
Abstract
Background:
Limited options exist for young patients with massive, irreparable rotator cuff tears. While several treatment options exist, superior capsular reconstruction (SCR) was developed to restore glenohumeral joint stability by preventing superior humeral head migration during glenohumeral motion.
Indications:
Arthroscopic SCR is indicated in young patients with a massive, irreparable rotator cuff tear. Patients require a functioning deltoid muscle with minimal to no glenohumeral joint arthritis. In addition, patients should have Hamada grade 2 or less and should have an intact or repairable subscapularis tendon.
Technique Description:
The patient is positioned in the beach chair position. Standard anterior, posterior, and mid-lateral portals are established. An accessory posterior-superior lateral portal is used for visualization. Three 3.0 mm knotless anchors are placed in the glenoid through lateral percutaneous incisions. Two 4.75 mm anchors are placed adjacent to the humeral articular cartilage for medial row fixation. The graft dimensions are measured using the distance between the anchors. The graft is prepared using a gown card as a template with 5 mm added to the medial, posterior, and anterior graft dimensions, and 10 mm added to the lateral dimension. Sutures are passed through the graft in an inverted horizontal mattress for the glenoid anchors to diminish friction and allow appropriate suture passage through the knotless mechanism of the anchor. The graft is then shuttled into the joint through a lateral PassPort button cannula. Two lateral row anchors are used to secure the lateral graft on the humerus. Native rotator cuff tissue is repaired to the graft using sutures from the medial row anchors as well as free SutureTape.
Results:
Outcomes following SCR have demonstrated improvements in clinical outcomes and shoulder range of motion. Similar outcomes have been identified between the use of allograft and autograft. Patients generally are able to return to light recreational activities and work.
Discussion/Conclusion:
Arthroscopic SCR yields favorable results in the setting of a massive, irreparable rotator cuff tear. Meticulous surgical technique is needed to avoid intraoperative surgical complications.
