
Abstract
Background:
Subscapularis (SSC) tears can present as isolated or combined with additional rotator cuff tendon tears. The repair of SSC tear improves postoperative outcomes. However, the effect that SSC repair and healing have on functional outcomes after arthroscopic repair of isolated or combined SSC tears requires further investigation.
Purpose:
To (1) compare the clinical outcomes of arthroscopic rotator cuff repair (ARCR) of isolated SSC tears with those having SSC tears combined with supraspinatus and/or infraspinatus tears and (2) evaluate the effect of SSC healing on postoperative clinical outcomes.
Study Design:
Cohort study; Level of evidence 3.
Methods:
A retrospective study was carried out in patients who underwent ARCR of isolated or combined SSC tears with a minimum 2-year follow-up. Three groups were compared: isolated SSC tear, anterosuperior rotator cuff tear with SSC tear (AS-RCT) and posterosuperior rotator cuff tear with SSC tear (PS-RCT). Patient-reported outcomes (PROs) and range of motion (ROM) were assessed pre- and postoperatively. SSC healing was evaluated via ultrasound at the final follow-up in a subset of patients.
Results:
The study included 588 patients with a minimum 2-year follow-up, of whom 279 underwent ultrasound assessments. PROs and ROM improved after ARCR in all groups (P < .01). The postoperative American Shoulder and Elbow Surgeons (ASES) score improvement was significantly higher for the AS-RCT group compared with the PS-RCT group (P = .01), with no statistically significant difference between isolated SSC and AS-RCT (P > .05), or between isolated SSC and PS-RCT groups (P > .05). There was no statistically significant difference when comparing the pre- to postoperative change in ROM between the groups (P > .05). The SSC healing rates for isolated SSC, AS-RCT, and PS-RCT groups were 88.1%, 91.6%, and 84.3%, respectively, (P >.24). There was no significant difference in ASES score or Subjective Shoulder Value (SSV) improvement between healed and unhealed groups in patients with isolated SSC tears (P > .05). ASES and SSV were significantly lower in unhealed SSC patients compared with those having a healed SSC in patients with AS-RCTs (ASES, P < .01; SSV, P < .01) and PS-RCTs (ASES, P > .01; SSV, P < .01).
Conclusion:
Both isolated and combined SSC repairs showed improvement in PROs and ROM. SSC healing rates did not differ between isolated and combined SSC tears. While failure to heal did not affect the clinical outcome of isolated SSC tears, an unhealed SSC was associated with lower functional scores in combined tears. Regardless of tear type, a healed SSC was associated with increased shoulder strength.
Keywords
The successful repair of subscapularis (SSC) tears significantly improves postoperative outcomes in rotator cuff repair (RCR) by enhancing shoulder stability, function, and healing of the other rotator cuff components.7,16,28,30 SSC tears may be identified in up to half of cases involving arthroscopically repaired rotator cuff tears (RCTs).10,31 The SSC tear can present as an isolated tear or be combined with additional rotator cuff tearing.10,14,31 Regardless of tendon involvement, arthroscopic repair of SSC tears is important for restoring shoulder function.3,14,23,29
SSC retears after repair are not uncommon, with rates reported as high as 32% for isolated tears and combined tears.2,11,13,17,23 Unhealed SSC tears after arthroscopic repair have demonstrated inferior functional outcomes, regardless of whether there is an isolated or combined SSC tear.10,12 However, studies comparing these patterns are limited, and the effect the SSC has on functional outcomes after arthroscopic repair of isolated and combined SSC tears requires further study. 23
The primary objective of this study was to compare the clinical outcomes of arthroscopic RCR (ARCR) of isolated SSC tears to those with SSC tears combined with supraspinatus (SS) and/or infraspinatus (IS) tears. The secondary objective was to evaluate the effect of SSC healing on postoperative outcomes. We hypothesized that clinical outcomes would improve after arthroscopic repair in patients with isolated SSC tears and in patients with SSC tears combined with SS and/or IS tears. In addition, we hypothesized that those with an unhealed SSC with concomitant tears would have lower functional scores compared with those with an unhealed SSC after isolated SSC repair.
