
Abstract
Background:
Rotator cuff repair aims to optimize stability and healing. While double-row (DR) techniques have shown biomechanical advantages, retear rates remain high, especially in the anterior supraspinatus (SSP). This region experiences greater gap formation and strain than the posterior SSP, making it more prone to retears.
Purpose:
To assess the biomechanical properties of a novel double–double-row (DDR) repair compared with a DR repair.
Hypothesis:
The DDR repair will exhibit superior biomechanical outcomes than the standard DR repair.
Study Design:
Controlled laboratory study.
Methods:
Twelve pairs of fresh-frozen human cadaveric shoulders were mounted to a 6-degree-of-freedom robot. With the humerus at 30° of abduction and external rotation, the SSP line of action was marked. The SSP muscle was dissected, and native tendon stiffness was measured. Each specimen was then repaired with either a DR or a DDR repair. The DR repair used a 6-strand, self-reinforcing construct with three medial and two lateral anchors. The DDR repair added an anterior row to the standard repair. A pressure sensor was placed beneath the repair. The tendon was then cyclically loaded from 25 to 100 N for 3000 cycles and pulled to failure. Repair footprint contacts and failure outcomes were compared.
Results:
The DDR repair group exhibited a 54% increase in overall contact area (DR, 172 ± 27 mm2; DDR, 266 ± 42 mm2; P < .001), a 92% increase in mean contact pressure (DR, 0.08 ± 0.03 MPa; DDR, 0.16 ± 0.4 MPa; P = .015), a 57% improvement in gapping (DR, 0.7 ± 0.2 mm; DDR, 0.4 ± 0.1 mm; P = .001), and a 57% increase in failure load (DR, 332 ± 119 N; DDR, 520 ± 184 N; P = .025) compared with the DR repair group.
Conclusion:
Addressing the anterior portion of the SSP in a DDR repair versus a DR rotator cuff repair yields significant increases in contact area and mean contact pressure at the tendon-bone interface, stronger fixation, and reduced gap formation under cyclic loading.
Clinical Relevance:
DDR repair may enhance healing potential and reduce retear risk, particularly in patients with anteriorly based tears or those at elevated risk due to tissue quality or tear morphology.
One of the central aims of rotator cuff repair has been to maximize mechanical stability and healing potential.7,27 Early open transosseous repair techniques were designed to achieve these goals by recreating the native tendon-to-bone footprint and providing broad contact for biological healing. As arthroscopic methods developed, the double-row (DR) technique was introduced as a minimally invasive adaptation of the transosseous approach, aiming to reproduce the mechanical strength and restore the footprint while leveraging the advantages of suture anchor technology.
While biomechanical studies have consistently shown that DR constructs provide greater footprint coverage, higher initial fixation strength, and improved load distribution compared with single-row techniques, clinical outcomes have been more variable. Despite these advantages seen after the adoption of DR repair, however, retear rates have ranged from 10% to 45% at long-term follow-up.10,22,25 Several randomized controlled trials and meta-analyses have reported no significant differences in functional outcomes, pain scores, or retear rates between single-row and DR repairs, particularly in small to medium-sized tears.4,15,31 These findings suggest that, although DR repairs may offer theoretical biomechanical advantages, their clinical superiority remains debated.
Further investigation into the causes of repair failure has revealed distinct anatomical and functional differences between the anterior and posterior regions of the supraspinatus (SSP).20,23,28,30 Additionally, biomechanical studies by Park et al 20 showed that gap formation in the anterior tendon region was significantly higher than the posterior tendon region with a suture bridge configuration. They also demonstrated that tendon loading during dynamic external rotation significantly increases strain and gap formation, specifically in the anterior SSP tendon.20,21 Previous studies have found that minimizing postoperative gap formation, minimizing cyclic micromotion, maximizing contact area of the repair site, and maximizing contact pressure of the repair site are critical to optimizing tendon healing.1,19,26 Studies examining retear patterns after rotator cuff repair have found that, with typical DR repairs, type 2 retears at the musculotendinous junction tend to be more common than type 1 tears due to lack of healing at the tendon interface. However, type 1 tears still occur, ranging from 25% to 40%, highlighting the importance of optimizing the strength of the repair at the tendon-bone interface.6,9,13 Thus, maximizing the primary fixation strength of the repair construct and matching the time-zero stiffness of the repair construct to the stiffness of the native tendon is thought to reduce the risk of repair failure in the immediate postoperative period. 2 These biomechanical insights underscore the importance of understanding the distinct anatomical and functional differences between the anterior and posterior regions of the intact SSP and inform the development of repair techniques that optimize healing across the entire repair footprint.