The author(s) attests that consent has been obtained from any patient(s) appearing in this publication. If the individual may be identifiable, the author(s) has included a statement of release or other written form of approval from the patient(s) with this submission for publication.
This is a visual representation of the abstract.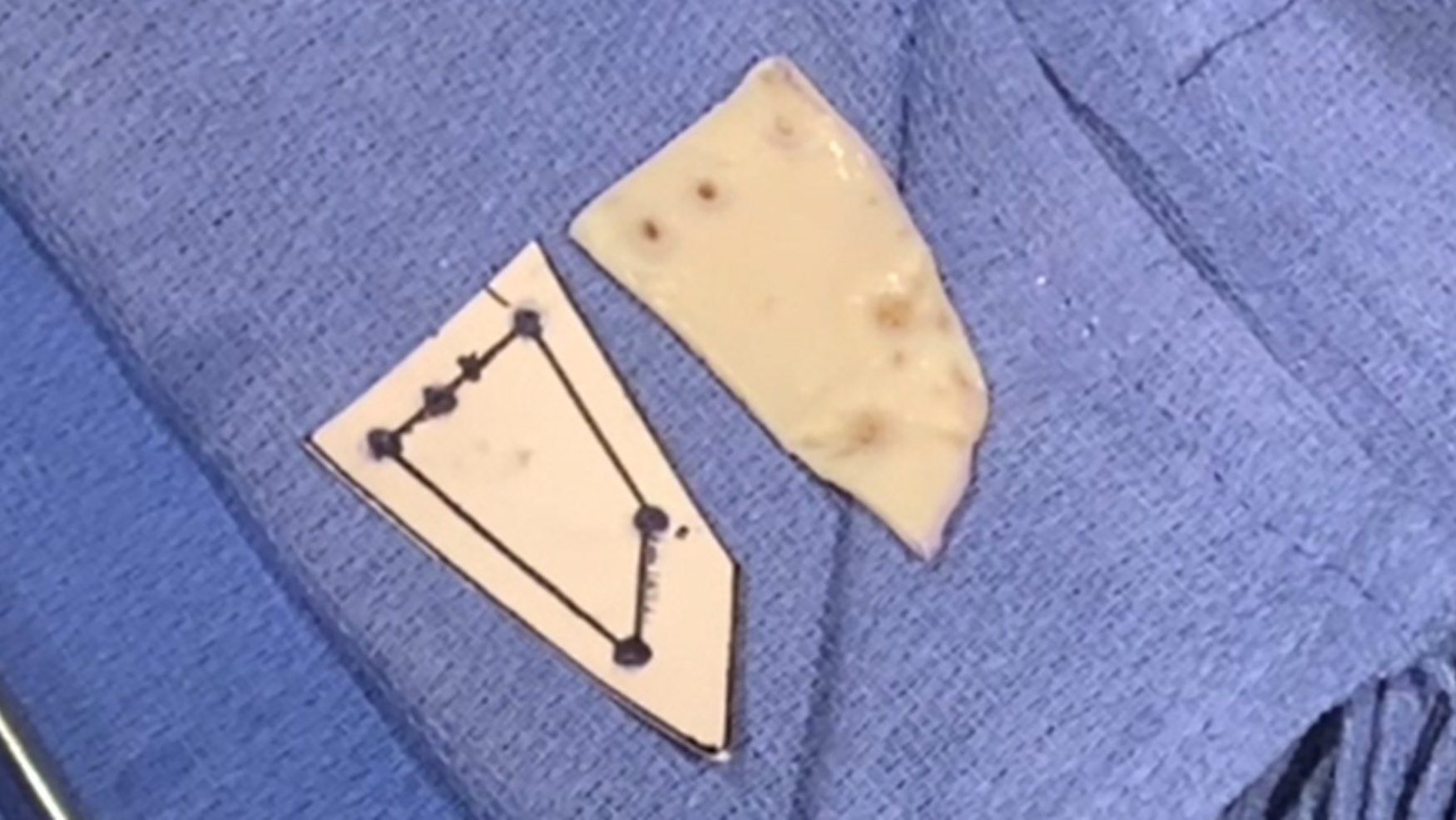
Video Transcript
This video describes our technique for arthroscopic superior capsular reconstruction.
These are our disclosures.
Here is an overview of the presentation.
Superior capsular reconstruction (SCR) was first introduced in 2012 as an alternative surgical treatment for irreparable rotator cuff tears. 7 SCR was developed to restore superior stability of the glenohumeral joint by creating a stable fulcrum for motion.
Biomechanical study has shown that with loss of the superior capsule, altered kinematics occur with increased glenohumeral translations in all directions. 8 With SCR, however, the superior stability of the glenohumeral joint can be restored.
For SCR to be successful, certain indications need to be met.2,6 The ideal candidate is an active patient with a massive, irreparable rotator cuff tear involving the supraspinatus and infraspinatus. Minimal glenohumeral joint arthritis and preservation of the acromiohumeral space are also needed. Also, a functional deltoid and trapezius muscle is needed, with optimal outcomes occurring with an intact or repairable subscapularis tendon.
Goals of the SCR are to prevent superior escape of the humerus during shoulder range of motion, minimizing acromiohumeral impingement, pain relief, and improved recruitment of the deltoid muscle once superior stability of the glenohumeral joint is restored.
Now on to the case. The case is a 50-year-old man with a history of right revision arthroscopic rotator cuff repair with patch augmentation by an outside provider. He presented to our clinic with a sudden onset of pain and weakness. Physical examination demonstrated active range of motion with forward flexion of 80°, external rotation of 50°, and internal rotation to L4. Strength testing revealed 4/5 strength with forward flexion and external rotation with a positive external lag and painful belly press and bear hug tests. Radiographs demonstrated preserved glenohumeral joint space with no arthritis as well as a preserved acromiohumeral distance.
