
Abstract
Background:
While anterior cruciate ligament (ACL) injury is often managed surgically in the young, active population, nonoperative management may be considered in older adults. Surgical decision-making in adults is usually based on patient preference, level of functional disability, and the presence of comorbidities. Understanding the role of clinical predictors in surgical decision-making can help identify disparities in treatment outcomes.
Purpose:
To report on clinical and social predictors of surgical versus nonsurgical treatment in patients with ACL injuries and quantify the influence of each factor.
Study Design:
Case control study; Level of evidence, 3.
Methods:
Patients diagnosed with ACL injury and those who underwent subsequent ACL reconstruction at a single center were identified. Functional disability was determined using patient-reported outcome measure scores, including the Knee injury and Osteoarthritis Outcome Score Physical Function Short Form (KOOS-PS) and Patient-Reported Outcomes Measurement Information Systems Physical Function (PROMIS-PF) within 90 days of diagnosis and before surgery. Clinical and sociodemographic factors were collected, and comorbidities were recorded using the Charlson Comorbidity Index. Logistic regression analysis was performed to identify relationships between clinical and sociodemographic factors with the likelihood of undergoing surgery for their ACL injury.
Results:
A total of 3656 patients were identified with ACL tear; 1734 (47.4%) were female (mean age, 34.9 years; SD, 13.8 years) and 1922 (52.6%) were male (mean age, 32.8 years; SD, 13.1 years). Overall, 53.8% of female patients and 53.4% of male patients underwent surgical treatment. Women had lower KOOS-PS and PROMIS values compared with men (−4.1 [P < .001] and −2.0 [P < .001], respectively) at the time of initial evaluation. Older age (P < .001), greater body mass index (P = .014), greater comorbidities (P < .001), smoking (P = .06), and subsidized insurance (P < .001) were negative predictors of surgery.
Conclusion:
Older age, greater body mass index, greater comorbidities, smoking, and subsidized insurance were negative predictors of undergoing surgical management of ACL injuries. Clinical predictors are useful in highlighting disparities and understanding ACL reconstruction decision-making for patients.
Anterior cruciate ligament (ACL) injury is one of the most common surgical sports injuries, with >250,000 reconstructions performed every year.4,25 Surgical management of ACL injury is commonly recommended in the young, active population to improve functional stability and preserve the long-term health of the knee. 24
In older adults, surgical indications tend to vary with patient preference, level of functional disability, and desire to return to sport.2,11,16,34 In these patients, ACL reconstruction (ACLR) is often recommended for patients with functional instability and a greater desire to return to cutting and pivoting sports or high activity demand. 40
Surgical decision-making after an ACL injury involves a thorough assessment of the risks and benefits of surgery, including clinical considerations and risk factors. Risk factors such as smoking, greater body mass index (BMI) and Charlson Comorbidity Index (CCI), 8 female sex, and low socioeconomic status have been associated with poorer outcomes and increased risk of post-ACLR complications such as venous thromboembolism, graft failure, worse anterior translation, and development of knee osteoarthritis.3,19,20,29,37,39 Socioeconomic status, including insurance status and education levels, has also been associated with poorer outcomes after surgery. 21 However, predictors of undergoing surgery beyond socioeconomic status in these groups have not been described.
Our study aimed to identify clinical and social predictors of surgical versus nonsurgical treatment in patients with ACL injuries and assess the relationship of findings with known clinical and social risk factors. We hypothesized that rates of surgical treatment would differ between groups based on social and clinical risk factors.
Methods
This study was approved by our institutional review board. Patients with a diagnosis of ACL injury at our institution from the start of the use of International Classification of Diseases, 10th Revision (ICD-10) codes in 2015 to 2022 were identified using ICD-10 codes S83.511 and S83.512, through a search of the electronic medical records. Patients who underwent ACLR of the ipsilateral knee subsequent to this injury were identified by Current Procedural Terminology code 29888. Patients were included in this study if they were diagnosed with an ACL injury of the right or left knee during an encounter in the sports medicine division at Massachusetts General Hospital. Exclusion criteria were those diagnosed with an ACL injury of an unspecified knee. Diagnoses or surgeries outside of the hospital or sports medicine division (eg, trauma or arthroplasty) were also excluded from this study.