Methods
Study Design
A retrospective study was conducted using prospectively collected data from patients with isolated or combined SSC tears who underwent ARCR at a single institution between 2011 and 2021. The inclusion criteria were patients with any SSC tear who underwent ARCR, baseline patient-reported outcomes (PROs), and minimum 2-year follow-up. Patients with a history of previous ipsilateral shoulder surgery, those who had ARCR without SSC tear, proximal humeral fracture, glenoid fracture, inaccessible magnetic resonance imaging (MRI) scans or insufficient images for evaluation, inaccessible or incomplete physical examination record, or incomplete intraoperative documentation were excluded from this study. Institutional review board approval was obtained before commencing the study. No funding was received for the study.
Patients who met the inclusion criteria were invited to the clinic for an ultrasound assessment. The assessment was performed by an independent orthopaedic surgeon blinded to tear size and repair technique (A.I.K.). During this visit, patients filled out questionnaires including the American Shoulder and Elbow Surgeons (ASES) score, Subjective Shoulder Value (SSV), and visual analog scale (VAS) pain scale, as well as information about their return to activity; and postoperative satisfaction was assessed dichotomously, considering overall shoulder symptoms and function. During the clinical evaluation, range of motion (ROM) was assessed using a goniometer, and isometric strength was assessed using a handheld dynamometer.
The patients were categorized into 3 groups based on the presence of SSC tears and combined with other rotator cuff tears: isolated SSC tears, anterosuperior rotator cuff tears with SSC tear (AS-RCT) (involving an SS tear accompanied by SSC tear), and posterosuperior rotator cuff tears with SSC tear (PS-RCT) (involving the SS and IS tendons accompanied by a SSC tear). The criteria for determining surgery for isolated SSC tears included full-thickness tears or partial tears exceeding 15% in a cephalocaudal direction.
Study Variables
Demographic variables, including age, sex, tobacco use, and length of follow-up, were collected. The Charlson Comorbidity Index, which includes 17 different comorbidities associated with mortality and assigns weights ranging from 1 to 6 points (0-29), was used to standardize comorbidities, and the Charlson Comorbidity Index score was calculated by dividing the patient's score by 29 (score received/29 = %).8,22 Active ROM and PROs were documented pre- and postoperatively at a minimum 2-year follow-up. Preoperative ROM measurements, including forward flexion (FF), external rotation (ER) at the side, and internal rotation (IR), were recorded preoperatively by the treating surgeon (P.J.D.) or a physician assistant, while the follow-up measurements were assessed by the same independent orthopaedic surgeon who performed the ultrasound evaluation. IR was numerically scaled based on the nearest spinal level achieved with the thumb (ie, T10 = 10, T12 = 12, L2 = 14, L4 = 16, S1 = 18, hip = 20). PROs included ASES, VAS for pain, and SSV. Complications, revision surgeries, and satisfaction were all recorded for analysis.
Preoperative MRI Evaluation
All MRI scans were performed at a single institution with a 1.5-T magnet and with the arm in a neutral position and a shoulder coil. No intra-articular or intravenous gadolinium was administered. The Goutallier classification was assessed and documented by 1 high-volume fellowship-trained shoulder surgeon (P.J.D.) preoperatively for each rotator cuff muscle on T1 sagittal MRIs using the most medial image where the scapular spine connected with the body of the scapula.5,33 This classification system consists of 5 grades, scored from 0 to 4. Grade 0 indicates the absence of fat, grade 1 indicates the presence of some fatty streaks, grade 2 indicates a higher proportion of muscle compared with fat, grade 3 indicates an equal presence of fat and muscle, and grade 4 indicates a higher proportion of fat compared with muscle. The SSC was also divided into the upper and lower half for grading based on the division described by Collin et al. 6
The coracohumeral distance was evaluated by measuring the narrowest distance between the cortical border of the coracoid and the cortical border of the humeral head on T2-weighted axial images obtained from MRI scans, following the criteria established by previous studies.19,25 The axial images were set at the point where the subcoracoid space was at its narrowest. Measurements were made by an independent orthopaedic surgeon (A.I.K.). Three measurements were recorded, and the mean was taken for analysis.
