
Abstract
Background:
The anterolateral ligament (ALL) contributes to anterolateral rotational stability of the knee. Internal bracing of the anterior cruciate ligament (ACL) and ALL reinforces the ligaments and encourages natural healing by protecting both during the healing phase and supporting early mobilization.
Purpose/Hypothesis:
To assess the 2-year patient-reported outcomes of combined ACL repair and ALL internal brace augmentation. We hypothesized that significant improvements in outcomes would be seen.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 43 consecutive patients with acute proximal ACL ruptures were prospectively evaluated for a minimum of 2 years. The mean age at the time of surgery was 25.7 years (range, 13-56 years). Indications for the combined ACL/ALL procedure were associated Segond fractures, grade 3 pivot shift, or high levels of sporting activity. Patients with chronic ruptures or with multiligament injuries were excluded. The Knee injury and Osteoarthritis Outcome Score (KOOS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), visual analog scale (VAS) for pain, Veterans RAND 12-Item Health Survey (VR-12), and Marx activity scale were collected preoperatively and at 12 and 24 months postoperatively. Patients with any postoperative complications were identified at the time of this analysis.
Results:
The mean follow-up period was 44.8 months. Five patients were lost to follow-up, leaving 38 patients (88.4%) in the final analysis. The mean KOOS for Pain, Symptoms, Activities of Daily Living, Sport/Recreation, and Quality of Life improved from a respective 64.9, 58.6, 75.0, 33.7, and 28.9 preoperatively to 91.1, 81.8, 96.1, 82.8, and 74.3 at the 2-year follow-up (P < .0001). The mean WOMAC scores for pain, stiffness, and function improved from 77.5, 65.3, and 75.0 preoperatively to 94.6, 88.6, and 96.0 at the 2-year follow-up (P < .0001). The VAS pain score improved from 3.4 preoperatively to 0.7 at the 2-year follow-up, and the VR-12 physical score improved from 34.4 preoperatively to 52.7 at the 2-year follow-up (P < .0001 for both ). However, the Marx activity score decreased from 13.3 preinjury to 10.6 at the 2-year follow-up (P = .01). Two patients (5.3%) sustained a rerupture.
Conclusion:
Combined ACL repair and ALL internal brace augmentation demonstrated excellent outcomes in 94.7% of the study patients. Based on our experience with this cohort as well as our isolated ACL repair data, we suggest that high-risk patients with ACL ruptures have an additional ALL procedure to provide rotational stability.
Keywords
Primary repair of the ACL was the primary surgical treatment for ACL ruptures in the 1970s and 1980s. 8,29,38 However, high failure rates were described at midterm follow-up, 7,9,20 and as a result, ACL reconstruction became the gold standard treatment in the 1990s. 2,6 Reconstruction is still widely practiced today, despite a number of associated problems, including the loss of proprioception, graft harvest morbidity, posttraumatic osteoarthritis, and graft failure. Recent advancements in arthroscopic instrumentation, suture materials, imaging, and rehabilitation protocols, in addition to an enhanced understanding of ACL healing, could lead to improved outcomes with primary repair of the ACL for selected patients with a proximal ACL rupture when compared with traditional techniques.
