
Abstract
Background:
Rotator cuff tears (RCTs) are a significant cause of shoulder pain and disability. In clinical practice, assessing a patient’s rotator cuff health status generally includes multiple questionnaire-based clinical scales. Optoelectronic motion capture systems, currently considered the gold standard, can be used to assess shoulder 3-dimensional (3D) kinematics quantitatively. Identifying new, hitherto unexplored relationships between kinematic parameters and clinical scores may help provide new insights into the management of patients with RCTs.
Purpose:
To investigate the correlations between the most common clinical scores for evaluating patients with RCT and objective kinematic measures retrieved by optoelectronic motion capture systems.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 102 patients with RCT were enrolled to evaluate correlations between clinical scores (eg, Shoulder Pain and Disability Index [SPADI] score and Oxford Shoulder Score [OSS]) and kinematic measurements (range of motion [ROM] and peaks) obtained using a 3D optoelectronic analysis system while performing 4 tasks. The relationship between these variables was evaluated using the Spearman correlation analysis.
Results:
The results revealed moderate to weak correlations between some kinematic variables and clinical scales, varying by the kinematic variable type, the task performed, and the specific clinical scale. A moderate correlation was found between the SPADI score and peaks during flexion (ρ = −0.485; P < .001) and abduction (ρ = −0.493; P < .001). Another moderate correlation was found between the OSS and ROM in flexion (ρ = −0.428; P < .001) and abduction (ρ = −0.415; P < .001); additionally, a moderate correlation was found between the OSS and peaks in flexion (ρ = −0.403; P < .001) and abduction (ρ = −0.407; P < .001). Other significant correlations were identified between kinematic measures and clinical outcomes, albeit of fair intensity, between visual analog scale score and ROM and peaks in flexion, abduction, and external rotation.
Conclusion:
This study emphasizes the necessity of a multidimensional approach to managing RCT, showing that only moderate correlations exist between some kinematic measurements and outcome scores, such as the SPADI score and OSS. Furthermore, measures like the American Shoulder and Elbow Surgeons and visual analog scale scores display even weaker, fair correlations. This discrepancy suggests the need for complementary tools to comprehensively evaluate a patient’s rotator cuff health status.
Keywords
Introducion
Rotator cuff tears (RCTs) are a major cause of shoulder pain and disability, impacting up to 39% of the general population.18,22 This prevalence notably increases with age, affecting nearly half of all adults >70 years.3,21,22,29 Validated functional assessments are crucial in diagnosing, planning treatment, and monitoring patients’ progress.13,20,21,23 In current clinical practices, these often involve questionnaires, which, despite being validated, might not capture subtle variations due to reliance on predetermined score levels.2,8 Furthermore, scoring systems suffer from inherent operator-dependent subjectivity that may result in a nonobjective representation of the patient’s shoulder function. 2
Currently, an objective assessment of movement performance is feasible because of notable developments in 3-dimensional (3D) motion capture technology, which have transformed the study of shoulder biomechanics. Notably, optoelectronic motion capture (OMC) systems, currently considered the gold standard, provide significant insights into joint movement and function. 2 Three-dimensional kinematic assessments not only aid in identifying deficits in individuals who are clinically considered to have recovered well but also capture qualitative, detailed information on movement performance, including compensation strategies. 30 These objective measures of patient motor capabilities are instrumental in monitoring patient progress, evaluating the effectiveness of various interventions, and tailoring approaches to align with individual patients’ trends in motor recovery.19,30
Three-dimensional kinematic assessments are increasingly used as motor outcome measures in addition to clinical scores. 11 Three-dimensional kinematic assessment may represent a valid tool for objectively evaluating the efficacy of rehabilitation and surgical treatment. 9 Although these techniques afford an objective assessment of shoulder kinematics, their utility in everyday clinical practice is limited. Indeed, OMC systems necessitate highly skilled operators, are time-consuming and costly, and require a laboratory setting. 16 Furthermore, OMC systems also have inherent limitations, such as issues related to marker occlusion or soft tissue artifacts, which could negatively affect the accuracy of the measurements. 6 Nonetheless, OMC systems remain the most reliable method for motion analysis today.
