
Abstract
Background:
In young athletes with anterior cruciate ligament (ACL) injury, increased times from injury to magnetic resonance imaging (MRI) and injury to surgery can lead to the accrual of new injuries over time.
Purpose:
To determine the patient characteristics associated with differences in timing between injury, MRI, and surgery in young athletes with ACL tears.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
We reviewed the electronic medical records of patients aged 13 to 25 years who underwent isolated primary ACL reconstruction between January 2017 and June 2020 at a single orthopaedic surgery department. The times from injury to MRI, MRI to surgery, and injury to surgery were documented. Patient demographic data (age, sex, body mass index [BMI], race and ethnicity, and insurance type) were recorded. Multivariable analysis was used to determine if any patient characteristic had a significant association with increased time to MRI or surgery.
Results:
A total of 369 patients (mean age, 18.0 years; 56% female) were included. Both age and BMI were found to be significantly associated with timing of care while holding all other predictors constant. For every 1-year increase in patient age, time from injury to MRI increased by 9.6 days (95% CI, 1.8-17.4 days; P = .02), time from MRI to surgery increased by 7.4 days (95% CI, 4.4-10.5 days; P < .001), and time from injury to surgery increased by 17.0 days (95% CI, 8.4-25.6 days; P < .001). Compared with patients with normal BMI, overweight patients (BMI range, 25-29.9 kg/m2) had an MRI-to-surgery time that was on average 37.2 days (95% CI, 11.7-62.7 days; P < .004) longer and an injury to surgery time that was on average 71.8 days (95% CI, 0.5-143.0 days; P = .048) longer. Obese patients (BMI ≥30 kg/m2) did not demonstrate a significant relationship with the studied time intervals.
Conclusion:
Increasing age and elevated BMI were found to be associated with increased time to MRI and surgical care in young athletes with ACL injuries.
Keywords
Injuries to the anterior cruciate ligament (ACL) are among the most common knee injuries in the young athlete.11,14,23 For the majority of tears in this population, patients undergo ACL reconstruction to restore stability and return to sport. 14
Previous studies have shown that increased time from ACL injury to ACL reconstruction can lead to the accrual of new injuries over time, specifically medial meniscal tears.3,7-9,20-22,25 The complexity of the meniscal tears can also increase with delays to surgery.12,20 Untreated meniscal tears in the presence of ACL tears lead to poorer outcomes specifically in this patient population, with instability and progressive cartilage degeneration.1,7,8 In additional, the time between injury diagnosis with advanced imaging to surgical reconstruction can play a role in patient outcomes. While magnetic resonance imaging (MRI) has excellent sensitivity and specificity for diagnosing ACL and meniscal injury in the acute setting, its ability to accurately reflect injuries found intraoperatively decreases with increased time between imaging and surgery.4,10,15,19,21,22,24
Delays in care for young athletes who sustain ACL injuries, in receiving both advanced diagnostic imaging and surgical reconstruction, can have significant effects. However, risk factors for delays in care in this patient population remain largely undetermined. Previous studies outside of orthopaedic surgery have examined the causes for delay in care for both diagnosis and treatment. Race, marital status, and public insurance have been associated with delays in treatment for patients with adrenocortical carcinoma and breast cancer. 5 Within orthopaedics, public insurance and household income have been shown to be a barrier both to securing a clinic appointment and to receiving a diagnosis and treatment.2,6,13,16,18 A recent study examining individuals’ access to resources for health and development through use of the Child Opportunity Index, defined as a summative measure of indicators across education, health, and environment, with higher scores indicating greater access to resources, found that patients with higher scores who sustain ACL tears have surgery earlier than those with lower scores. 17
Identifying associations between risk factors and delays in care between ACL injury, MRI, and surgery would assist clinicians in developing strategies to improve care to this population. As prior investigations have examined the effect of patient characteristics on the development of subsequent meniscal injury after ACL injury, the purpose of this study was to determine the patient characteristics associated with differences in timing between injury, MRI, and surgery in young athletes with ACL tears. We hypothesized that patients with public insurance would be associated with longer times to MRI and surgery compared to those with private insurance in this population.