Although the debate on the exact anatomy and function of the anterolateral complex is ongoing, recent insights into the structure and function of the anterolateral ligament (ALL) of the knee have resulted in growing evidence of its role in rotational control of the knee. 4,24,31 There is a close association with anterior cruciate ligament (ACL) ruptures, and it has been reported that 90% of ACL ruptures also have an injury to the ALL complex. 10,11,37
Several indications for ALL reconstruction or repair have been described: an ALL rupture combined with an ACL rupture, chronic ACL lesions, an ACL rupture with a grade 3 pivot shift, high-demand athletes, and revision ACL surgery. 33 Multiple ACL reconstruction and repair techniques, in combination with ALL reconstruction, have been described in the literature. 25 Historically, anterolateral extra-articular stabilization was the procedure of choice. Most of these techniques were nonanatomic reconstructions and used a part of the iliotibial band, possibly causing overconstraint of the joint. 18 More recently, several techniques for anatomic ALL reconstruction have been described. 25 Most of these techniques use a tendon autograft, usually semitendinosus or gracilis, which has been shown to control internal rotation of the tibia but is associated with the disadvantage of donor site morbidity. 33
Internal bracing involves the augmentation of a ligament repair with suture tape, which reinforces the ligament and promotes natural healing by protecting the ligament during the healing phase and allowing early mobilization. 21 As a tendon graft is not required, the risk of morbidity associated with harvesting is absent. Postoperatively, patients are mobilized early without the need for external bracing. However, no clinical studies have been published that determine the outcomes of this technique.
This study describes the 2-year outcomes of combined ACL repair and ALL internal brace augmentation in high-risk patients with a grade 3 pivot shift, a high preinjury level of sporting activity, or an associated Segond fracture. We hypothesized that there would be significant improvements in patient-reported outcome measures (PROMs) at 2 years postoperatively.
Methods
Patient Selection
Approval to conduct this study was obtained through the University of Strathclyde institutional review board. Between April 2014 and March 2017, a total of 43 consecutive patients with an acute proximal ACL rupture were evaluated within 6 weeks of injury. These patients underwent a combined ACL repair and ALL internal brace augmentation technique and were included in this study. Inclusion criteria were those patients who had an associated Segond fracture identified on preoperative radiographs, a grade 3 pivot shift, or a high preinjury level of sporting activity. Patients who had acute proximal ACL ruptures without the above risk factors underwent isolated ACL repair, and patients with midsubstance and distal ACL ruptures or retracted ACL remnants underwent a standard ACL reconstruction in this time frame. This decision was made at the time of surgery based on the tear location and the ACL tissue quality. Patients with multiligament knee injuries or chronic ruptures were excluded (Figure 1). Five patients were lost to follow-up, leaving 38 patients (88.4%) in the final analysis.

Study enrollment flowchart. ACL, anterior cruciate ligament; ALL, anterolateral ligament.
Surgical Technique
The patient was placed in a supine position with a tourniquet on the upper thigh. Standard anterolateral and anteromedial portals were used, and a passport cannula (Arthrex) was placed in the anteromedial portal for suture management and to prevent interposing tissues. The ACL was probed to assess its suitability for primary repair. Proximal ruptures of the ACL were repaired with internal bracing. The ACL remnant was left intact, and a standard tibial ACL guide was placed at the center of the ACL footprint. A small skin incision was made above the pes anserinus, and a 3.5-mm tibial tunnel was drilled. The drill was subsequently exchanged for a FiberStick (Arthrex), and a suture grasper was used to take the FiberWire suture (Arthrex) out of the FiberStick and through the medial portal. A FiberLink (Arthrex)was passed through the midsubstance of the ACL stump using a Scorpion suture passer (Arthrex) and retracted through the medial portal, forming a lasso around the distal ACL stump. The femoral attachment was then identified, microfracturing was performed, and a 3.5-mm femoral tunnel was then drilled. The FiberLink suture and the FiberWire suture were then passed through the femoral tunnel. A femoral button (Retrobutton or TightRope RT; Arthrex) loaded with FiberTape (Arthrex) was subsequently transported proximally through the tibial tunnel, the center of the ACL, and the femoral tunnel. The button was flipped on the femoral cortex and the FiberTape was advanced in the femoral tunnel by pulling the 2 tensioning strands. The suture tape was fixed distally, just below the tibial tunnel, using a 4.75-mm SwiveLock (Arthrex) loaded with both ends of the FiberTape. Before insertion, the FiberTape was marked at the laser line and repositioned in the eye of the SwiveLock to avoid additional tension; it was secured in full extension. Finally, the ACL was gently tensioned using the cinch to approximate it to the femoral footprint, and the FiberLink was then tied on the femoral button with the appropriate tension on the ACL. 16
Now, we turn our attention to the ALL internal brace augmentation. 17 This is a percutaneous technique. The lateral femoral epicondyle, distal joint line, Gerdy tubercle, and anterior margin of the fibular head were palpated and marked. The tibial insertion was marked halfway between the Gerdy tubercle and the anterior margin of the fibular head, 15 mm distal to the joint line.