Given that selecting the ideal outcome measures for assessing shoulder pathology remains a complex issue,10,15 the correlation values between kinematic parameters and clinical scores emerge as particularly valuable. Identifying new hitherto unexplored correlation values may help to select an appropriate set of kinematic measures and clinical scales, thereby enhancing the evaluation of motor impairment recovery after therapy. 31 Some clinical scores also assess the patient’s mental health status 23 ; so assessing the correlation between clinical scores and kinematic variables can also allow quantification of how health and psychological status are related to objective functional abilities.
The exploration of correlations between kinematic parameters and clinical scores has been proposed in various studies focusing on the motor recovery of the upper limb in patients with neurological diseases. However, there is a paucity of similar investigations in the literature involving patients with RCT.2,9,12,15,25 For this reason, this work aimed to investigate the relationships between the most commonly used clinical scores for evaluating patients with RCT and objective kinematic measures retrieved by OMC systems. Our hypothesis was that there would be correlation between kinematic measurement and clinical score.
Methods
Patient Population
For this cross-sectional study, 102 patients (mean age, 61 ± 24 years; 52 male, 50 female) were consecutively recruited from the Department of Orthopedic and Traumatology at the Fondazione Policlinico Universitario Campus Bio-Medico between March 2022 and December 2023. The study was approved by a local ethics committee (protocol code: 15.1[21].21 OSS ComET UCBM), and informed consent was obtained from all participants before data collection.
Inclusion criteria included a full-thickness supraspinatus tendon tear as documented by magnetic resonance imaging, no previous surgical treatment to the affected shoulder, no history of shoulder instability, no radiographic signs of fracture of the glenoid fossa or the greater or lesser tuberosity, and age >18 years. Conversely, exclusion criteria included refusal or inability to provide informed consent, previous surgical treatment of the shoulder, and fractures or additional pathological conditions in the affected shoulder, such as long head of the biceps brachii pathology. Patients enrolled in the study were administered clinical score assessments, and a protocol was performed to assess shoulder kinematics before treatment (baseline). Before each trial, the patient’s sex, age, anthropometric data, limb dominance, pathological limb, and type of treatment were collected. It should be noted that no subacromial injections were performed. The Laboratory of Motion Analysis performed all experiments and data acquisition.
Data Collection
Shoulder kinematics were evaluated for each patient by using a Qualisys stereophotogrammetric system.
A total of 22 anatomic markers (diameter, 8 mm) were placed bilaterally by the same operator to track body segments of the thorax, upper arms, and forearms, following the International Society of Biomechanics recommendations (Figure 1).6,33 Moreover, clusters of markers were placed on the thorax and bilaterally on the upper arms, forearms, and scapulae (Figure 1).6,32
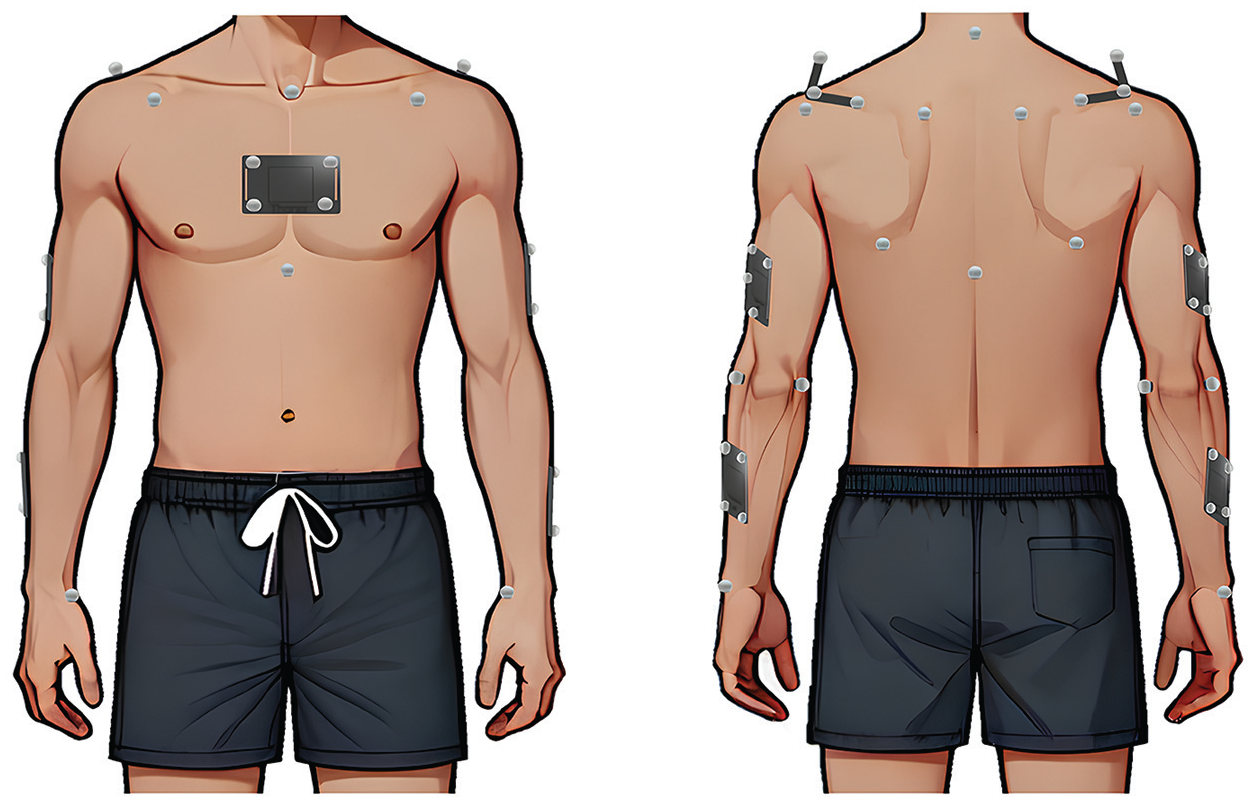
Placement of anatomic marker and clusters on the patient’s body.