Shoulder magnetic resonance imaging (MRI) demonstrated a retear of the posterosuperior rotator cuff involving the supraspinatus and infraspinatus. The tendons were retracted medially with stage-IV fatty infiltration. A repairable superior subscapularis tear was also identified.
Preoperative planning for SCR included beach chair positioning with an arm holder and a dermal allograft with a minimum of 3 mm of thickness. Arthroscopic portals included standard posterior, anterior, and mid-lateral portals. An accessory superior-posterior lateral portal was established for viewing, while percutaneous lateral portals were utilized for glenoid and medial row humeral anchor placement.
In addition to standard rotator cuff repair equipment, a mini lasso was available for shuttling of medial row humeral anchor suture through the dermal allograft. In addition, a PassPort Button (Arthrex; Naples, FL) cannula was used in the mid-lateral portal to pass the graft and for suture management. Glenoid fixation included three 3.0 mm knotless anchors, with 3.5 mm corkscrew anchors available for poor bone quality. Medial row humeral fixation included two 4.75 mm anchors loaded with fibertape, with lateral row humeral fixation including two 4.75 mm anchors. SutureTape (Arthrex) was used to repair the native cuff tissue to the dermal allograft.
Anticipated portals are shown.
The technique video begins having the subacromial space and bony beds already debrided and prepared.
Three 3.0 mm Knotless SutureTak (Arthrex) anchors are placed on the glenoid at 10, 12, and 2 o’clock. The anterior glenoid anchor is placed through the anterior cannula, while the remaining two anchors are placed through separate percutaneous incisions along the lateral acromion. The sutures remain exiting the shoulder in each of the respective percutaneous incisions until a later portion of the case.
Two 4.75 mm SwivelLock SpeedBridge (Arthrex) anchors are then placed at the anterior and posterior aspects of the greater tuberosity at the juxta-articular margin for graft medial row fixation.
The sutures from the 3 glenoid anchors and 2 medial row humerus anchors, with sutures directed downward toward the cannula, are now visualized.
The anterior dimension of the graft is determined using an arthroscopic measuring device, going from the anterior humeral anchor suture to anterior glenoid suture. The lateral dimension of the graft is determined going from the anterior humeral anchor to posterior humeral anchor. The measuring device is then used to measure the distance from the posterior glenoid anchor to both the middle and anterior glenoid anchors to determine the medial dimension of the graft. The posterior dimension of the graft is the distance from the posterior glenoid anchor to the posterior humeral anchor.
The graft is then prepared with the use of a template.
First, the measured dimensions are drawn out on a gown card. This includes 5 points: 3 glenoid anchors and 2 humeral anchors. The points are then connected using a straight edge to demarcate the lateral, anterior, medial, and posterior margins of the graft. Next, a 5 mm margin is added to the medial, anterior, and posterior borders of the graft. A 10 mm margin is added to the lateral border, which will assist in graft integration.
After the final template is drawn, a punch is used to place holes in the 5 anchor locations on the card. The template is then cut out using scissors.
The card template is then placed on the graft. The card template is outlined with a marking pen. The holes in the card representing the 5 points of the anchors are also marked. When the outline is complete, the graft is cut with a surgical knife while an assistant stabilizes the graft. The graft is then placed over a fenestrated instrument box, and holes are punched in the graft for the 2 humeral anchors. These holes will help facilitate suture passing. This completes preparation of the graft.
Returning to the arthroscope, a looped suture retriever is then used to deliver the sutures from the humeral anchors through the lateral portal, ensuring that one set is not wrapped around the other.
Meticulous suture management is crucial for the glenoid sutures. The glenoid SutureTak anchors have 3 suture limbs. The blue-and-white suture is fixed to the anchor. One of the 2 black-and-white suture limbs is looped, and the other is for passing. The blue-and-white and the looped black-and-white sutures from each glenoid anchor are retrieved through the lateral portal. The remaining nonlooped black-and-white limb is retained in each percutaneous incision. After each retrieval, the suture retriever is run along the previously retrieved set of sutures to ensure no tangles have been made.