A 3-cm incision was made starting over the lateral femoral epicondyle in a posterior and proximal direction, and the iliotibial band was split in line with its fibers. The femoral origin of the ALL was approximately 7 mm posterior and proximal to the lateral epicondyle. After predrilling with a 4.5-mm drill and a 20-mm drill stop, followed by tapping, a 4.75-mm bone anchor loaded with FiberTape was placed. The femoral drill hole was kept under direct vision to avoid superficial placement of the bone anchor in the bone or loss of the drill hole position.
A hemostat was directed distally under the iliotibial band, superficial to the lateral collateral ligament. To break any adhesions, the hemostat was distally moved sideways to create a tunnel for the FiberTape. The skin was incised over the tip of the hemostat at the previous marked ALL insertion. Using a lead suture transported by the hemostat, we brought the suture tape to the tibial incision. Under direct vision of the bony ALL insertion location, the 3.5-mm bone anchor was predrilled and tapped, with the tap left in place. A 3.5-mm anchor provided sufficient strength in the strong tibial bone and was preferred over larger sizes, given the proximity of the joint.
The suture tape was placed around the tap with the knee in flexion, followed by a full range of movement to ensure that full extension could be achieved. The FiberTape was loaded in the distal bone anchor and measured with the knee positioned in 90° of flexion with no additional tension and the foot in neutral rotation. The suture tape was marked at the laser line, which allowed for the length of the screw. It was repositioned in the eye of the bone anchor at the marked level, and finally, the bone anchor was placed in the drill hole. This prevented additional tension from being applied and overconstraint of the lateral compartment (Figure 2).
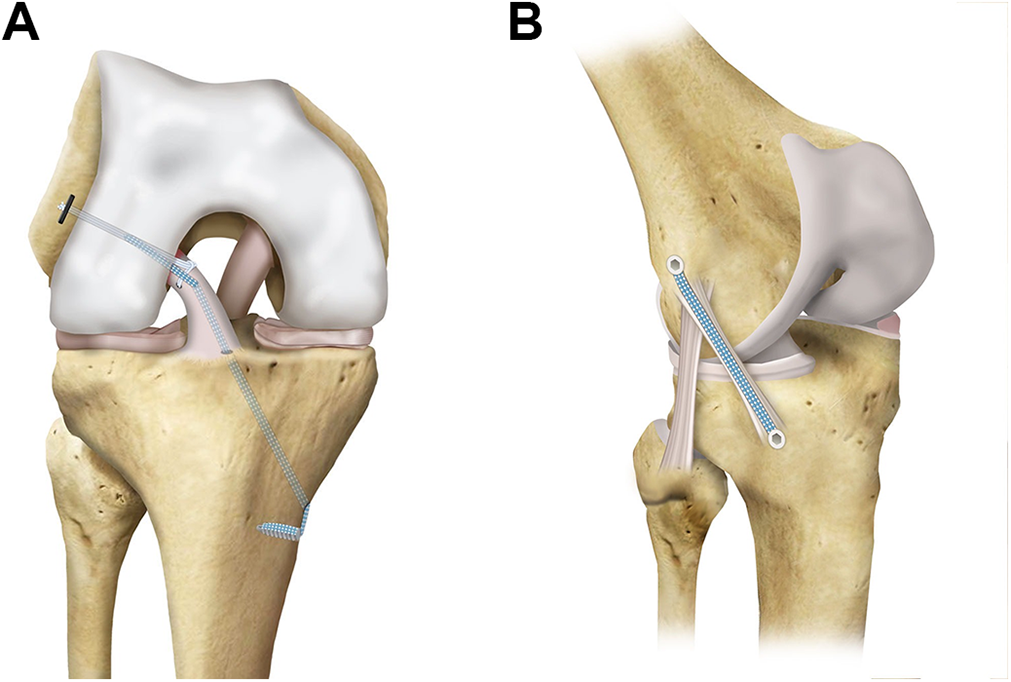
The final construct demonstrates combined internal bracing of the (A) anterior cruciate ligament (ACL) and (B) anterolateral ligament (ALL) with internal brace augmentation.