For kinematic model implementation, patients were instructed to maintain a static pose with arms along the body and palms facing internally. Then, patients simultaneously performed bilateral upper limb movements: flexion-extension, abduction-adduction, external rotation with shoulder adducted and elbow flexed at 90°, and scaption, that is, elevations in the scapular plane (about 30° rotated anteriorly from the frontal plane). Patients performed the first 3 movements up to the maximum range they could achieve without pain and at a comfortable and self-selected speed. Similarly, patients performed elevations in the scapular plane up to a maximum of 120°, as tolerated based on their functional capacity and pain. Each movement was performed 5 times; however, only the central 3 repetitions were selected to mitigate potential undesired kinematics associated with adjustments at the beginning and at the end of the exercises.
Data Analysis
Patients’ OMC data were preprocessed using the Qualisys Track Manager software for marker trajectory labeling, gap filling, filtering (fourth-order Butterworth low-pass filter with a 6-Hz cutoff), 28 and event identification to isolate the repetitions of each movement. Subsequently, data were imported into Visual 3D (C-Motion) for model definition and shoulder kinematic analysis. All subsequent analyses were performed in MATLAB (Version R2023.a; MathWorks). A custom pipeline was developed to extract only the upward phases of the humerothoracic joint angles. The start of the upward phase of each repetition was determined by using the velocity profiles of the signals. 28 A custom algorithm was developed to detect a threshold set experimentally at 5% of the maximum absolute velocity. 28 The maximum value of the signal determined the end of the upward phase of each repetition.
Subsequently, quantitative parameters used as objective measures of shoulder functions were extrapolated, namely the range of motion (ROM) (computed as the minimum value subtracted from the maximum value) and maximum angles (peaks). 1
The mean and standard deviation or median and range of the ROM and peak values were determined for each task performed by each patient across the sessions.
Clinical Evaluation
Validated clinical score assessments were administered to all patients to evaluate shoulder function and pain. The clinical scales included the American Shoulder and Elbow Surgeons (ASES) Shoulder Evaluation Form 34 (range, 0-100), the visual analog scale (VAS) (range, 0-10), the Shoulder Pain and Disability Index (SPADI) (range, 0-100), the Oxford Shoulder Score (OSS) (range, 12-60), and the 36-Item Short-Form Health Survey (SF-36) (range, 0-100). 23
Statistical Analysis
All subsequent statistical analyses were conducted in MATLAB to assess the correlation between kinematic parameters and clinical scores. The normality of the data distribution was examined using the Shapiro-Wilk test. 24 The Spearman correlation test was performed to highlight any correlation between kinematic measurements and clinical scores at baseline, which was graded as excellent (0.81-1.00), good (0.61-0.80), moderate (0.41-0.60), fair (0.21-0.40), or poor (0.00-0.20).5,17 For all hypothesis tests, the P value for significance was .05 for rejecting the null hypothesis. Post hoc power analysis indicated that the power was 0.82 for the correlation between the SPADI score and ROM in abduction and 0.81 for the correlation between the OSS and ROM in flexion.