Traditionally, the DR configuration primarily addresses the central region of the SSP tendon, leaving the anterior portion uncovered and not fully repaired. However, the anterior region is where most rotator cuff tears initiate 10 and is prone to gapping during external rotation,20,21 which may increase the risk of retear postoperatively. Moreover, the involvement of the anterior SSP in full-thickness rotator cuff tears has been identified as a risk factor for retear after arthroscopic rotator cuff repair. 5 Given the propensity for failure in the anterior tendon region, enhanced fixation strategies targeting the anterior SSP may lead to improved outcomes and lower retear rates. This paper introduces a novel repair technique, termed the double–double-row (DDR) repair, that augments a standard DR SSP repair with an additional anterior DR configuration. It is unknown how this proposed repair technique biomechanically compares to the standard DDR repair.
This study aimed to assess the biomechanical properties of the DDR repair compared with a standard DR repair. We hypothesized that the DDR repair would exhibit greater footprint contact surface area and mean contact pressure, less gapping, and higher load-to-failure and stiffness than the standard DR repair.
Methods
Specimen Preparation
Twelve paired, fresh-frozen, human cadaveric shoulders (mean age, 54 years [range 35-64 years]; 3 male pairs and 3 female pairs) were included in this study. The cadaveric specimens used were donated to a tissue bank designated for medical research and purchased by the author’s institution. The use of cadaveric specimens donated for medical research is institutional review board exempt at the authors’ institution. Specimens were selected based on the following inclusion criteria: age 18 to 65 years; body mass index between 20 and 35 kg/m2; and no evidence or known history of degenerative joint disease, osteoarthritis, osteoporosis, cancer metastasizing to bone, or previous surgery to the shoulder. Specimens were excluded if there was gross evidence of rotator cuff pathology or greater tuberosity asymmetry—including footprint size, cysts, and bone quality.
Specimens were thawed at room temperature for 24 hours before dissection and testing. Skin and subcutaneous tissue were dissected except for the SSP, infraspinatus, and subscapularis. The glenohumeral joint was accessed arthroscopically through a posterior viewing portal and an anterosuperior portal established within the rotator interval. 3 The long head of the biceps tendon was tenotomized at the superior labrum. No open arthrotomy was performed, and the rotator interval was not excised. The biceps tendon was subsequently removed from the groove to simulate a miniopen subpectoral biceps tenodesis.
Biomechanical Testing—Establishment of Physiologic Muscle Line of Action
To test the fixation of a tendon repair site, the direction of pull must be in line with the physiologic line of action of the tendon. The orientation line of action of the SSP tendon changes with rotation of the humerus 29 ; thus, the physiologic line of action of the SSP tendon was determined when the shoulder was positioned in 30° of external rotation and 30° of abduction. This position may be commonly performed during rehabilitation, 20 and it allows the vulnerable anterior region of the repair site to be evaluated across repair types.
Before potting the specimens, a glenohumeral joint coordinate frame was established using a coordinate measuring machine (Romer Absolute Arm; Hexagon Manufacturing Intelligence) in accordance with the methodology established by SimVITRO (SimVITRO). To estimate the joint center, the humerus was rigidly clamped, and the scapula was allowed to rotate freely. The same point was digitized 20 times across different shoulder positions covering the entire range of motion of the joint, and a best-fit sphere was fitted to these points to determine the joint center, which was used as the origin of the joint coordinate frame. The lateral axis was defined along the line connecting the joint center with the trigonum scapulae. The anterior axis was defined as mutually perpendicular to the lateral axis and the axis passing through the joint center and a point collected on the inferior angle of the scapula. The superior axis was defined as mutually perpendicular to the anterior and lateral axes. After establishing the joint coordinate frame, the distal aspect of the humerus was potted in a cylindrical mold with polymethyl methacrylate (PMMA) (Fricke Dental).
The humerus was secured to a custom-designed fixture on the end effector of a 6-degrees-of-freedom robotic arm (KR 60-3; KUKA Robotics), equipped with a 6-axis universal force/torque sensor (ATI Industrial Automation). The scapula was rigidly fixed to another custom-designed fixture on a steel pedestal (Figure 1). To seat the humerus into the glenoid, a 50 N compressive force was applied to the specimen. The glenohumeral joint was then positioned to 30° of abduction and 30° of external rotation. A K-wire was drilled through the humerus in an orientation parallel to the line of action of the SSP muscle.