The blue and white nonlooped suture limb is then passed through the medial graft with a Scorpion (Arthrex) in an inverted horizontal mattress fashion 10 mm apart to allow for suture sliding during graft delivery. The blue-and-white nonlooped suture that was placed through the graft is passed through the looped end of the black-and-white suture and shuttled through the knotless anchor. A small blunt instrument can be placed to assist with suture sliding.
This process is repeated for each glenoid anchor, resulting in 3 inverted mattress sutures through the graft with tails exiting each respective percutaneous glenoid incision.
A looped grasper can be utilized to ensure that there are no tangles by starting external to the cannula and heading toward each suture’s respective glenoid anchor.
A mini lasso is used to shuttle suture from the humerus medial row anchors through the graft.
A toothed grasper is used to roll the graft and push the graft into the joint through the lateral PassPort Button cannula. Once the graft is pushed beyond the cannula, gentle sequential traction on the ends of the suture exiting the percutaneous glenoid incisions is performed to prevent tangle. Full seating of the graft is confirmed visually and by feeling a hard stop on all 3 shuttling sutures.
The native cuff tissue demonstrated adequate mobility for later incorporation into the SCR graft.
Knotless fixation of the graft to the humerus is performed by placing two lateral row anchors, incorporating a limb of Fibertape from each humeral anchor. All excess suture are then cut.
The remaining native cuff tissue in this revision scenario is then incorporated into the SCR construct by passing the stay sutures from the medial humeral anchors through the native cuff tissue in horizontal mattress and tying arthroscopic knots to secure the native cuff to the SCR as well as the humeral footprint. Additional SutureTapes are passed posterior in a side-to-side fashion to secure the native cuff to the posterior graft.
Here is a view of the final construct. At the end, arthroscopic fluid is used to irrigate the subacromial space. The arthroscopic portals are closed and a shoulder sling is applied before the patient is awoken from anesthesia.
The postoperative protocol includes shoulder immobilization in a sling for 6 weeks. Elbow range of motion is started at 2 weeks. Passive range of motion with pendulum exercises is started around 6 to 8 weeks postoperatively. Active range of motion is then initiated at 8 to 10 weeks. Strengthening begins at 3 months after surgery. Patients can return to full activities around 5 to 6 months postoperatively.
There are several key points regarding arthroscopic SCR. With the technique described, the knotless glenoid anchor sutures are unable to be loosened after tightening. Therefore, suture management is critical to ensure no tangles are present. Running a looped instrument along the suture through the portal from external to the anchor, can help prevent tangles. In addition, a 1 cm suture bridge in the mattress suture of the graft will decrease friction and help prevent the sutures from being pulled through the knotless mechanism. Furthermore, slow and sequential tightening of sutures is recommended when bringing the graft to the glenoid. One additional key point is to template the graft size and anchor location separately from drawing on the graft, as this makes graft preparation more efficient.
With regard to returning to sporting activities, one study using fascia lata graft demonstrated a high rate of return to recreational sport and physical labor at a minimum of 24 months follow-up. 5
Multiple series evaluating the outcomes of superior capsule reconstruction have been published.1,3,4 With the use of SCR dermal allograft, preoperative measures improved at a minimum of 1 year for active forward flexion, visual analog scale (VAS) for pain, American Shoulder and Elbow Surgeons (ASES), and Subjective Shoulder Value (SSV) scores. The authors determined that 75% of cases were considered a success. 2
In a review of 10 articles of 374 shoulders, both allograft and autograft demonstrated improvements in clinical scores and forward elevation. The authors concluded that both allograft and autograft are acceptable options for SCR. 1
Thank you for your attention.
Footnotes
Submitted May 20, 2022; accepted September 16, 2022.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.