Isometric Muscle Strength Measures
Isometric strength measurements were conducted by the same surgeon who performed the ultrasound evaluation using a manual muscle-testing dynamometer with the patient in the standing position. The strength of the SSC muscle was evaluated using the belly press (BP) test. During the test, the patient was instructed to press the hand dynamometer between the palm and abdomen. To assess ER strength, the participants’ elbows were flexed at a 90° angle, and their arms were positioned at the side. ER strength was measured with the hand dynamometer placed on the dorsal aspect of the forearm, 2 cm proximal to the ulnar styloid process. To determine the FF strength, maximal arm extension strength was measured using a dynamometer. The patient’s arms were positioned at a 90° FF in the plane of the scapula, with the elbows fully extended and the forearms in a half pronation position. The hand dynamometer was placed on the dorsal aspect of the forearm, approximately 2 cm proximal to the ulnar styloid process. For each participant, the mean of the 3 independent measurements was taken.
Ultrasound Examination
SSC tendon healing was graded using the Barth modification of the Sugaya classification for ultrasound assessment of RCR. 1 Grade I designated tendons with sufficient thickness and normal structure. Grade II indicated sufficient thickness with partial hypoechogenicity. Grade III indicated insufficient thickness without discontinuity. Grade IV repairs demonstrated minor discontinuity in the tendon. Grade V repairs demonstrated major discontinuity. Repairs graded 1, 2, and 3 were considered healed.1,15
Surgical Technique and Arthroscopic Findings
All arthroscopic procedures were performed by a single surgeon (P.J.D.). Patients were positioned in the lateral decubitus position, and conventional portals were used (ie, posterior, anterosuperior, and lateral). SSC tendon integrity was evaluated from the posterior viewing portal with 30° and 70° arthroscopes. Intraoperatively, SSC tear type was documented according to the Lafosse classification18,27 (ie, types 1 to 5) and SSC tear size as a percentage (ie, % cephalad to caudal). In addition, long head biceps tendon integrity (ie, intact, subluxated, partial tear, or complete tear), SS tear (ie, intact, partial tear, complete tear), and IS tear (ie, intact, partial tear, complete tear) were reported.18,27
After arthroscopic examination of the joint, biceps tenodesis was performed on patients with impaired biceps sling or biceps pathology on physical examination or imaging. The width of the subcoracoid space was evaluated. Coracoplasty was performed if there was a narrowed subcoracoid space (<7 mm) or if a coracoid spur was present. SSC repair was performed with a single-row or double-row technique based on the tear pattern and tendon mobility. After repairing the SSC, the posterosuperior cuff was evaluated. A double-row repair was the preferred choice based on the tear pattern unless it was under excessive tension or had tendon loss. In such cases, a single-row repair or a single-row repair with rip-stop technique was performed instead. A limited acromioplasty with preservation of the coracoacromial ligament was routinely conducted. All tears were fully repairable at the time of surgery.
Postoperatively, patients were immobilized in a sling for 4 weeks for SSC tears of ≤50% of the footprint in the cephalocaudal axis and for 6 weeks for tears >50% of the footprint. After sling discontinuation, patients were permitted to engage in passive ER and FF. Strengthening exercises and passive IR began 3 months postoperatively, with full return to activity, including sports, at 6 months.
Statistical Analysis
Categorical variables were characterized using absolute and proportional frequencies, whereas continuous variables were described by means and standard deviations. The statistical analysis included the chi-square test to assess associations among categorical variables, and the t test was employed to compare means among continuous variables. The Shapiro-Wilk test was used to assess the normality of the numerical data distribution. Parametric tests were employed to compare groups when data were normally distributed, and nonparametric tests were utilized when data were not normally distributed. In pairwise group comparisons, the Bonferroni correction was applied to adjust P values in parametric tests, while the Dunn-Bonferroni correction was used in nonparametric tests to control for multiple comparisons. The IBM SPSS Version 25 program was used to evaluate the data. A threshold of .05 was used to denote statistical significance.
