
Abstract
Background:
Surgeons used the minimal clinically important difference (MCID) to interrogate outcomes—using patient-reported outcomes—to determine whether a patient can achieve clinical benefit after orthopaedic surgery. However, it is proposed to be crucial to separate the idea of meeting a clinically established threshold of patient-reported outcome measures (PROMs), which could truly predict patient-reported satisfaction with that outcome.
Purpose:
To investigate the association between achieving MCID and patient-reported satisfaction after arthroscopic superior capsular reconstruction with fascia lata autografts for irreparable massive rotator cuff tears.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
A total of 62 patients with ≥2-year follow-up and receiving questionnaires were included. PROMs were collected pre- and postoperatively, including pain visual analog scale (VAS), American Shoulder and Elbow Surgeons (ASES), and Single Assessment Numeric Evaluation (SANE) scores. MCIDs were determined using the sensitivity- and specificity-based approaches. Patient-reported satisfaction was evaluated with the following question: “Are you satisfied with your superior capsular reconstruction surgery (yes/no)?” The association between achieving MCID and patient-reported satisfaction was evaluated.
Results:
All 3 scores had acceptable area under the curve values (>0.7) for MCID. The MCID values were 4.5, 14.5, and 25.0 for the VAS, ASES, and SANE scores, respectively. Patients achieving MCID for PROMs had significantly greater improvement levels in the other clinical outcome scores than their counterparts (P < .05), except for the VAS score that demonstrated no difference between patients achieving and not achieving the MCID for SANE score (P = .07). Achieving MCID for PROMs was associated with a significantly higher proportion of patients feeling satisfied with the outcomes than the group failing to achieve the MCID (all P < .05). However, the percentages of patients who failed to achieve MCID for pain VAS, ASES, and SANE scores reported satisfaction with their results at 63.3%, 54.5%, and 59.1%, respectively.
Conclusion:
Achieving MCID thresholds on the VAS, ASES, and SANE scores were predictive of patient-reported satisfaction after arthroscopic superior capsular reconstruction 2 years postoperatively. However, half of the patients who failed to achieve MCID were still satisfied, regardless of clinical outcome improvements. Surgeons may need to be careful when consulting patients about expected outcomes, and patients need to set reasonable expectations based on their preoperative condition.
Keywords
Arthroscopic superior capsular reconstruction (ASCR) has been reported to achieve patient satisfaction.2,55,63 Historically, Yeom etal 63 revealed that 79.5% of patients were satisfied with their pain relief and functional outcomes after ASCR using fascia lata autograft. Shin etal 55 indicated that 95.3% of patients were satisfied with the outcomes after ASCR using dermal allografts. Surgical or nonsurgical treatment selection is subjectively associated with the patient’s and surgeon’s perception of how symptoms evolve because objective guidelines for determining which patient could derive the greatest benefit from ASCR remain limited. 46 Orthopaedic studies have widely applied patient-reported outcome (PRO) measures (PROMs) for evaluating healthcare quality8,16,47 and surgical outcome values.23,34 Patients have been reported to reach significantly improved clinical outcomes after ASCR.30,31,63 However, statistical significance may not necessarily correlate with clinical relevance.24,28 Hence, the emphasis is shifting toward meeting the minimal clinically important difference (MCID), which represents a meaningful improvement for patients postoperatively.3,15,43
Recently, practical and patient-centered benchmarks have been developed to evaluate clinically significant outcomes postoperatively.57,61 MCID is the minimal amount of change required for a patient to feel “better,” which focuses on the concept of patient improvement. 58 It was theoretical for most studies, which investigated the association between achieving MCID and predicting patient-reported satisfaction.3,11,17 Surgeons used MCID to interrogate outcomes—using PROs—to determine whether a patient can achieve clinical benefit after orthopaedic surgery.14,32,40,63 Additionally, PROMs have been used to evaluate the value of healthcare by commercial payers 61 and have been used in the orthopaedic arthroplasty field. 35 Based on previous studies on the association between MCID achievement and patient-reported satisfaction,11,17,27,35 separating the idea of meeting a clinically established threshold of PROMs, which could truly predict patient-reported satisfaction about that outcome, is proposed to be crucial.
Patient satisfaction with outcomes after interventions is demonstrated to be complex and context-dependent. 19 Some factors have been reported to affect patient satisfaction, including patient expectations9,20,25,56 and preoperative PROMs.48,59,63 Nowadays, surgeons establish the MCID values after ASCR using dermal allografts 14 and fascia lata allografts, 63 hoping that patients achieve clinically meaningful outcomes if PROMs exceed MCID thresholds. Waterman 61 proposed that clinical success stratification using clinically significant outcomes is more important to substantiate healthcare cost allocation for ASCR. However, achieving the MCID, defined as the threshold for clinically relevant improvement, and satisfaction reported by patients about their outcomes, are not necessarily equivalent.