Methods
Patient Selection
The protocol for this study was approved by an institutional review board of the University of Washington. A retrospective chart review was performed on consecutive patients who underwent primary ACL reconstruction within a single academic orthopaedic surgery department between January 1, 2017, and June 30, 2020. Inclusion criteria were patients aged 13 to 25 years at time of surgery with demographic data available in the patient chart. Exclusion criteria were lack of active participation in an athletic activity, prior surgery to the ipsilateral knee, other ligament surgery at the time of ACL reconstruction, and charts without MRI, operative report, or date of initial injury. The age range was selected to include patients with the highest likelihood of participating in an athletic activity or sport at the time of ACL tear. Athletic activity was defined by participation in a primary sport as part of their recreational activities. This was done to include only our specific population of interest, as patients whose primary activities were of daily living and not sports likely had a difference in risk of future degenerative injury. All surgeries were performed by fellowship-trained orthopaedic surgeons specializing in sports medicine (M.H., A.G., C.K., K.C., M.S., G.S.). The patient selection process is illustrated in Figure 1. A waiver of documentation of consent was obtained.

Patient selection process through inclusion and exclusion criteria. ACL, anterior cruciate ligament.
Medical records were reviewed and demographic data were collected including age, sex, body mass index (BMI), race and ethnicity, and insurance status. BMI was categorized as underweight (<18.5 kg/m2), normal (18.5-24.9 kg/m2), overweight (25-29.9 kg/m2), and obese (≥30 kg/m2). Race and ethnicity were categorized as African American, American Indian or Alaska Native, Asian, White, Hispanic, Native Hawaiian or Pacific Islander, or other. Patients with multiracial ethnicity were given the option to choose 1 ethnicity or “other.” Insurance status was categorized as public, private, military, or self-pay. Date of injury was the day identified by patients on which they experienced an acute traumatic event that resulted in persistent knee pain, swelling, or instability. The following time intervals were then calculated: time from injury to MRI (TIM), time from MRI to surgery (TMS), and time from injury to surgery (TIS). Time of injury was defined as the date the patient experienced an acute instability event, a subjective popping in the knee, or leg trauma that resulted in persistent pain, swelling, or instability.
Statistical Analysis
The normality of data distribution was confirmed using Q-Q plots. We analyzed the effect of the study variables (age, sex, race and ethnicity, BMI, and insurance type) on TIM, TMS, and TIS through multiple linear regression models. Age was considered a quantitative variable, while the remainder were all categorical. For the categorical variables with more than 2 options, effects were compared with the value determined as having the highest proportion per subgroup (White race, normal BMI, and private insurance). Patients with “military” or “self-pay” insurance statuses were removed from analysis given their small proportion of the cohort. Factors of the raw categorical data were transformed into indicator variables for the sake of easier modeling.
We then determined the 95% CIs for factors that had significant effects on any of the time outcomes tested. An alpha value of .05 and a null hypothesis of 0 days were used to determine the significance of an effect on outcome. Type 2 errors for nonsignificant predictors were calculated as such. Confidence intervals were calculated using standard error values determined using N = 369 as the basis for degrees of freedom for t tests. Data were assumed to be normally distributed based on the nature of the data collected for analysis. When the combined effect of multiple factors was determined, the variances and covariances for the factors were used to determine the standard error of the effect. All calculations and modeling were done through R Version 4.2.1 (Posit PBC).
Results
Overall, 510 patients underwent primary ACL reconstruction during the study period. A total of 369 patients (56% female) were included with a mean age of 18.0 ± 3.4 years. The median TIM was 17 days (interquartile range [IQR], 0-39 days). The median TMS was 44 days (IQR, 22-66 days). The median TIS was 69 days (IQR, 25-113 days). Baseline categorical demographic data, stratified according to time intervals, are illustrated in Table 1.
Patient Characteristics According to Timing of MRI and Surgery (N = 369)

MRI, magnetic resonance imaging; TIM, time from injury to MRI; TIS, time from injury to surgery; TMS, time from MRI to surgery.
On multivariable analysis, age was found to be significantly associated with timing of care while holding all other predictors constant. For every 1-year increase in patient age, TIM increased by 9.6 days (95% CI, 1.8-17.4 days; P = .02), TMS increased by 7.4 days (95% CI, 4.4-10.5 days; P < .001), and TIS increased by 17.0 days (95% CI, 8.4-25.6 days; P < .001). The length of time to obtain imaging and surgery as a function of age is illustrated in Figure 2.