Six-degree-of-freedom robots used to establish the physiologic supraspinatus muscle line of action (left). Mechanical testing set up (right).
The specimen was then removed from the robot and disarticulated. The SSP muscle was sharply dissected 100 mm from the humeral origin. The humerus was cut to one-third of its proximal length and potted in a rectangular PMMA mold.
Biomechanical Testing—Native State
The native humerus with the K-wire installed was mounted to a dynamic tensile testing machine (Instron ElectroPuls E10000; Instron) with the humerus fixed to the end effector and the musculotendinous portion of the SSP fixed within a custom clamp fixed to the base of the testing machine 8 (Figure 1). To ensure that the line of action of the end effector was aligned to the line of action of the SSP, the humerus was positioned such that the line of action of the SSP tendon was parallel to the K-wire. The K-wire was then removed. Specimens were cyclically preconditioned over 20 cycles at 1 Hz from 5 to 20 N. A nominal 20 N of tension was then applied to the specimen to remove any slack in the muscle, and the position of the end effector was recorded. A constant nondestructive ramp displacement was then applied to the specimen at 0.5 mm/s up to 4 mm of displacement, and the resulting force-displacement curve was recorded. Native stiffness was calculated from the linear portion of this curve.
Study Design
This study employed a paired study design. In 6 randomly assigned shoulder specimens, a standard DR repair was performed. In 6 of the contralateral matched pairs, a DDR repair was performed. All surgeries were performed on the dynamic tensile testing machine under a nominal tensile load of 5 N.
Pressure Sensor Installation
A tear to the SSP tendon was replicated by sharply resecting the distal 10 mm of the SSP tendon from anterior to posterior. A flexible, thin electronic pressure sensor (K-scan Model 4000, 1500 psi; Tekscan Inc) was trimmed and placed at the repair site (see Figure 3) such that the anchors of the repair would be placed just outside the pressure sensor. The sensors measured pressures from 0.1 to 172 MPa with an accuracy of 0.1 MPa and a spatial resolution of 0.1 mm. The sensors were equilibrated and calibrated by performing the manufacturer’s defined calibrations at 20% and 80% of the expected maximum pressure. A power calibration was performed in accordance with the manufacturer’s specifications.
Surgical Technique
For the standard DR repair, a 6-strand self-reinforcing interconnected construct was created. Three medial-row anchors (2.6 Fibertak RC SP Soft anchors; Arthrex) were positioned at the far medial edge of the greater tuberosity footprint along the sulcus just lateral to the articular cartilage; the anterior-medial suture anchor was always placed 5 mm posterior to the bicipital groove. All-suture anchors were utilized because the senior author (M.T.P.) has recently started to utilize all-suture anchors to be able to more consistently place 3 medial row anchors with less risk of anchor convergence with larger anchors that are typically 4.75 mm in size. Two lateral holes were punched approximately 15 mm lateral from the medial row to remain as far lateral as possible on the footprint, thus maximizing the potential tendon contact area on the actual bony insertion. All holes were placed at a 90° angle relative to the footprint surface. For the medial and lateral rows, the distance between each suture anchor in the same row was 12.5 mm anterior to posterior, with approximately 25 mm between the anterior and posterior-most anchors, which corresponds to the mean width of the SSP tendon, 25 mm. 24 Two Peek knotless anchors (4.75-mm Swivelock; Arthrex) were used to establish the lateral row (Figure 2).

Schematic of the standard double-row repair (left) and the double–double-row repair (right).
For the DDR repair, a 10-strand self-reinforcing interconnected construct was created as previously described. 3 First, the technique for the 6-stranded standard DR repair anchors was performed as detailed above. Two additional flat-braided sutures (FiberTapes; Arthrex) were manually threaded through the eyelet of each medial anchor before anchor insertion and passed through the SSP tendon just anterior to the previously placed sutures. Another 4-strand self-reinforcing interconnected construct was created 10 mm from the medial row by anchoring these additional flat-braided sutures to an anterior row of 2 anchors (4.75-mm Peek knotless Swivelock; Arthrex) that were placed along the intertubercular groove (Figure 2). The senior author typically performs a mini open subpectoral biceps tenodesis; thus, the biceps tendon was not incorporated into the rotator cuff repair construct.