Therefore, knowledge about the relationship between achieving MCID and patient-reported clinical benefits after ASCR remains limited. Thus, this study aimed to investigate the association between achieving MCID and patient-reported satisfaction after ASCR. This study hypothesized that (1) patients achieving MCID thresholds are related to PROM improvements and greater satisfaction at ≥2 years after ASCR and that (2) a subset of patients who achieve MCID would not feel satisfied, whereas a subset failing to achieve MCID would feel satisfied after ASCR.
Methods
Study Design
This retrospective study was performed after obtaining approval from the institutional review board of Asan Medical Center. A total of 109 patients with irreparable massive rotator cuff tears underwent ASCR from June 2013 to September 2020 were retrospectively reviewed. Inclusion criteria were (1) diagnosis of an irreparable rotator cuff tear with greatest dimension of the tear of >5 cm, complete tear of ≥2 tendons, or medial retraction of Patte grade ≥3 on a preoperative magnetic resonance imaging (MRI) scan according to their medical record, 36 (2) irreparable rotator cuff tear under arthroscopy as being irreducible to its anatomic footprint, and (3) graft using a fascia lata autograft. Exclusion criteria were (1) glenohumeral joint arthritis according to Hamada classification, (2) irreparable subscapularis tendon tear, (3) history of ipsilateral rotator cuff surgery, and (4) failed to reach a 2-year follow-up (Figure 1).

Flow diagram. ASCR, arthroscopic superior capsular reconstruction; ASES, American Shoulder and Elbow Surgeons; IRCT, irreparable rotator cuff tear; pVAS, pain visual analog scale; SANE, Single Assessment Numeric Evaluation; SCB, substantial clinical benefit.
Surgical Technique
All surgeries were performed in the beach-chair position after general anesthesia. Rotator cuff tear irreparability was confirmed under arthroscopy, followed by tear size measurement. Subacromial decompression, biceps tenotomy, and tenodesis (if present) were performed before anchor insertion. The assisting surgeon (J.Y.P.) harvested and prepared the fascia lata from the ipsilateral thigh. No. 2-0 polyester suture (Ethicon) was used to suture the folded graft with running sutures. 6 The preliminary outcomes of an earlier technique by the operating surgeon (I.H.J.) 31 changed the technique that a mesh was fashioned between the folded graft, since October 2016. A graft ≥6 mm thick was obtained at the final graft preparation. Three all-soft anchors (1.7-mm SUTUREFIX Suture Anchor; Smith & Nephew) were inserted at the glenoid to fix the graft, and 2 polyetheretherketone-threaded anchors (4.5-mm HEALICOIL Suture Anchor; Smith & Nephew) were introduced at the medial row of the footprint to fix the lateral side of the graft. The remaining rotator cuff and subacromial bursa were sutured using the “over-the-top” technique. 29 Finally, 2 knotless anchors (4.5-mm FOOTPRINT Ultra; Smith & Nephew) were used to fix all sutures in the lateral row.
Postoperative Rehabilitation
After ASCR, a brace was used to fix the shoulder at an abduction angle of 30° for 6 weeks, and patients were instructed to do pendulum exercises. Patients were supervised and taught to perform rotator cuff muscle–strengthening exercises from 3 months postoperatively. 38
Data Collection
Patient demographics, including age, sex, body mass index, and diabetes mellitus, were collected. Functional outcomes were followed up using the American Shoulder and Elbow Surgeons (ASES) 49 and Single Assessment Numeric Evaluation (SANE) scores. 5 Pain was assessed using the pain visual analog scale (pVAS) score. 63 The acromiohumeral distance was measured on the preoperative standard anteroposterior plain radiograph. All patients underwent MRI with a 3-T machine (Ingenia; Philips Healthcare) preoperatively, then 3 and 12 months postoperatively. Preoperative MRIs were used to evaluate rotator cuff retraction and fatty infiltration following the Patte and Goutallier classifications, respectively. 38 The fatty infiltration was rated and reported as the global fatty infiltration index. 18 Postoperative 3- and 12-month MRIs were used to evaluate graft healing and integrity. Any sign of complete graft discontinuity on MRI was defined as graft failure.4,41 At the follow-up visit, patients were requested to evaluate their changes in symptoms and whether they felt satisfied (Table 1).