The patients followed our routine accelerated ACL rehabilitation program under the guidance of physical therapy. Initially, this focused on early range of movement, muscle control, and restoration of function. This was facilitated by limited pain and swelling, allowing accelerated early-phase rehabilitation. No external brace was required.
Clinical and Functional Evaluation
Patients were evaluated in the outpatient clinic for 6 months postoperatively. All patients were evaluated through manual clinical examination using Lachman and pivot-shift tests. No further testing was performed at that time.
Patients were evaluated prospectively using the Surgical Outcome System (SOS; Arthrex). SOS is a web-based tool that sends questionnaires and PROMs via email at scheduled time points. The collected PROMs were the Knee injury and Osteoarthritis Outcome Score (KOOS); the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), which was aimed more at our longer-term follow-up; the visual analog scale (VAS) for pain (0-10; 10 = worst pain); the Veterans RAND 12-Item Health Survey (VR-12) to assess patient physical and psychological health status; and the Marx activity scale for patient activity level. 5,22,23,27,28 These data were collected preoperatively and at 12 and 24 months postoperatively. Additionally, a standard questionnaire was completed to ask patients who did not have any further surgery about their overall satisfaction with regard to reducing pain, improving movement, resuming normal function, and resuming sport. All of the patients were also contacted by email/telephone at the time of this analysis to collect data about any complications.
Data Analysis
Descriptive statistics were expressed as means ± SDs with ranges. Analysis of variance was used to compare the pre- and postoperative PROMs after exclusion of any patients suffering from a rerupture and confirmation of normally distributed data using a Shapiro-Wilk test. Tukey-Kramer testing was used to compare all pairs. Results were considered significant if P < .05. All analyses were performed with JMP, Version 14 (SAS Institute Inc).
Results
The mean age for the 38 study patients was 25.7 ± 10.1 years (range, 13-56 years) at the time of surgery; there were 21 male and 17 female patients. The mean follow-up was 44.8 ± 9.1 months (range, 24-59 months).
All patients were found to have a stable knee on manual clinical examination (Lachman and pivot-shift tests) when reviewed in the outpatient clinic 6 months postoperatively. No further clinical testing was performed.
Outcome Measures
At the 2-year follow-up, all KOOS subsections demonstrated significant improvements (Figure 3). From preoperatively to the 2-year follow-up, the scores for each KOOS subsection were as follows: Pain, 64.9 ± 15.1 to 91.1 ± 11.1; Symptoms, 58.6 ± 17.3 to 81.8 ± 15.7; Activities of Daily Living, 75.0 ± 15.2 to 96.1 ± 8.3; Sport/Recreation, 33.7 ± 23.9 to 82.8 ± 19.5; and Quality of Life, 28.9 ± 13.9 to 74.3 ± 24.4 (P < .0001 for all). No significant differences were seen between the 1- and 2-year time intervals on any KOOS subsection.