Results
All patients could perform the tasks, and ROM and peaks were successfully retrieved for all tasks executed.
Table 1 shows descriptive statistics (mean, standard deviation, median, and range) and the results of the Shapiro-Wilk test for the kinematic variables extracted for all the tasks. All variables, except ROM (P = .0923) and peaks (P = .0983) for shoulder abduction movement and ROM (P = .0819) and peaks (P = .0804) for shoulder external rotation in the transverse plane, were not distributed normally (P < .05).
Descriptive Statistics and Results of the Shapiro-Wilk Test for All Kinematic Variables Extracted for Tasks 1 Through 4 a

ROM, range of motion. Values are in degrees.
No normal distribution.
Table 2 shows descriptive statistics (mean, standard deviation, median, and range) and the results of the Shapiro-Wilk test for the clinical scores, that is, ASES score, VAS score, SF-36 score, OSS, and SPADI score. All clinical scores were not normally distributed (P < .05) except for the SF-36 score (P = .1352) and OSS (P = .1521).
Descriptive Statistics and Results of the Shapiro-Wilk Test for All Clinical Scores a
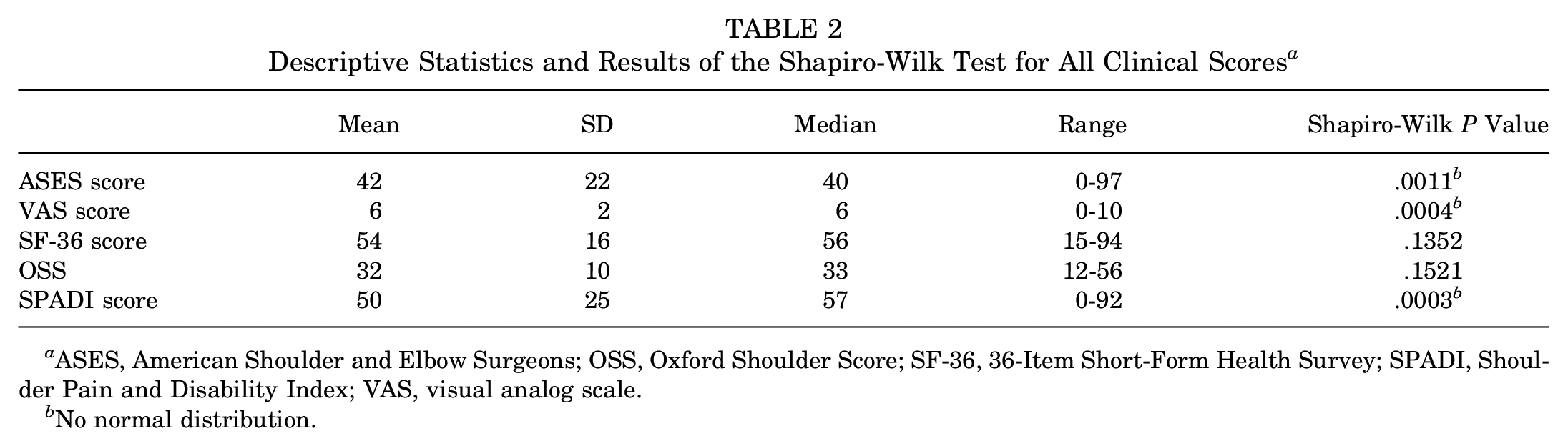
ASES, American Shoulder and Elbow Surgeons; OSS, Oxford Shoulder Score; SF-36, 36-Item Short-Form Health Survey; SPADI, Shoulder Pain and Disability Index; VAS, visual analog scale.
No normal distribution.
Correlation Analysis Between Clinical Scores and Kinematic Variables
The majority of the data exhibit a nonnormal distribution (P < .05) (Tables 1 and 2), so nonparametric tests were implemented for subsequent analyses. Figure 2 reports the results of the Spearman correlation test across all kinematic parameters and administered clinical scores.