Results
A total of 1018 patients were identified from the database of patients who underwent ARCR for isolated or combined SSC tears during the study period. Of these, 588 patients met the study's inclusion criteria, with 279 undergoing ultrasound evaluation (Figure 1). Baseline characteristics are summarized in Table 1. Male predominance was observed in cases of isolated SSC tears, AS-RCT, and PS-RCT, comprising 62.8% (n = 49), 60.9% (n = 204), and 69.7% (n = 122) of cases, respectively (P = .14). The mean follow-up periods for isolated SSC, AS-RCT, and PS-RCT were 58.3 ± 29.6 months, 59.9 ± 29.7 months, and 58.1 ± 29.9 months, respectively (P > .05). Isolated SSC accounted for 13.3% (n = 78) of the cases, AS-RCT constituted 57% (n = 335) of the cases, and 3 tendon tears (PS-RCT) made up 29.8% (n = 175) of the cases.

A total of 1018 patients were identified from a registry of individuals who underwent arthroscopic rotator cuff repair for isolated or combined subscapularis tears at a single institution between 2011 and 2021. Among these, 588 patients met the study's inclusion criteria. Postoperative ultrasound assessments for subscapularis repair integrity were conducted in 279 of these patients.
Baseline Characteristics of Arthroscopic Isolated and Combined Subscapularis Repair (N = 588) a
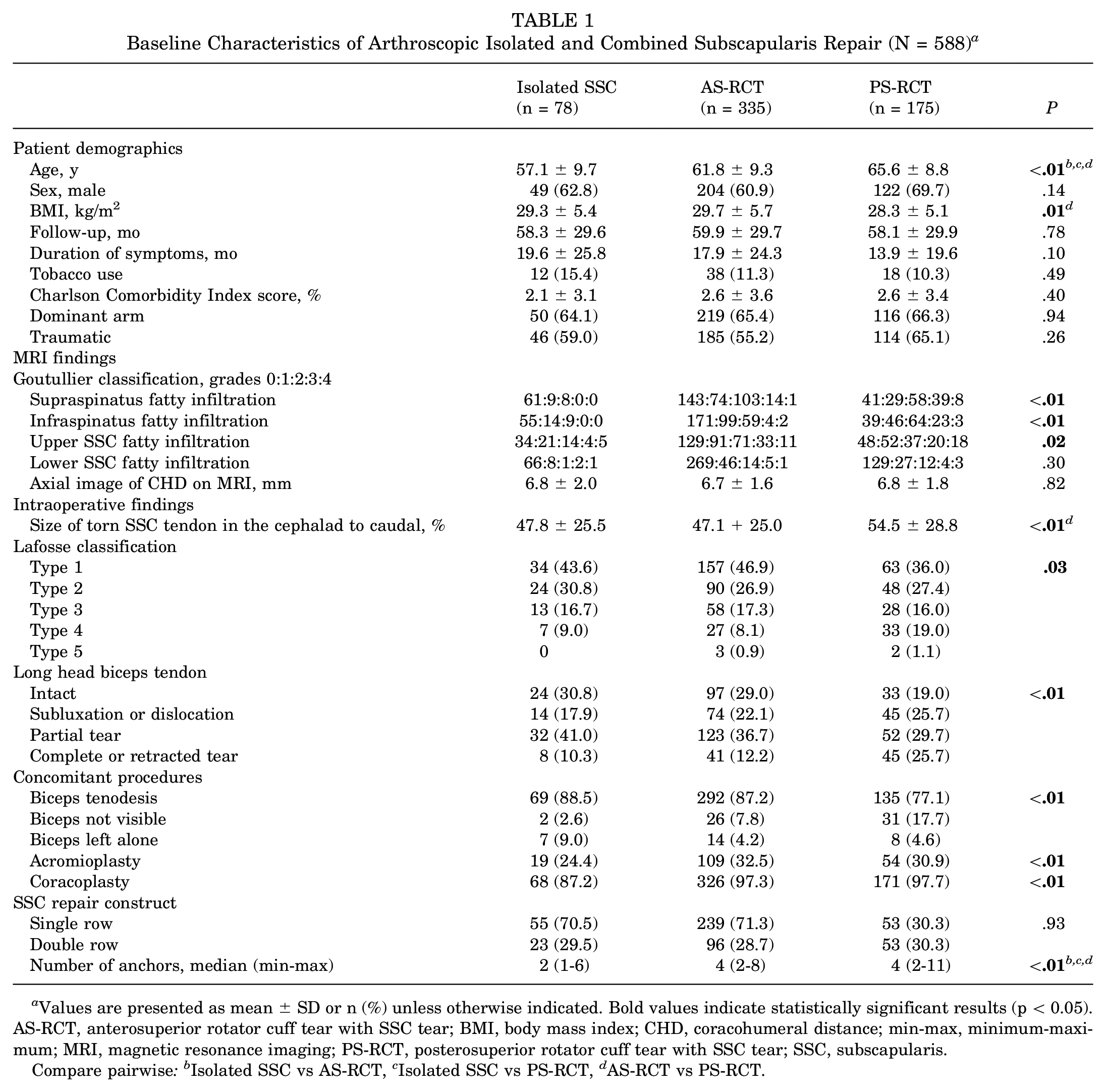
Values are presented as mean ± SD or n (%) unless otherwise indicated. Bold values indicate statistically significant results (p < 0.05). AS-RCT, anterosuperior rotator cuff tear with SSC tear; BMI, body mass index; CHD, coracohumeral distance; min-max, minimum-maximum; MRI, magnetic resonance imaging; PS-RCT, posterosuperior rotator cuff tear with SSC tear; SSC, subscapularis.
Compare pairwise: bIsolated SSC vs AS-RCT, c Isolated SSC vs PS-RCT, d AS-RCT vs PS-RCT.
Functional Outcomes
Overall, PROs and ROMs showed significant improvements from baseline to the final follow-up in all 3 groups (P < .01) (Table 2). There was no statistically significant difference with pre- to postoperative ASES change between isolated SSC and AS-RCT (P > .05), or between isolated SSC and PS-RCT groups (P > .05). However, the ASES improvement was