Questionnaire a
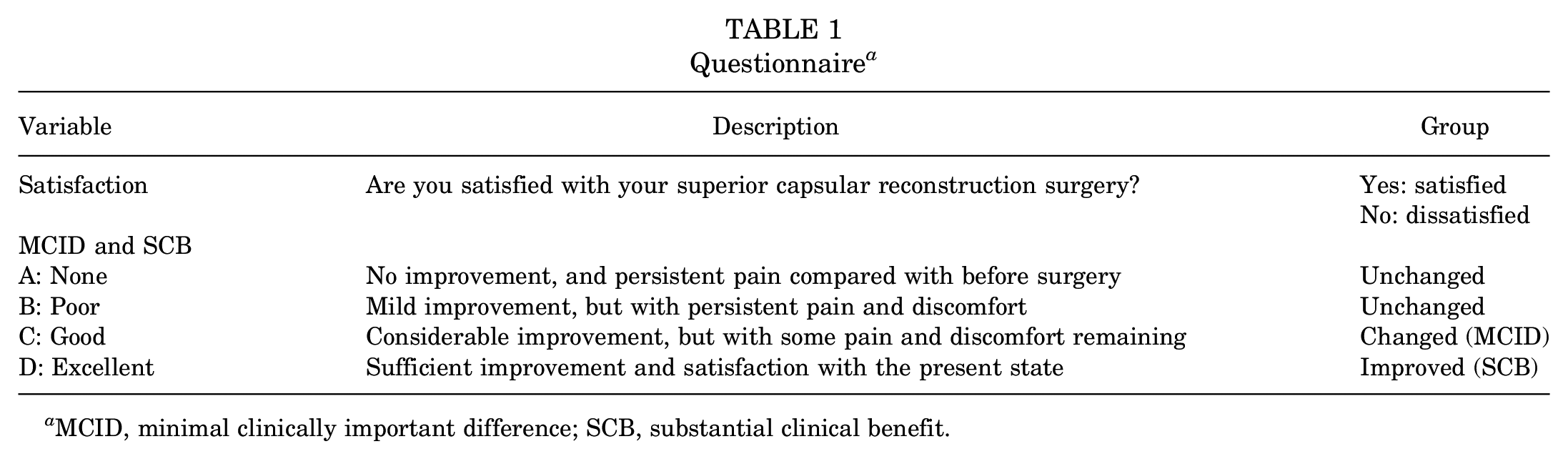
MCID, minimal clinically important difference; SCB, substantial clinical benefit.
MCID Determination and Questionnaire
MCID was determined using anchor-based methods. Patients were requested to express their postoperative state according to the questionnaire (Table 1), which included 4 response items: A (none), B (poor), C (good), and D (excellent). Patients’ answers reflected the changes in their symptoms. Patients who answered A or B were categorized into the unchanged group, those who answered D were placed into the substantial clinical benefit (SCB) (improved) group, and those who answered C were placed into the MCID (changed) group. Patient-reported satisfaction was evaluated with the following question: “Are you satisfied with your superior capsular reconstruction surgery?” [Yes/No].
Statistical Analysis
Reliability and predictivity for determining MCID and SCB were assessed using the receiver operating characteristic (ROC) curve and the area under the curve (AUC). AUCs of ≥0.7 and ≥0.8 were considered acceptable and excellent, respectively. 7 MCID and SCB were determined using sensitivity- and specificity-based approaches. The cutoff value of the ROC analysis between the unchanged and changed groups was derived as the MCID value. 63 The cutoff value of the ROC analysis between the unchanged and improved groups was derived as the SCB value. 63
Continuous data are presented as median ± SD. The results of data normality distribution indicated that an unpaired Student t test was used to compare the clinical outcomes, and a chi-square test was used to compare the graft integrity. Chi-square or Fisher exact test was applied to investigate whether those who achieved the MCID or maintained graft integrity had a higher chance of reporting satisfaction. The association between achieving MCID threshold and patient-reported satisfaction was evaluated and reported as sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), likelihood positive ratio, and likelihood negative ratio.