All patients were divided into surgical and nonsurgical cohorts based on whether they underwent ACLR after receiving a diagnosis of ACL injury. Clinical and sociodemographic factors for each patient were recorded and are detailed in Figure 1. Patient comorbidities were recorded using the CCI, a weighted index that predicts the risk of death within 1 year of hospitalization with specific comorbid conditions. Smoking status was recorded as current use, previous use, or no use. Education level was recorded as less than high school, completed high school, some college, completed college, graduate school, or other. Insurance types were commercial, Medicare, and subsidized insurance, which included Medicaid and state-subsidized programs.

Collected clinical and sociodemographic patient characteristics. CCI, Charlson Comorbidity Index.
Functional disability for each patient was determined using preoperative patient-reported outcome measure (PROM) scores, including the Knee injury and Osteoarthritis Outcome Score Physical Function Short Form (KOOS-PS) and Patient-Reported Outcomes Measurement Information Systems Physical Function (PROMIS-PF) within 90 days of diagnosis and before surgery, if applicable. PROM scores from the initial visit were recorded when >1 set of scores was available.
Statistical Analysis
Descriptive statistics were used to summarize the number of patients with ACL injuries and the proportion of patients who underwent ACLR. Clinical and sociodemographic characteristics of all patients with ACL injuries were summarized with means and proportions, stratified by sex. Multivariable logistic regression was performed to determine predictors of surgery, with results presented as adjusted odds ratios and P values. In the subgroup of patients who reported PROM scores before surgery, an identical multivariable analysis was performed to determine whether the KOOS-PS or PROMIS-PF values were related to surgery. Secondary subgroup analyses were conducted for patients ≤30 and >30 years of age, based on previous data demonstrating a significant difference in patients undergoing surgery between these groups. 12 Finally, multivariable linear regression models with presurgical PROM scores as outcomes were run to examine whether function was different between women and men at the time of surgical determination and to identify other sociodemographic characteristics associated with physical function. Analyses were performed using SAS OnDemand for Academics (SAS Institute). Significance was set at a P value <.05.
Results