Results of the Spearman correlation test between clinical scores and kinematic parameters. ASES, American Shoulder and Elbow Surgeons; OSS, Oxford Shoulder Score; ROM, range of motion; SF36, 36-Item Short-Form Health Survey; SPADI, Shoulder Pain and Disability Index; VAS, visual analog scale. *P < .05.
Moderate (0.41 < |ρ| < 0.60) and significant (P < .05) correlations were found between the SPADI score and ROM during flexion (ρ = −0.453; P < .001), scaption (ρ = −0.452; P < .001), and abduction (ρ = −0.543; P < .001) (Figure 3A).

Scatterplots (A) between the Shoulder Pain and Disability Index (SPADI) score and range of motion (ROM) and (B) between the SPADI score and peaks during abduction.
Moderate and significant correlations were found between the SPADI score and peaks during flexion (ρ = −0.485; P < .001) and abduction (ρ = −0.493; P < .001) (Figure 3B). Moderate and significant correlations were found between the OSS and ROM in flexion (ρ = −0.428; P < .001) (Figure 4A) and abduction (ρ = −0.415; P < .001); moreover, moderate and significant correlations were found between the OSS and peaks in flexion (ρ = −0.403; P < .001) and abduction (ρ = −0.407; P < .001) (Figure 4B). Additionally, other significant correlations were identified between kinematic measures and clinical outcomes, albeit of fair intensity (0.21 < |ρ| < 0.40) between the VAS score and ROM in flexion (ρ = −0.296), abduction (ρ = −0.338), and external rotation (ρ = −0.282) and peaks in flexion (ρ = −0.3226), abduction (ρ = −0.299), and external rotation (ρ = −0.285).

Scatterplots (A) between Oxford Shoulder Score (OSS) and range of motion (ROM) and (B) between OSS and peaks during flexion.
Discussion
In clinical practice, assessing a patient’s rotator cuff health status generally includes multiple questionnaire-based clinical scales, such as the ASES Shoulder Evaluation Form, VAS, SF-36, OSS, and SPADI. 23 Three-dimensional kinematic assessments are increasingly used as motor outcome measures. Identifying new, hitherto unexplored relationships between 3D kinematic parameters and clinical scores may help identify auxiliary tools that could objectively assess a patient’s rotator cuff health status. For this reason, the purpose of this work was to investigate the correlations between the results of different clinical scores used in patients with RCTs and objective kinematic parameters (ie, ROM and peaks) retrieved from objective assessments of shoulder motor performance through an OMC system.
Understanding the relationship between kinematic parameters and clinical scores may help clarify whether and how changes in mobility influence a patient’s perception of pain and function.
Our findings indicated moderate and weak correlations between some kinematic variables and clinical scales, which may depend on the type of kinematic variable considered, the task performed, and the specific clinical scale.7,15 Each clinical scale evaluates different aspects of shoulder function and patient well-being, with scores reflecting various facets of recovery.
The SPADI score and ROM showed moderate and significant correlations in scaption and abduction and a weakly significant correlation in external rotation. This suggests that as SPADI scores increase, indicating greater pain and disability, ROM decreases. In the study conducted by Anwer et al 4 involving a heterogeneous population of individuals with shoulder disorders (adhesive capsulitis, rotator cuff injury, impingement syndrome, acromioclavicular pain, and instability), similar good to weak correlations were reported between SPADI scores and ROM in abduction (ρ = −0.714), flexion (ρ = −0.547), and external rotation (ρ = −0.495).
Weak to moderate correlations were also observed between the OSS and ROM during flexion, abduction, and external rotation. Similar weak correlations between the OSS and ROM during flexion (ρ = −0.295; P < .001), abduction (ρ= −0.311; P < .001), and external rotation (ρ = −0.336; P < .001) have been reported in the literature. 27 These findings indicate that increases in pain levels and diminished functionality are associated with reduced ROM, suggesting a relationship between the OSS and shoulder kinematics, in accordance with findings by Özden et al. 27
Furthermore, weak to poor correlations were observed between VAS, ASES, and SF-36 scores and kinematic variables. ASES and SF-36 scores were found to be positively correlated with ROM and peaks. In particular, ASES scores showed a significantly weak correlation with ROM and peaks in abduction. SF-36 scores showed a significantly weak correlation with ROM and peaks in external rotation. These results show that lower ASES and SF-36 scores, indicating worse shoulder functional abilities and quality of life, correspond to similarly low values in ROM and peak joint angles. 14
A weak significant correlation was observed between ROM and VAS scores in flexion, abduction, and external rotation, which is in agreement with the findings of Özden et al, 27 who reported similar weak correlations, demonstrating that pain is only weakly associated with ROM.