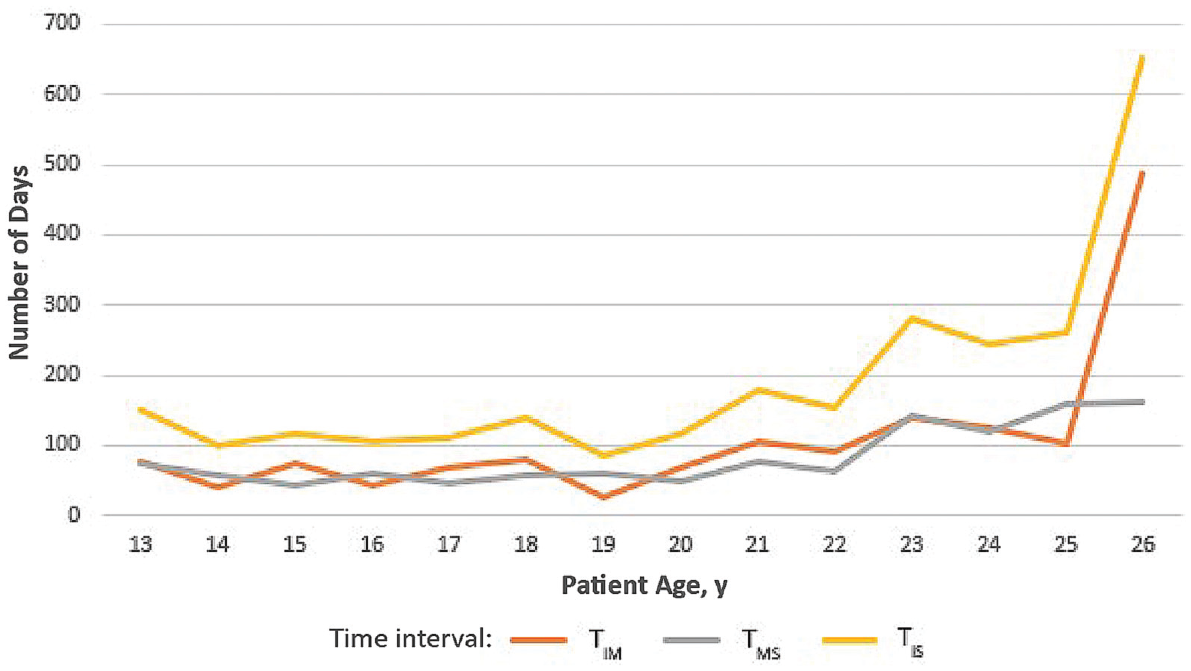
Timing of magnetic resonance imaging (MRI) and surgery as a function of patient age. There was a significant association between age and all 3 time intervals studied (P < .05 for all). TIM, time from injury to MRI; TIS, time from injury to surgery; TMS, time from MRI to surgery.
There was also a statistically significant association between BMI and timing of care while holding all other predictors constant. When compared to patients with normal BMI, TMS for overweight patients was on average 37.2 days (95% CI, 11.7 to 62.7 days; P < .004) longer and TIS was on average 71.8 days (95% CI, 0.5 to 143.0 days; P = .048) longer. Obese patients did not demonstrate significant findings with any time interval. For obese patients, TIM was on average 82.5 days (95% CI, –2.6 to 167.0 days; P = .057) longer than for those with normal BMI, and TIS was on average 86.2 days (95% CI,–8.8 to 181.0 days; P = .075) longer than for those with normal BMI. The length of time to obtain imaging and surgery as a function of BMI is illustrated in Figure 3. No other patient characteristics had a statistically significant relationship with the timing of care, although patients with public insurance or who were of certain minority races and ethnicities trended toward delays in care.