A total of 3656 patients were diagnosed with an ACL tear during an encounter with a surgeon in our sports medicine division (consisting of 15 surgeons), of whom 1734 (47.4%) were female and 1922 (52.6%) were male. The mean age of female patients was 34.9 years (SD, 13.8 years), and the mean age of male patients was 32.8 years (SD, 13.1 years). Overall, 78.9% of female patients were White and 21.1% were non-White, while 70.1% of male patients were White and 29.9% were non-White. The mean BMI was 25.2 (SD, 5.2) for female patients and 26.7 (SD, 4.3) for male patients. The CCI was 0.59 (SD, 1.3) for women and 0.40 (SD, 1.0) for men. Overall, 36.2% of female patients had some college or less as their highest level of education, whereas 46.4% of male patients had some college or less. Regarding insurance, 89.2% of women and 85.0% of men had commercial insurance. Full demographic information can be found in Table 1.
Characteristics of All Patients With ACL Tear Diagnosis (N = 3656) a
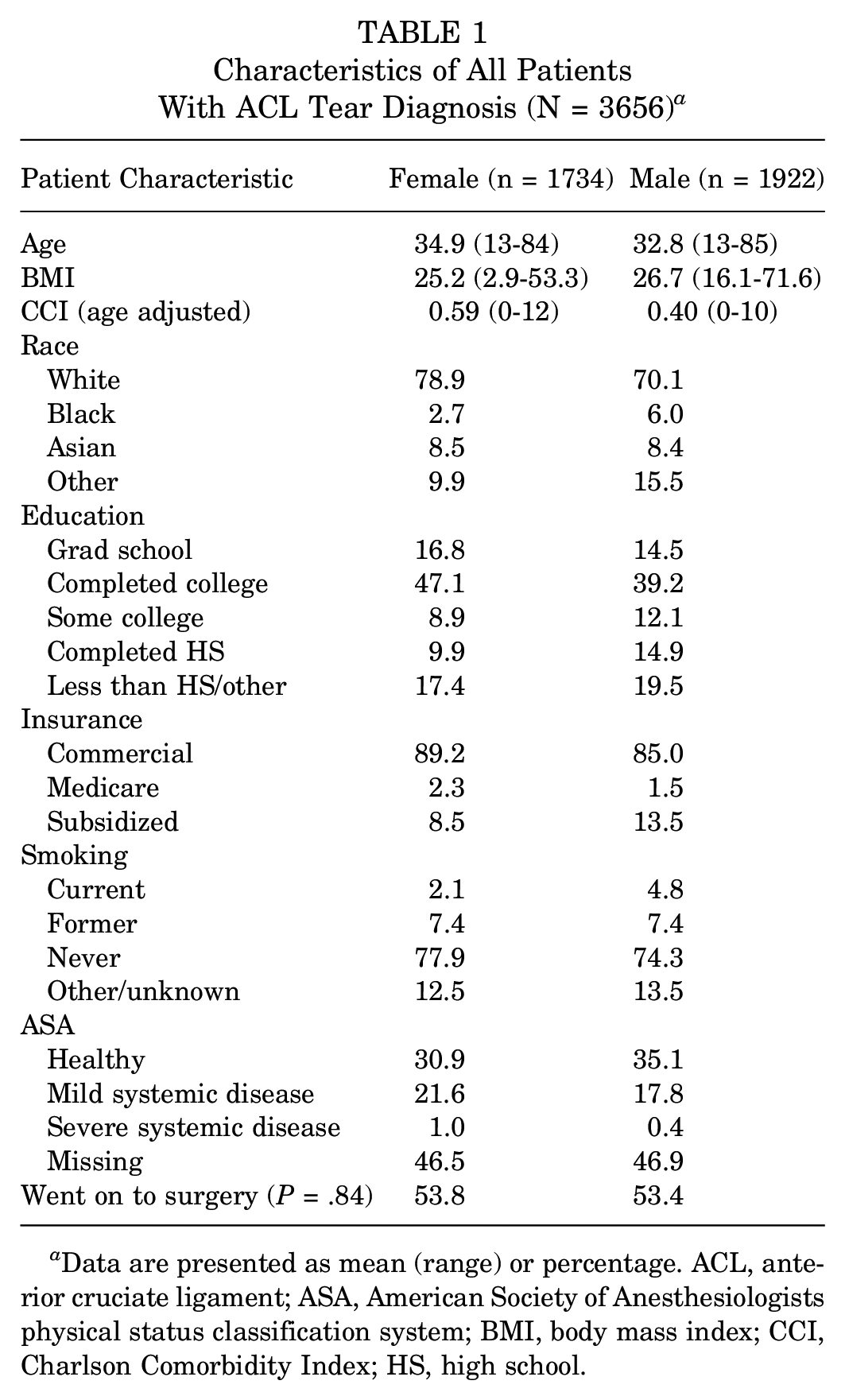
Data are presented as mean (range) or percentage. ACL, anterior cruciate ligament; ASA, American Society of Anesthesiologists physical status classification system; BMI, body mass index; CCI, Charlson Comorbidity Index; HS, high school.
Overall, 53.8% (n = 933) of female patients and 53.4% (n = 1027) of male patients went on to have ACLR surgery. All patients underwent surgery within 1 year of their diagnosis, with most undergoing surgery within 90 days. Only 15 (0.8%) patients underwent surgery >90 days from the time of their diagnosis. Odds ratios of factors associated with surgical treatment are shown in Table 2. Age (OR, 0.986; P < .001) and BMI (OR, 0.981; P = .014) demonstrated minimal effects, while CCI (OR, 0.867; P < .001), Medicare insurance (OR, 0.54; P = .04), and subsidized insurance status (OR, 0.47; P < .001) were significant negative predictors of surgical management, with current smoking status (OR, 0.70; P = .06) trending toward significance.
Predictors of Surgery for All Patients and by Age Cohort a

Bold P values indicate statistical significance. BMI, body mass index; CCI, Charlson Comorbidity Index; HS, high school; NA; not applicable; Ref, reference.
In patients ≤30 years, holding subsidized insurance was a negative predictor of surgical management (OR, 0.38; P < .001). In patients >30 years, a greater number of factors were found to influence rates of surgery, although the effects were minimal. In this group, women had a minimally greater likelihood of undergoing surgical management than men (OR, 1.05; P = .04). BMI was a slightly negative predictor of surgical management (OR, 0.97; P = .01), and factors such as CCI and smoking status trended toward significance.