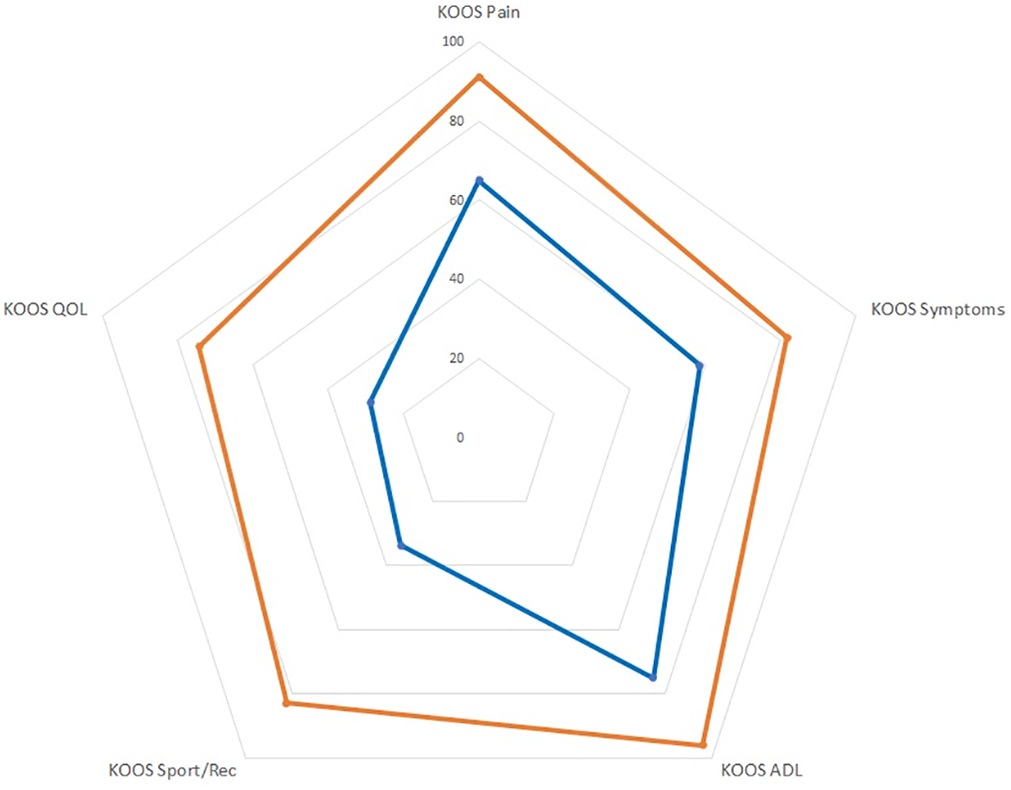
Spider chart demonstrating significant improvements at the 2-year follow-up (orange line) in all subsections of the Knee injury and Osteoarthritis Outcome Score (KOOS). ADL, Activities of Daily Living; QOL, Quality of Life; Rec, recreation.
All sections of the WOMAC demonstrated significant improvements at the 2-year follow-up (Figure 4). From preoperatively to the 2-year follow-up, the WOMAC for pain scores were 77.5 ± 15.5 to 94.6 ± 8.9, the WOMAC for stiffness scores were 65.3 ± 21.1 to 88.6 ± 17.4, and the WOMAC for function scores were 75.0 ± 15.2 to 96.0 ± 8.4 (P < .0001 for all). No significant differences were seen between the different postoperative time intervals for any of the WOMAC subsections.

Spider chart demonstrating significant improvements at the 2-year follow-up (orange line) in all subsections of the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score.
The VAS for pain decreased significantly from 3.4 ± 1.9 preoperatively to 0.7 ± 1.3 at the 2-year follow-up (P < .0001) (Figure 5). No significant differences were seen between the 1- and 2-year postoperative time intervals.

Chart demonstrating a significant decrease in visual analog scale (VAS) pain scores from preoperatively to 2 years postoperatively. The median, interquartile range, and range are illustrated in the box plot.