significantly higher for the AS-RCT group compared with the PS-RCT group (P = .01). There was no statistically significant difference when comparing the pre- to postoperative change in ROM between the groups (P > .05). The rates of return to activity in the isolated SSC, AS-RCT, and PS-RCT groups were 85.9% (n = 67), 83% (n = 278), and 77.1% (n = 135), respectively (P = .17). Similarly, the satisfaction rates for these groups were 91.0% (n = 71), 88.1% (n = 295), and 86.3% (n = 151), respectively (P = .64).
Functional Outcomes of Isolated SSC Repair, SSC + SS Repair, and SSC + SS + IS Repair a

Values are presented as mean ± SD or mean (95% CI) unless otherwise indicated. Bold values indicate statistically significant results (p < 0.05). ASES, American Shoulder and Elbow Surgeons; AS-RCT, anterosuperior rotator cuff tear with SSC tear; en: total number of patients in each group who were assessed via ultrasound; ER, external rotation; FF, forward flexion; IR, internal rotation; IS, infraspinatus; PS-RCT, posterosuperior rotator cuff tear with SSC tear; SS, supraspinatus; SSC, subscapularis; SSV, Subjective Shoulder Value; VAS, visual analog scale.
Pairwise comparison: isolated SSC vs PS-RCT.
Pairwise comparison: AS-RCT vs PS-RCT.
Pairwise comparison: isolated SSC vs AS-RCT.
Tendon Healing
Of the 588 patients who were contacted and agreed to a clinic visit, 279 (47.4%) underwent ultrasound assessments during their final follow-up, as presented in Table 3. Overall, 89.2% (249 of 279) SSC repairs healed, including 88.1% (n = 37 out of 42) for the isolated SSC group, 91.6% (n = 153 out of 167) for the AS-RCT group, and 84.3% (n = 59 out of 70) for the PS-RCT group (P = .24).
Functional Outcomes of Isolated SSC Repair, AS-RCT Repair, and PS-RCT Repair in Relation to SSC Healing Status (n = 279) a

Bold values indicate statistically significant results (p < 0.05). AS-RCT, anterosuperior rotator cuff tear with SSC tear; ASES, American Shoulder and Elbow Surgeons; ER, external rotation; FF, forward flexion; IR, internal rotation; PS-RCT, posterosuperior rotator cuff tear with SSC tear; SSC, subscapularis; SSV, Subjective Shoulder Value; VAS, visual analog scale.