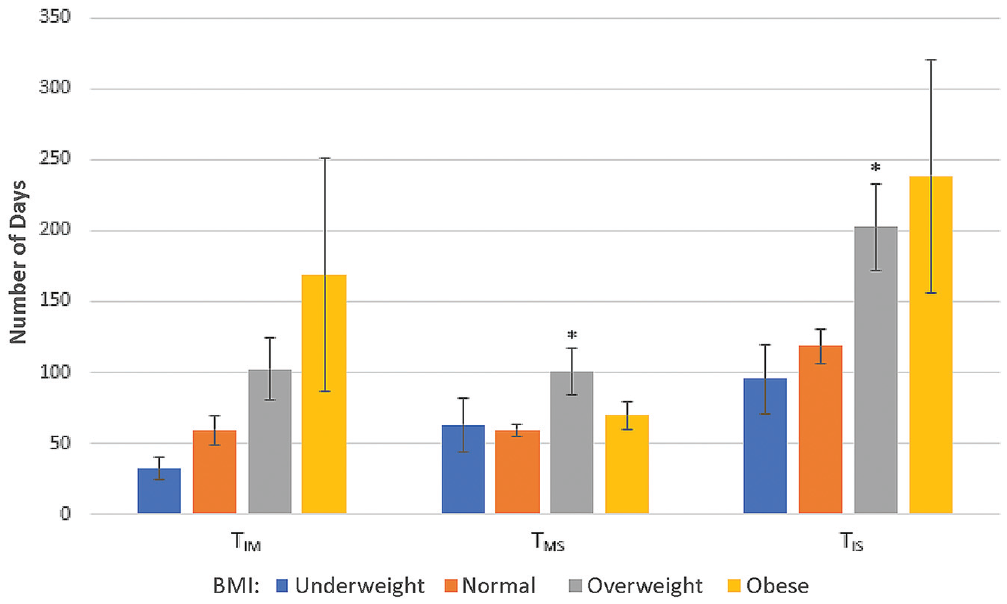
Timing of magnetic resonance imaging (MRI) and surgery as a function of patient body mass index (BMI). Overweight patients experienced significant delays from MRI to surgery and injury to surgery. Obese patients trended toward delays from injury to MRI and injury to surgery. TIM, time from injury to MRI; TIS, time from injury to surgery; TMS, time from MRI to surgery. Error bars represent 95% CIs. *Significantly different compared with normal BMI (P < .05).
Discussion
The results of this study indicated that increasing age and elevated BMI were associated with increased times from injury to MRI and surgery in athletes with ACL injuries, when controlling for other variables. Obese athletes also experienced a trend toward longer times to MRI and surgical care.
Previous studies have shown the importance of timely care in young athletes with ACL tears. Delays in diagnosis and surgical reconstruction can lead to the accrual of new injuries over time as well as diminishing value in diagnostic imaging.10,19,24 While the delays in these prior studies have mostly been over the course of years, rather than months as in our cohort, prior evidence has shown diminishing ability to repair concomitant meniscal tears with delays on a month-by-month basis. 20 With this knowledge, understanding what factors play a role in health care timing becomes all the more important.
No study to our knowledge has commented on the relationship that age and BMI have with the timing of health care in this patient population. Considering age, this may be due to surgeons’ prioritizing getting their younger patients to the operating room faster in order to minimize the amount of time spent on an unstable knee. In addition, older patients may have more rigid scheduling requirements that could preclude surgery being done right away, such as job requirements, college courses, or waiting for the off-season schedule in their sport. In our analysis, there were higher increases in each time interval after age 22 years, around the age of transitioning from undergraduate education to entering the work force. Younger patients may not have as many extrinsic constraints and could have more flexibility in the timing of MRI or surgery, allowing them to be seen earlier. Last, younger patients may also be more likely to live with their parents and have the help of family regarding transportation, rehabilitation, and general care, whereas older patients may be more independent and not have as much help at their disposal.
With regard to BMI, explanations for this association could include the makeup of patients with higher BMI. In athletes with an abundant soft tissue envelope, palpating bony landmarks and conducting accurate provocative tests can be more difficult than in thinner patients. In addition, BMI is an imperfect measurement of overall health as it factors in only height and weight. As a result, athletes can often fall into “overweight” or “obese” categories due to large stature and increased overall muscle mass. In those athletes with significant muscle mass, lack of appropriate relaxation can make physical examination maneuvers challenging. These challenges can lead to delays in diagnosis and, as a result, delays to imaging and surgery.
There is likely an element of hidden bias that providers have toward patients with higher BMI. Those with higher BMI could experience a lack of trust from their physician, disbelief in their symptoms, or even misattribution of their pain to other causes such as their weight. When this occurs, patients do not receive the timely care they deserve, leading to delays in ordering advanced imaging or even booking patients for surgery. This subset of patients is then exposed to consequences of ambulating with an unstable knee for extended periods of time. Furthermore, physicians may have their patients with elevated BMI wait longer times before surgical reconstruction in an effort to spend more time in physical therapy. This can be done to improve range of motion and mobility in order to maximize all other risk factors for surgical complications to ensure the best possible outcome postoperatively.
Existing studies have examined the role that patient characteristics play in health care timing, primarily insurance status. Hung et al 6 demonstrated that in patients with shoulder instability, public insurance was associated with delays in evaluation and postoperative complications. Pierce et al 16 conducted a survey study demonstrating reduced access to orthopaedic care in patients with acute ACL tears who had public insurance. In our study, sex, race and ethnicity, and insurance type did not produce a significant relationship with timing of care. A possible reason for the lack of statistical significance could be the makeup of each demographic factor. For example, almost two-thirds of our cohort identified as White, and there were over twice as many patients with private insurance as those with public insurance.