Results
Baseline Data
This study excluded 26 patients, including those who used allografts (n = 7), underwent revision surgery since those requiring additional surgery were thought to be less likely to report significant improvement and patient satisfaction (n = 9), and failed to reach a 2-year follow-up (n = 10). Additionally, as the purpose of this study was to investigate the relationship between patient satisfaction and MCID, it would overestimate the true relationship to include those achieving SCB, a further 21 patients were excluded. Thus, a total of 62 patients were included with a mean age of 64.5 ± 6.6 years and a mean follow-up time of 3.5 ± 1.4 years (Table 2). Patients had a mean body mass index of 26.1 ± 4.1 kg/m2 and a mean preoperative acromiohumeral distance of 5.0 ± 2.2 mm. Twenty (32.3%) patients demonstrated a subscapularis tear, of which 15 (24.2%) underwent repair and 5 (8.1%) did not because of an upper-part partial-thickness tear or tendinosis that did not require repair. No patients had subscapularis retear after repair. Nineteen patients (30.6%) developed graft tears after surgery. Satisfaction was reported by 48 (77.4%) patients, while dissatisfaction by 14 (22.5%) patients.
Demographics and Preoperative Findings (N = 62) a

Data are presented as mean ± SD or n (%) unless otherwise indicated. AHD, acromiohumeral distance; GFDI, global fatty degeneration index.
Determination of MCID Values
Table 3 shows the calculated threshold values with sensitivities and specificities. The established values of this cohort for pVAS, ASES, and SANE scores were 4.5, 14.5, and 25.0, respectively.
MCID Values for Each Score After ASCR a

ASCR, arthroscopic superior capsular reconstruction; ASES, American Shoulder and Elbow Surgeons; AUC, area under the curve; MCID, minimal clinically important difference; pVAS, pain visual analog scale; SANE, Single Assessment Numeric Evaluation.
Patients achieving MCID for VAS, ASES, and SANE scores had significantly greater improvement levels in the other clinical outcome scores than their counterparts (P < .05) (Table 4), except for the VAS score that demonstrated no difference between patients achieving and not achieving that for SANE (P = .07). Moreover, graft tears did not affect achieving MCID for all scores or for reaching satisfaction (Tables 4 and 5).
Association Between Achieving MCID Thresholds on PROMs and PROM Improvement a

Data are presented as mean ± SD or n. ASES, American Shoulder and Elbow Surgeons; MCID, minimal clinically important difference; PROM, patient-reported outcome measure; pVAS, pain visual analog scale; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale.
Association Between Achieving MCID Thresholds and Patient-Reported Satisfaction a

Data are presented as mean ± SD or n (%) unless otherwise indicated. ASES, American Shoulder and Elbow Surgeons; MCID, minimal clinically important difference; pVAS, pain visual analog scale; SANE, Single Assessment Numeric Evaluation.
Achieving MCIDs for VAS, ASES, and SANE scores was associated with a significantly higher proportion of patients reporting satisfaction than the group who failed to achieve that (P = .02) (Table 5). Furthermore, 63.3% (19/30) of patients who failed to achieve the MCID for VAS score felt satisfied after ASCR. Patients achieving MCID for ASES and SANE scores demonstrated similar results (P = .003 and .02, respectively). However, patients who failed to achieve MCID for ASES and SANE scores felt satisfied, accounting for 54.5% (12/22) and 59.1% (13/22), respectively.
MCID achievement demonstrated a sensitivity, specificity, PPV, and NPV of 0.604, 0.786, 0.906, and 0.367 for the VAS score; 0.750, 0.714, 0.900, and 0.455 for the ASES score; and 0.729, 0.643, 0.875, and 0.409 for the SANE score, respectively, for predicting patient-reported satisfaction (Table 6).
Association Between Achieving MCID Thresholds and Predicting Patient-Reported Satisfaction a

Data are presented as n (%) unless otherwise indicated. ASES, American Shoulder and Elbow Surgeons; MCID, minimal clinically important difference; NPV, negative predictive value; PPV, positive predictive value; pVAS, pain visual analog scale; SANE, Single Assessment Numeric Evaluation.
Discussion
The most important result is that achieving MCID thresholds on VAS, ASES, and SANE scores were predictive of patient-reported satisfaction after ASCR at 2 years postoperatively. Specifically, achieving MCID is associated with a high PPV for patient-reported satisfaction. Additionally, patients who achieved MCID demonstrated significantly higher improvements in clinical outcomes than those who failed to achieve MCID. However, another important result was that half of the patients reported satisfaction with the outcomes, although they failed to achieve MCID.