In total, 998 (50.9%) patients had PROM scores available before surgery: 51.4% (n = 513) were women and 48.6% (n = 485) were men. The mean female age was 33.7 years (SD, 12.5 years), and the mean male age was 31.6 years (SD, 11.8 years). Women diagnosed with ACL injury had lower KOOS-PS and PROMIS-PF values at the time of evaluation when compared with men (−4.1 [P < .001] and −2.0 [P < .001], respectively). BMI was a negative predictor of KOOS-PS and PROMIS values for women (−0.59 [P < .001] and −0.22 [P < .001], respectively). Predictors of lower KOOS-PS were completing high school as the highest level of education (−7.67; P = .001) and current smoking status (−12.7; P < .001). For men, BMI (−0.33 [P = .01] and −0.16 [P = .01], respectively) and current smoking status (−10.4 [P < .001] and −3.54 [P = .01], respectively) were predictors of lower KOOS-PS and PROMIS values. Some college education (−2.46; P = .026) and completing high school as the highest level of education (−2.58; P = .01) were also predictors of lower PROMIS scores in men. Table 3 describes predictors of KOOS and PROMIS values in patients with ACL injury.
Predictors of KOOS and PROMIS Values in Patients With ACL Injury a

Bold P values indicate statistical significance. BMI, body mass index; CCI, Charlson Comorbidity Index; HS, high school; KOOS, Knee injury and Osteoarthritis Outcome Score; PROMIS, Patient-Reported Outcomes Measurement Information Systems; Ref, reference.
Discussion
The most important finding of this study was that surgical management of ACL injuries appears to vary by clinical and social factors. We found that greater age, BMI, and CCI; current smoking status, and Medicare or subsidized insurance type were predictors that negatively influenced the likelihood of undergoing ACLR after ACL injury.
Previous studies have reported on the rates of surgical intervention after ACL injury. In an analysis using a commercial insurer database, Cevallos et al 6 reported that the overall rate of ACLR in the population was 75%. While the overall rates of surgery in our study were substantially lower, we did find that insurance status was one of the main factors related to the decision to proceed with surgery. In our study, the presence of Medicare or subsidized insurance was associated with less than half the likelihood of proceeding with surgery than in patients with commercial insurance, suggesting that this could account for the difference in the rates seen between these studies.
Similarly, Otero et al 30 reported that when compared with privately insured patients, nonprivate insurance holders were less likely to go through with operative management due to disparities in access to care. Barriers to management of ACL injuries include cost of care, delayed time to diagnosis and treatment, and lack of physical therapy access. 37 When cost presents a barrier, patients may be more likely to pursue nonoperative treatments, as they have been shown to be more cost-effective than surgical management in middle-aged patients. 14 Patients insured with Medicaid have been shown to be seen in the clinic significantly later after initial injury and had worse outcomes compared with patients with other insurance types. 21 The study by Chava et al 9 reported that patients with Medicaid undergoing ACLR had lower postoperative patient outcome scores and were less likely overall to return to sport than their private insurance counterparts at final follow-up. Additionally, patients with nonprivate insurance attend significantly fewer postoperative physical therapy sessions than those with private insurance.26,31 Another aspect that may potentially contribute to this disparity was noted in a study by Hall et al, 17 that orthopaedic surgeons believe Medicare does not reimburse for ACLR well. While our study did not assess the reason for this disparity or its association with outcomes, further studies are needed to elucidate and address barriers to care in this population.
Increased age has been well established to negatively affect the likelihood of undergoing ACLR.13,35,38 Herzog et al 18 and Sanders et al 33 established that patients between 18 and 30 years had the greatest rates of ACLR compared with any other age cohort. The objectives of ACL injury management are to restore knee function, address psychological barriers to activity participation, prevent further injury and osteoarthritis, and optimize long-term quality of life, and these factors in decision-making differ between younger and older athletes. In younger athletes, especially <25 years of age, ACLR results in greater return to sport and reduces the likelihood of reinjury, development of arthritis, and meniscal injuries, 1 whereas rates of complications have been shown to be higher in patients >50 years, which may direct surgeons and patients away from ACLR and toward nonsurgical management. 32 In our study, while age was found to significantly influence odds ratios for surgery, the differences were clinically insignificant. Furthermore, while a greater number of risk factors were found to be significant in influencing surgery in the >30-year age group, the majority of these differences were not clinically significant.