The VR-12 physical score was 34.4 ± 9.5 preoperatively, increasing significantly to 52.7 ± 6.4 at the 2-year follow-up (P < .0001) (Figure 6). The VR-12 mental score was 51.6 ± 13.4 preoperatively, and this increased to 55.8 ± 5.3 at the 2-year follow-up; however, this difference was not significant (P = .07). No significant differences were seen between the 1- and 2-year postoperative time intervals.

Chart demonstrating the Veterans RAND 12-Item Health Survey (VR-12) physical scores at the different time intervals. The median, interquartile range, and range are illustrated in the box plot.
The Marx activity scale decreased significantly from 13.3 ± 3.9 preinjury to 10.6 ± 5.0 at the 2-year follow-up (P = .01). There was no significant change in the scores between 1 and 2 years postoperatively.
As outlined in Table 1, the majority of patients were happy with their combined ACL repair and ALL internal brace augmentation at 2 years. In total, 94% of the patients felt that the surgery exceeded or met their expectations with regard to reducing pain; 94% of the patients felt that the surgery exceeded or met their expectations with regard to improving movement and strength of the knee, as well as resuming normal functions of daily living; and 86% of the patients felt that the surgery exceeded or met their expectations with regard to resuming normal sporting activities.
Patient Satisfaction Scores at the 2-Year Follow-Up a
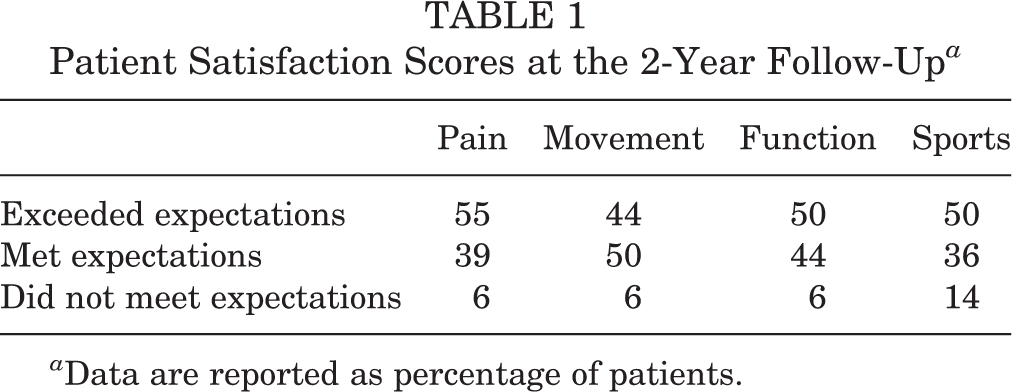
a Data are reported as percentage of patients.
Complications
Two patients (5.3%) sustained a rerupture after a significant trauma after returning to sport 9 months postoperatively. Both of these patients underwent a standard ACL reconstruction for their revision surgery and reported no issues at the time of this analysis. Moreover, no other complications or further surgery on the knee were reported at the time of this analysis. No significant differences were found between the 2 patients who sustained a rerupture (a 14-year-old boy and a 30-year-old man) and the other patients in terms of age, sex, or preoperative PROMs.