Pain and daily activity limitations, as captured by scales such as the VAS and SPADI, are critical factors that significantly affect overall functional scores. 4 Thus, patients with limited ROM may nonetheless report higher clinical scores because of better pain management or increased capacity to carry out daily activities, which could account for a low correlation between kinematic variables and clinical scores.
Despite the potential discrepancies in how pain and disability are perceived versus objectively measured, clinical scores like the SPADI score and OSS still show a moderate correlation with ROM in key movements. This suggests that these scores do indeed capture significant aspects of the physical impairment caused by shoulder dysfunction, reinforcing their utility in assessing disability, providing important insights into both patient status and the effects of treatment.
Patient-reported outcomes and satisfaction levels are important elements of clinical evaluation; however, kinematic outcomes warrant equal emphasis for their essential role in objectively evaluating patient status, monitoring rehabilitation progress, and assessing surgical outcomes. While their complexity and the specialized expertise required may limit their routine use in clinical practice, these tools remain crucial in research settings, enabling comprehensive evaluations and driving innovation in patient treatment strategies.
Observed differences between the results of this work and previous studies in the literature could stem from several factors, such as different study populations, the intrinsic subjective nature of clinical scores, and the methodologies used for shoulder kinematic evaluations. For instance, Johnson et al, 14 who reported different correlations between ASES scores and ROM relative to our findings, used a goniometer for angle estimation, while in the current study, an OMC system was used for objective shoulder kinematic measurements. The difference in the methodology might account for the discrepancies between the results obtained compared with the literature, highlighting the effect of different assessment tools for shoulder kinematic evaluation and the subjectivity of clinical scores. 14 Furthermore, direct comparisons of the present study with other works in the literature regarding the correlation between clinical scores and peaks was not possible, as no previous study evaluated this kinematic variable.
In our study, an OMC system was used to evaluate shoulder kinematics with the aim of providing a comprehensive assessment. To increase the reliability of our results, all measurements were performed 3 times following a well-established protocol. Moreover, this study stands out as it comprehensively compares a wide range of scores for the first time and evaluates a large cohort of patients with rotator cuff issues using an OMC system.
Limitations
The results of this study must be considered in light of some limitations. First, correlations between clinical scores and kinematic parameters were assessed only at baseline before surgical treatment. Additionally, the study did not include control group, data differentiating between chronic and acute RCTs, or asymptomatic patients with RCTs.
Further investigations are needed to evaluate the relationship between clinical scores and shoulder kinematics at different time points with a larger sample size. This study considered ROM and peaks as kinematic parameters. In future works, other kinematic indices should be included to investigate their correlation with clinical scores, such as velocity, number of velocity peaks, spectral arc length, and peak velocity.15,30 Future research should also incorporate structural evaluation (eg, magnetic resonance imaging) 26 to identify how preoperative factors (such as tear size, muscle fatty infiltration, and muscle atrophy) may influence clinical outcomes.
Conclusion
This study emphasizes the importance of a multidimensional approach for RCT management, highlighting the complementary role of clinical scores and quantitative shoulder kinematic assessments. Despite the established utility of clinical scores in evaluating shoulder function and pain, the study identifies a discrepancy between these measures and shoulder kinematics evaluated with an OMC system, suggesting the need for complementary tools to comprehensively evaluate a patient’s rotator cuff health status. Biomechanical function assessments are crucial in clinical practice for disease diagnosis, medication prescription, and therapy modification. They are also used for management and to provide feedback to patients and clinicians. Finally, sensitive and reliable evaluations are essential for use as clinical trial outcome measures. Therefore, our data suggest that given their moderate and significant correlations with some kinematic measures, the SPADI score and OSS are the most likely to be included in future hybrid clinical biomechanical metrics.
Footnotes
Final revision submitted November 27, 2024; accepted December 30, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding was received from the European Union—Next Generation EU—NRRP M6C2—Investment 2.1 Enhancement and Strengthening of Biomedical Research in the NHS (Project No. PNRR-MAD-2022-12376080–CUP: F83C22002450001). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Fondazione Policlinico Universitario Campus Bio-Medico (2022.202).