Additional clinical factors such as BMI, smoking status, and comorbidities (CCI) are considered by orthopaedic surgeons when discussing surgical treatment options to optimize patient outcomes. Burns et al 5 found a positive correlation between increasing BMI in adult patients requiring revision ACLR. Ninkovic et al 27 conducted a systematic review with significant consensus that greater BMI is associated with poor patient-reported outcome metrics such as KOOS and decreased physical activity level after ACLR, increasing the risk of morbidity. Similarly, in our study, increased BMI was found to be negatively associated with undergoing ACLR; however, the reasons for this in terms of clinician or patient preference were not assessed. Further studies are needed to better understand how BMI is factored into the model of shared decision-making when discussing ACLR.
Smoking status is often considered a contraindication to elective surgery. 7 A systematic review by Novikov et al 29 found that cigarette smoking is associated with significantly worse clinical outcome scores and increased complication rates after ACLR. Smoking is recommended to be stopped 6 to 8 weeks preoperatively and up to 2 years after ACLR to minimize damage to graft ligamentization or graft rupture. 7 In our study, current smokers were less likely to undergo surgery than nonsmokers, and these findings trended toward significance, with the difference being most pronounced in the >30-year age group. Kraus et al 23 reported that active smokers had significantly worse baseline and postoperative PROMs compared with nonsmokers. Because of the significant risks associated with tobacco use in ACL injury, it is possible that surgeons recommend nonoperative management. Also, health behaviors, such as exercise, of smokers are not optimal, which may also factor in the patient’s preferences regarding surgical intervention. While this study did not assess the reasoning for nonsurgical treatment, future studies should explore the components of shared decision-making and factors that influence patients’ choices of treatment in ACL injury.
In our study, female sex, low education level, BMI, and current smoking history were found to be predictors of low KOOS-PS and PROMIS-PF values or low preoperative functional ability. Preoperative PROMIS, in a cohort study conducted by Chen et al, 10 was highly predictive of outcome in the early postoperative period in patients who underwent primary ACLR. Our findings are consistent with the current literature that establishes sex, education, BMI, and smoking status as predictors of worse outcomes.22,36 A cohort study performed by Nordenvall et al 28 found that patients classified as highly educated had a significantly increased likelihood of being treated operatively versus those with low education. DiSilvestro et al 15 pointed out that obese patients who underwent ACLR had lower KOOS values and a consistent association between overweight status and developing arthritis. Although the timing of presentation and diagnosis were not considered in relation to the patient-reported outcomes, our study highlights the differential in functional scores that exists between patient populations, and these require further study to optimize and promote parity in orthopaedic sports medicine care.
Limitations
This study has several limitations. First, our patient population comes from a single hospital and thus may not be generalizable to the entire US population. Additionally, our study does not account for surgeon counseling versus patient preference that may have influenced decision-making. This study was performed based on diagnosis and surgical procedure codes within the sports medicine division within 1 hospital and does not account for those who may have sought care outside of the hospital. Because the study is retrospective, there is potential for selection bias and confounding variables. Relevant clinical information impacting decision-making, such as concomitant injuries, physical therapy before surgery, and level of sports participation, was not recorded, limiting generalizability. Finally, this study was performed based on diagnoses and surgical codes and did not take into account patient-specific conditions or factors, including severity of injury and clinical symptoms, influence of physical therapy, presence of concurrent injury or multiligamentous injury that may have influenced surgical decision-making, or physical examination findings.
Conclusion
This study found that factors including increased age and BMI, the presence of comorbidities, smoking status, and nonprivate insurance status were negative predictors of undergoing surgical management of ACL injuries. While surgical decision-making involves careful consideration of the multitude of the risks and benefits of surgery, further study is needed to understand the reasons and potential barriers to care when optimizing treatments for populations with these risk factors.
Footnotes
Final revision submitted November 26, 2024; accepted January 3, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.J.T. has received consulting fees from Arthrex, Johnson & Johnson, Vericel, Verywell, DePuy Synthes Products, and Medical Device Business Services; and hospitality payments from Synthes GmbH and Pinnacle; her spouse has received consulting fees from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Mass General Brigham (protocol No. 2019P003181).