Biomechanical Testing Protocol
Six pins tipped with white or yellow spheres were placed in the specimen to track gapping of the repair site. A high-resolution digital camera was rigidly positioned so that the camera plane was perpendicular to the motion of the pins, and all pins were visible throughout testing (Figure 1). A nominal 20 N of tension was applied to the repaired specimen to remove any slack, and the initial position of the end effector was recorded. A 50 N load was then applied to the specimen, and the resulting force-displacement curve was recorded. Stiffness was calculated from the linear portion of this curve. A snapshot of the pressure map was captured from the pressure sensor under this 50 N load. The mean contact pressure and contact area were calculated from the pressure map. The repair was unloaded, and the pressure sensor was removed with care to avoid disturbing the repair site. A 1 Hz cyclic loading protocol was then applied to the specimen with loads cycling from 25 N to a maximum load of 100 N for 3000 cycles. The 100-N load was chosen for several reasons. The force of the rotator cuff has been estimated to be 9.6 times the weight of the upper extremity. If an average man weighs approximately 80 kg, and the SSP represents one-fourth of the maximum rotator cuff contraction, a 100-N load was deemed appropriate. 14 If repair had not failed after the 3000th period of cyclic loading, the specimen was then pulled to failure at a constant ramp displacement of 31 mm/min.
Statistical Analysis
A priori power analysis (G*Power 3.1 Universität Düsseldorf) based on the data from a previous study 20 indicated that a sample size of 7 pairs of specimens (Mean difference: 47.33, Standard deviation of difference: 37.39, Power: 0.8) is required to perform a paired t test.
Statistical analyses were performed using commercial software (MATLAB; Mathworks). Five outcomes are reported in this study: contact area of the repair site, mean contact pressure of the repair site, stiffnesses of the native and repair states, gapping of the repairs after cyclic loading, and failure load of the repairs. Shapiro-Wilk tests were used to assess the normality of the outcome data. Outcomes were compared between repair states using a 1 × 4 analysis of variance and a Tukey-Kramer post hoc test. Stiffness and footprint area were compared between each repair state and the native state using a 1-way analysis of variance and Tukey-Kramer post hoc test. Statistical significance was set at α = .05, with β error at 0.80.
Results
Contact Area and Pressure of the Repair Site
Representative contact pressure maps are presented in Figure 3, and a graphical display of contact area data and contact pressure data is presented in Figure 4. The DDR repair group exhibited a 54% significant increase in overall contact area (standard, 172 ± 27 mm2; double, 266 ± 42 mm2) and a 92% significant increase in mean contact pressure (standard, 0.08 ± 0.03 MPa; double, 0.16 ± 0.4 MPa) compared with the standard DR repair group. Regarding contact area and pressure of the anterior and posterior portions of the repair, the DDR repair yielded higher contact area (P < .001) and mean contact pressure (P < .001) in the anterior portion of the repair site compared with the standard DR repair. Posteriorly, contact pressure (P = .015) was higher in the DDR repair than the standard DR repair. Anterior and posterior contact area and mean pressure did not differ in DDR repair.

Representative specimens and their respective contact pressure maps of a standard double-row repair (left) and a double–double-row repair (right). Pressure values are reported in MPa.

Bar graph displaying contact area (left) and mean contact pressure (right) of the posterior and anterior sides of the standard double-row repair and the double–double-row repair. P < .05 was considered statistically significant and is indicated with an asterisk.
Stiffness
The graphical display of stiffness data is shown in Figure 5. Native stiffness of the standard DR repair group (23 ± 21.2 N/mm) was not significantly different than native stiffness of the DDR repair group (14 ± 9 N/mm; P = .617). The repair stiffness of the standard DR repair group (44.7 ± 7.1 N/mm) was not significantly different than that of the DDR repair group (57.1 ± 24.2 N/mm; P = .360). Stiffnesses of both repair groups were significantly higher than those of their respective native states (standard, P = .040; double, P < .001).