Strengths and Limitations
There are several strengths of this study. This includes our patient population size. We studied a large cohort of over 350 young athletes with ACL tears. In addition, we assessed multiple demographic factors at one time. We also examined multiple time intervals between injury, diagnosis, and treatment, all of which play a role in patient outcomes. Furthermore, the study brings to the forefront age and BMI, 2 demographic factors not often studied with regard to equality in care. Last, this study has the ability to change future practice. By recognizing these differences in care, we can then take the necessary steps to eliminate them. While the relationship between age and health care timing could be primarily due to extrinsic time constraints, equity in the timing of care should always be emphasized. With regard to BMI, we must become more aware of our own hidden biases. When seeing patients who have elevated BMI, we must consciously act to ensure they receive the same standard of care as other patients. Systemic changes can occur as well. For example, given the difficulty in examining a patient with higher BMI (either secondary to adipose tissue or high muscle content), there may be a false sense of stability that could delay a primary care provider's initiating the referral process to MRI or seeing an orthopaedic surgeon. Education of these challenges to referring physicians can help limit these delays. In addition, orthopaedic surgeons themselves can have a lower threshold for diagnostic imaging in patients who meet overweight or obese BMI criteria when examinations are more unreliable. System-wide protocols can be created that, for example, can lead to more efficient MRIs in this subset of patients. Finally, surgical delay due to increased time spent in preoperative physical therapy can occur implicitly or explicitly. Time between injury and surgery spent in therapy should be planned thoughtfully, and excess time should be avoided if added for reasons other than to promote the best outcome for the patient.
This study has limitations. First and foremost is the retrospective design. The study findings cannot determine a causative link between BMI and timing of care and can only provide associations. Second, there were patients who did not provide complete demographic data and as a result were not included in the overall analysis. The data set excluded 14% of patients secondary to incomplete demographic data, which could lead to over- or underestimating the disparities discussed. Third, the data collected were from a single orthopaedic institution, and thus the results may not be generalizable to other patient populations. Fourth, we did not record the date of initial evaluation. While valuable information, most patients in our hospital system with acute sports knee injuries are seen by a primary provider and referred to our service after MRI. As a result, we do not know if delays in TIM were secondary to time to initial provider evaluation versus referral to a specialist. Fifth, while we found significant results in patients with overweight BMI criteria, those with obese BMI criteria experienced delays that were not significant when controlling for other variables. It is possible that with 47 patients with BMI ≥30 kg/m2, our analysis of obese patients was underpowered, and including a larger sample size could lead to significant delays in the obese patient population. Sixth, we did not control for the intensity of sport played. While lack of participation in a sport was part of the exclusion criteria, sport activity level could be associated with BMI and therefore could confound the results related to timing of care in patients with elevated BMI. Seventh, we did not find a significant association with other demographic factors previously shown to be associated with timing of care, such as insurance type or race and ethnicity. Due to the small sample size for many nonsignificant factors, they uniformly had a high type 2 error. Incorporating a larger cohort, perhaps from several different populations, could have provided more statistical significance. Last, we removed patients who chose “military” and “self-pay” as insurance status from our analysis. This subgroup made up a fraction of our total cohort, as 96% of patients fell in either the “public” or the “private” insurance category.
Conclusion
Increasing age and elevated BMI were associated with increased times to MRI and surgical care in young athletes with ACL injuries. In the present study, we focused on a minority population that is less often discussed with regard to disparities in health care, expanding on the relationship between patients with higher BMI and increased time from injury to diagnosis and treatment. Recognizing and understanding this potential for disparities in health care are important to helping provide better patient care.
Footnotes
Final revision submitted August 28, 2023; accepted September 7, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.S. has received education payments from Summit Surgical and Arthrex and nonconsulting fees from Arthrex. G.S. has received education payments from Summit Surgical. A.G. has received education payments from Summit Surgical, Smith & Nephew, and Miach Orthopaedics and hospitality payments from Arthrex and Zimmer Biomet Holdings. C.K. has received education payments from Summit Surgical and Smith & Nephew and hospitality payments from Arthrex. K.C. has received education payments from Summit Surgical and Arthrex and hospitality payments from Stryker. M.H. has received education payments from Smith & Nephew, Summit Surgical, and Arthrex; consulting fees from Smith & Nephew and Linvatec; and hospitality payments from RTI Surgical and Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from University of Washington (ref No. STUDY00009903).