Discussion
This study demonstrates encouraging 2-year follow-up results of combined ACL repair and ALL internal brace augmentation. There were significant improvements in all aspects of the KOOS and WOMAC scores (P < .0001) as well as a significant reduction in the VAS for pain (P < .0001) and a significant increase in the VR-12 physical score (P < .0001). These 2-year follow-up PROMs are comparable with those of the Multicenter Orthopaedic Outcomes Network Knee Group of 1592 patients who underwent ACL reconstruction. 34 Two patients (5.3%) sustained a rerupture, and both of these occurred after significant trauma. The ACL survival rate of 94.7% is similar to the rates of other combined ACL/ALL reconstruction techniques that have recently been published. 26
Indeed, Helito et al 14 described better results in an ACL/ALL reconstruction group versus an isolated ACL reconstruction group in patients who were treated for a chronic ACL lesion. The ACL/ALL group had a positive pivot-shift test in 9.1% and no reruptures versus 35.3% and 7.3%, respectively, in the isolated ACL group at 2 years postsurgery. Additionally, Helito et al 15 described their findings in patients with ligamentous hyperlaxity and also demonstrated a lower failure rate with combined ACL/ALL reconstruction compared with ACL reconstruction alone (21.7% vs 7.3%). More recently, the STABILITY trial demonstrated a statistically significant reduction in graft rupture from 11% to 4% with the addition of a lateral extra-articular tenodesis to a single-bundle hamstring autograft ACL reconstruction. 12 Good clinical outcomes have also been revealed with combined autograft procedures in high risk-groups including professional athletes, and they have also been shown to protect medial meniscal repairs with a significantly lower rate of failure when compared with isolated ACL reconstructions. 26,32,33 The literature reports rates similar to our rerupture rate of 5.3%. Conversely, these techniques have some issues, as demonstrated in a recent anatomic paper that reported that there is a 70% chance of tunnel convergence with a combined ACL reconstruction and lateral extra-articular tenodesis. 19 The technique we described prevents this complication, as small tunnels are used for the ACL repair and bone anchors are used for the percutaneous ALL internal brace augmentation.
ACL repair and ALL internal brace augmentation were indicated in 43 patients during the time frame of this study. As illustrated in Figure 1, this was 21% of the total number of cases and 118 patients (58%) were suitable overall for ACL repair in the cohort of 203 patients. van der List et al 35 identified patients who were suitable for primary ACL repair and noted that 44% of their large cohort of 361 patients had repairable ACL tears. Additionally, the same group identified patients who were suitable for primary ACL repair on magnetic resonance imaging and demonstrated that 16% of their patients had type 1 tears and 27% had type 2 tears that were suitable for ACL repair. 36 On the other hand, Achtnich et al 1 reported the incidence of proximal ACL tears to be only 10%. The experience of the senior author (G.M.M.) in primary repair and the number of tertiary referrals at the time of this study could account for our higher proportion of ACL repairs, although Grøntvedt et al 13 did report that 71% of their patients had proximal third tears amenable to repair.
There are several limitations associated with this study, including the lack of clinical testing and radiological assessment at 2 years. Furthermore, no comparisons can be made with ACL reconstruction procedures or isolated ACL repair procedures, as all of the patients within the inclusion criteria underwent this combined procedure. Clinical studies are necessary with larger patient numbers and longer follow-up with objective clinical measurements and imaging, and concurrent cohorts to allow comparisons to further assess the encouraging early results of this combined ACL and ALL internal brace augmentation technique.
Based on our experience with this cohort, in addition to our isolated ACL repair outcomes, we suggest that younger patients (<25 years old), patients with a high level of sporting activity (Marx activity >14), and those with a grade 3 pivot shift or associated Segond fracture should have an additional ALL procedure to provide rotational stability. We also suggest that patients requiring ACL reconstruction have internal bracing with suture tape augmentation, as this has recently been shown to be biomechanically superior in the literature. 3,30 Therefore, our suggested treatment algorithm for ACL ruptures based on our experience is outlined in Figure 7.

Flowchart demonstrating our recommended treatment for anterior cruciate ligament (ACL) ruptures with internal bracing. ALL, anterolateral ligament.
Conclusion
Combined ACL repair and ALL internal brace augmentation had excellent outcomes in 94.7% of our patients. Therefore, based on our experience with this cohort, we suggest that high-risk patients with an ACL rupture, including younger patients, patients with a high level of sporting activity, and those with a grade 3 pivot shift or associated Segond fracture, should have an additional ALL procedure to provide greater rotational stability.
Footnotes
Final revision submitted June 12, 2020; accepted July 2, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: G.M.M. is a consultant for and receives royalties from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Strathclyde (UEC19/24).