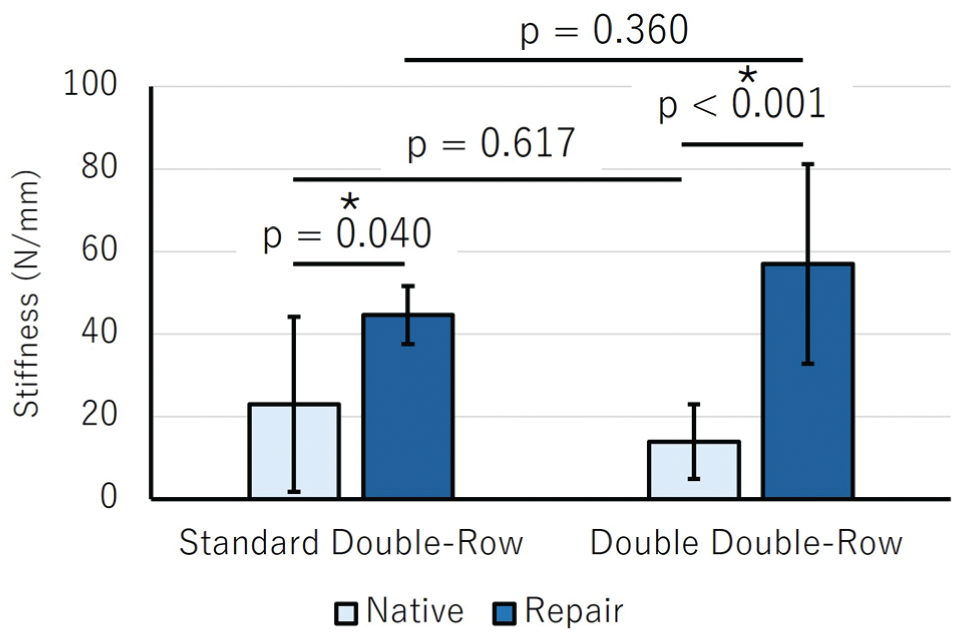
Stiffness values of native and repair states for the standard double-row repair (left) and the double– double-row repair (right). P < .05 was considered statistically significant and is indicated with an asterisk.
Gapping
The graphical display of the repair gapping data is shown in Figure 6. The DDR repair group exhibited a 57% significant reduction in gapping (standard, 0.7 ± 0.2 mm; double, 0.4 ± 0.1 mm; P = .001) compared with the standard DR repair group.

A bar graph displaying failure load (left) and a bar graph displaying repair gapping (right) of the standard double-row repair group and the double–double-row repair group. P < .05 was considered statistically significant and is indicated with an asterisk.
Failure Load
The graphical display of the failure load is shown in Figure 6. The DDR repair group exhibited a 57% significant increase in failure load (standard, 332 ± 119 N; double, 520 ± 184 N; P = 0.025) compared with the standard DR repair group.
Discussion
The results of this study demonstrate that augmenting a traditional DR rotator cuff repair with an additional anterior DR—termed the double–double-row repair—yields significant biomechanical advantages in the repair of the SSP tendon. Compared with the standard DR technique, the DDR configuration produced a marked increase in contact area and mean contact pressure at the tendon-bone interface, enhanced failure load, and reduced gap formation under cyclic loading. These findings support the hypothesis that targeted reinforcement of the anterior SSP improves the mechanical integrity of the repair construct.
Augmenting the SSP repair with additional anterior DR fixation yielded a 54% increase in contact area and a 92% increase in mean contact pressure compared with the traditional DR technique. The DR technique originally described by Millett et al 16 was designed to enhance contact area and compression of the repair site to improve healing potential. As is supported in previous research, greater footprint contact area and pressure are critical factors for tendon-bone healing, as they enhance biological integration and reduce interfacial micromotion that can disrupt early healing phases. 1 The addition of an anterior DR in the DDR technique not only increased surface area and mean contact pressure anteriorly but also, interestingly, significantly increased mean contact pressure on the posterior aspect of the repair. These results suggest that the DDR technique effectively added surface area anteriorly while reinforcing the entire repair footprint.
The enhanced anterior contact area and pressure in the DDR group specifically address the anterior SSP region—an area increasingly recognized for its susceptibility to strain concentration and retear, particularly in large or crescent-shaped tears. 21 Park et al 20 showed that the anterior rotator cuff is the first to experience peak tension during shoulder elevation, making it a biomechanically vulnerable zone. The observation that specifically reinforcing this region led to a 57% increase in failure load in our study suggests that anterior augmentation plays a critical role in optimizing load-sharing and construct strength. From a clinical standpoint, a stronger time-zero construct has important implications. The early postoperative period is when the repair is most dependent on mechanical stability, as tendon-to-bone healing is still biologically immature. Improved initial fixation strength may therefore reduce the risk of early repair failure, particularly when the humerus is externally rotated, and may allow for safer, more progressive rehabilitation protocols.