ASCR is thought to be the “experimental procedure,” and its value is discussed by surgeons and commercial payers. 61 However, ASCR is demonstrated to be reliable for successful pain management and function improvement.5,30,31 The study results revealed that patients who achieved MCID had significantly greater improvements in both pain and functional outcomes. Patients who suffered from low preoperative functions (either high VAS, low ASES or low SANE scores) appeared to be more likely to meet MCID. Additionally, achieving MCID was predictive of patient-reported satisfaction in the patient cohort after ASCR. However, the results indicated that patient-reported satisfaction after ASCR was not wholly determined by achieving MCID alone. Additionally, Aversano etal 1 revealed that a proportion of patients who failed to achieve MCID for the Boston Carpal Tunnel Questionnaire still reported satisfaction after carpal tunnel release. Further, Rogers etal 52 reported that a proportion of patients who failed to achieve MCID for the short version of the Disabilities of the Arm, Shoulder and Hand (68%) and Patient-Reported Outcomes Measurement Information System–Upper Extremity Computer Adaptive Test (77%) still expressed satisfaction after ligament reconstruction tendon interposition. This study revealed that a subset of patients who failed to achieve MCID for VAS (63.3%), ASES (54.5%), and SANE (59.1%) scores still expressed satisfaction after ASCR.
MCID is reported to be affected by many factors, including illness severity, patients’ concepts of health and improvement, and biopsychosocial status. 13 Further, a significant limitation of MCID is the possibility of a ceiling effect of achieving MCID in patients with high preoperative scores, even after achieving an excellent result. 12 Furthermore, previous studies revealed that patients with higher preoperative scores were more likely to fail to achieve the MCID postoperatively.44,50,54 Yeom etal 63 revealed that patients with higher preoperative scores had significantly lower odds ratios in achieving MCID after ASCR using fascia lata autografts. Evuarherhe etal 14 reported similar results using dermal allografts. Hence, MCID was proposed to not precisely measure patient-reported satisfaction for individual patients. In this study, surgical technique of graft preparation was changed from an isolated fascia lata to a fascia lata with a single layer of mesh inside. However, there was no selection bias for the application of mesh augmentation because the change started from the specific time-point (after October 2016), which was based on the evaluation of the preliminary surgical outcome using the earlier technique. Moreover, a previous study reported that mesh used was not a risk factor affecting the achievement of MCID and PASS. 63 Furthermore, no difference was found in graft tear rates between patients achieving MCID for all scores. This finding was also consistent with a previous study finding that graft tears did not affect MCID achievements. 63 However, the results of this study might not reveal the true effect of graft integrity on achieving MCID and patient-reported satisfaction. In this study, any sign of graft discontinuity on MRI, including graft tear with continuity and complete tear, was recorded as graft failure. Lee etal 39 reported that graft tear with continuity contributed significantly better outcomes than graft tear without continuity. This may explain why 12 patients (63.2%) of 19 patients with graft tear still reported satisfaction after surgery. Moreover, the recovery of range of motion and muscle strength may also affect the achievements of MCID and patient-reported satisfaction. Further studies using bigger sample sizes and detailed graft tear pattern are necessitated to investigate the effects of graft tears on achievements of MCID and patient-reported satisfaction.
Patient satisfaction is associated with many factors, including increased compliance, improved outcomes, 21 decreased risk of litigation, 26 patient understanding of one’s health, 21 and the meeting of preoperative expectations. 22 Decreased satisfaction is associated with poor patient health and slow recovery, as well as demographics.33,45,62 Acknowledging that patient satisfaction also varies between different procedures and diseases10,51,53 and is not always well understood by the treating surgeon.37,42,60 Moreover, patient-reported satisfaction is also affected by the relationship between doctors and patients. Patients might report satisfaction with less-than-ideal results to please a surgeon they like. Surgeons may need to be careful when consulting patients about the expected outcomes, and patients need to set reasonable expectations even with a poor condition preoperatively. The findings of this study enhanced the necessity of establishing more accurate and rigorous scales, which could predict the complex patient-reported satisfaction.
Limitations
This study demonstrated several limitations. First, this is a single-center study that may limit generalizability. Second, the enrollment rate of 57% could be a potential source of selection bias. However, the use of the 4 PRO questionnaires could separate patients who felt much improved (SCB) because it would overestimate the relationship between patient satisfaction and achieving MCID. Excluding those patients who achieved SCB was thought to contribute to more reliable and accurate results. Third, range of motion and muscle strength were not evaluated in this study, and the recovery of these objective measurements might affect satisfaction.
Conclusion
Achieving MCID thresholds on the VAS, ASES, and SANE scores were predictive of patient-reported satisfaction after ASCR at 2 years postoperatively. However, half of the patients who failed to achieve MCID still expressed satisfaction, regardless of clinical outcome improvements. Surgeons may need to be careful when consulting patients about the expected outcomes, and patients need to set reasonable expectations based on preoperative conditions.
Footnotes
Final revision submitted December 18, 2024; accepted January 21, 2025.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto. Ethical approval for this study was obtained from the institutional review board of Asan Medical Center (No. 2021-1321).