eligibility for ACL-preserving techniques. Given the low interobserver reliability among orthopaedic surgeons for the determination of ACL tear location, tissue quality, and decision for repair versus reconstruction based on preoperative MRI, 1 our study further corroborates that although MRI can help approximate the location of an ACL tear, a thorough examination of stump tissue intraoperatively should precede the final decision making. For example, a relatively high percentage of our cohort (26%) underwent a primary repair of their torn ligament, secondary to the preference of the senior authors to treat primary avulsions with biologically augmented primary repair. This is consistent with roughly 20% of our patients having a type I proximal avulsion as seen on diagnostic arthroscopy. However, only 3% of MRI diagnoses were proximal avulsions, reinforcing that primary repair would not have occurred as frequently if final procedural decision making preceded arthroscopic tear assessment.
The current study has a few limitations. First, it was a retrospective study, which may have led to differences in how surgeons recorded the length of the stump tissue. However, we confirmed tear classifications using arthroscopic images to reduce this potential bias. Previous research has shown substantial agreement (kappa = 0.79) for ACL stump length as assessed arthroscopically by fellowship-trained orthopaedic sports medicine surgeons.5,18 Second, the arthroscopic images used to confirm tear grades were static and 2-dimensional. During surgery, arthroscopic examination of the ACL tear is a dynamic process that involves probing and manipulating the remnant ligament. As arthroscopic videos were not available for review, we used the accessible intraoperative arthroscopic images to verify the location of the ACL tear, which may have limited the accuracy as compared with live arthroscopic assessment. Third, MRI scans were graded by the principal investigators of the study, who are both fellowship-trained sports medicine orthopaedic surgeons. This differs from a study by Mehier et al, 7 which involved senior musculoskeletal radiologists and found superior diagnostic accuracy of MRI. It is possible that having orthopaedic surgeons read the MRI scans may have reduced the modality’s diagnostic accuracy, but this approach enhances the study’s generalizability because most MRIs are interpreted by the treating surgeon in the clinical setting during surgical indication.
Conclusion
Our study demonstrates that MRI was unreliable for determining the precise location of an ACL tear. MRI overestimated how distal a tear was, which may influence surgical decision making. Surgeons should discuss ACL repair and reconstruction options with patients preoperatively and assess the remnant stump tissue arthroscopically before making a final determination.
Footnotes
Final revision submitted December 4, 2024; accepted January 10, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.G.A. is a consultant for Smith & Nephew, has equity in Manhattan Surgery Center, and has received education payments from Gotham Surgical Solutions & Devices and Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Mount Sinai Health System Institutional Review Board (STUDY-23-01140).