Gap formation has been identified as a biomechanical marker of repair stability and a predictor of poor tendon healing. In animal models, even small amounts of displacement at the repair site have been associated with impaired healing or retears. 11 In our study, the DDR configuration reduced gapping by 57% compared with the standard DR technique, reflecting a more stable construct capable of resisting displacement during early tendon healing. As Park et al20,21 demonstrated, the anterior SSP is prone to gapping, and the DDR appears to directly address this phenomenon by reinforcing the repair anteriorly, effectively reducing gap formation across the entire construct. This may be attributable to the anterior reinforcement provided by the additional row, which likely distributes force more evenly across the repair site and mitigates micromotion, particularly in the high-tension anterior zone.
Both repair techniques exhibited significantly greater stiffness than the native tendon, with the DDR repair demonstrating greater stiffness than the standard DR technique, although this difference was not statistically significant. The increased stiffness of both repair techniques over the native tendon is expected, as the overall stiffness is a combination of the individual pullout stiffness of the suture and anchors, as well as the inherent stiffness of the sutures and anchors, which are stiffer than the native tendon. A biomechanical study by Kim et al 12 that compared single-row and DR rotator cuff repair techniques found that the DR construct increased stiffness by 46% over the single-row repair. They postulated that this increase in stiffness was due to the medial row anchors serving as additional fixation points in sharing the load applied to the lateral sutures. In the present study, the increased stiffness exhibited by the DDR repair over the standard DR technique, albeit not statistically significant, aligns with this reasoning, as additional anterior suture anchors may help in sharing the applied load. However, since the DDR does not add any medial anchors, the addition of anterior anchors may have a smaller effect on the overall construct stiffness. Thus, the DDR technique maintains a stiff repair over the native tendon, similar to the standard DR repair, without creating an overly stiff construct that could be detrimental to healing. 17 It is important, nevertheless, to recognize that individual anatomic variation plays a critical role in the treatment of every rotator cuff tear. In smaller patients who may have reduced surface area for anchor placement, 18 a traditional DR construct may work well, and there may not be room for an additional anterior row even if the anterior SSP is involved.
The results of this study suggest that targeted anterior augmentation may address a critical shortcoming of the current gold-standard DR technique—namely, its limited engagement of the anterior SSP footprint. Given the biomechanical advantages observed, the DDR construct may provide a promising strategy to enhance healing potential and reduce retear risk, particularly in patients with anteriorly-based tears or those at elevated risk due to tissue quality or tear morphology.
This study is not without limitations. The use of cadaveric specimens, while necessary for controlled biomechanical testing, precludes evaluation of biological healing responses and does not capture the dynamic and variable in vivo loading environment of the shoulder. While efforts were made to simulate physiologic loading conditions, the application of uniform cyclic loads may not fully replicate the multidirectional stresses experienced during postoperative rehabilitation. Furthermore, although supported by a previous power analysis, the sample size was relatively small. Future in vivo studies with imaging and histologic correlation, particularly in patients with anterior SSP involvement, are needed to validate the clinical applicability of these biomechanical findings. Additionally, as the biceps tendon was tenotomized and limited rotator interval debridement was performed to permit anchor placement, these findings may not fully apply to cases where the biceps is preserved. In such cases, suture proximity to the intact tendon could pose a risk of irritation. The cost-effectiveness of the DDR was beyond the scope of this study. Future clinical studies comparing retear rates are needed to determine the cost-effectiveness of this new repair construct based on its effect on retear rates and outcomes, and the cost of the additional 2 anchors, in addition to increased operative time.
Conclusion
Augmentation of a traditional DR rotator cuff repair with an additional anterior row yields significant increases in contact area and mean contact pressure at the tendon-bone interface, stronger fixation, and reduced gap formation under cyclic loading.
Footnotes
Final revision submitted October 20, 2025; accepted November 19, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.T.P. reports a relationship with Arthrex Inc (consulting or advisory roles, grant funding, and travel reimbursement); Arthrosurface (consulting or advisory); Anika Therapeutics Inc (consulting or advisory); JRF Ortho (consulting or advisory); the United States Department of Defense (funding grants); the National Institutes of Health (funding grants); the Arthroscopy Association of North America (board membership); the American Academy of Orthopaedic Surgeons (board membership); the American Orthopaedic Society for Sports Medicine (board membership); the American Shoulder and Elbow Surgeons (board membership); the San Diego Shoulder Institute (membership); and the Society of Military Orthopaedic Surgeons (board membership). The corresponding author serves as an Editorial Board Member for Arthroscopy. P.J.M. has received intellectual property royalties, consulting fees, and research support from Arthrex; research support from Ossur, Siemens, and Smith & Nephew; and publishing royalties and financial or material support from Springer; and holds stock or stock options in VuMedi.