Comparison of pre- to postoperative changes between healed and unhealed SSC.
In the isolated SSC group, significant pre- to postoperative improvements were observed in VAS, ASES, and SSV, both when the SSC healed (P < .01) and when it did not heal (P = .03, P = .02, and P = .02, respectively). All ROM measurements improved in healed repairs. However, in unhealed isolated SSC tears, there was no significant improvement in FF (P = .07) or IR (P = .25).
In AS-RCT, significant improvements were observed in VAS, ASES, and SSV, regardless of SSC healing (P < .01). There was a significant difference when comparing pre- to postoperative PRO changes between healed and unhealed SSC cohorts (P < .01). While ROM improved significantly in cases with SSC healing (P < .01), this was not the case in unhealed cases (P > .05). When evaluating ROM, there was a significant difference in active IR (P < .01) between the healed and unhealed groups, but no difference in active FF (P = .26) or ER (P = .07).
In the PS-RCT group, there was a significant improvement in PROs regardless of healing status (P < .01). However, while patients with a healed SSC significantly improved in ROM (P < .01), this was not observed in unhealed cases (P > .05). When comparing pre- to postoperative changes between groups, there was a significant difference in ASES and SSV (P < .01) between healed and unhealed SSC cases, but no significant difference in VAS (P = .20). Regarding ROM, a significant difference was found in active IR and ER (P < .01) between the healed and unhealed groups, but not with active FF (P = .22).
In the isolated SSC group, the return to the previous activity level rates were 60% for the unhealed (n = 3) group and 83.8% for the healed (n = 31) group (P = .24) (Table 4). AS-RCT showed a significantly higher level of return to previous activity in the healed SSC (86.9%; n = 133) compared with the unhealed (28.6%; n = 4) group (P < .01). Similarly, in PS-RCT, the return to the previous activity level was significantly higher in the healed SSC (91.5%; n = 54) compared with the unhealed (18.2%; n = 2) group (P < .01). Satisfaction rates for patients with unhealed SSC in the isolated SSC group did not differ significantly (P = .49) from patients with healed SSC, while patients with a healed SSC in AS-RCT and PS-RCT demonstrated significantly higher satisfaction rates (P < .01) (Table 4).
Comparison of Subscapularis Healing Effect on Return to Function and Patient Satisfaction in Isolated and Combined Subscapularis Tears a

Bold values indicate statistically significant results (p < 0.05). SSC, subscapularis; AS-RCT, anterosuperior rotator cuff tear with SSC tear; PS-RCT, posterosuperior rotator cuff tear with SSC tear.
Fisher exact test.
Isometric Muscle Strength
Isometric strength measurements for ER strength, BP strength, and FF strength are presented in Table 5. While there was no significant difference when comparing ER and BP strength between groups (P > .05), significant differences were observed between FF strength in isolated SSC and PS-RCT, as well as between AS-RCT and PS-RCT (P = .04 and P = .01, respectively). ER, BP strength, and FF strength were significantly higher in healed SSC cases compared with unhealed cases (P < .01). No differences in strength were found between the healed isolated SSC, AS-RCT, and PS-RCT groups (P > .05).
Postoperative Isometric Strength Measurements Based on Subscapularis Healing Status a

Values are presented as mean ± SD unless otherwise indicated. Bold values indicate statistically significant results (p < 0.05). AS-RCT, anterosuperior rotator cuff tear with SSC tear; BP, belly press ER, external rotation; FF, forward flexion; PS-RCT, posterosuperior rotator cuff tear with SSC tear; SSC, subscapularis.
Comparing overall strength measurement of isolated SSC, AS-RCT, and PS-RCT.
Comparison of strength measurements in individuals with healed SSC among isolated SSC, AS-RCT, and PS-RCT.
Comparison of strength measurements in individuals with unhealed SSC among isolated SSC, AS-RCT, and PS-RCT.
Pairwise comparison: isolated SSC vs AS-RCT.
Pairwise comparison: isolated SSC vs PS-RCT
Pairwise comparison: AS-RCT vs PS-RCT.
Discussion
The main finding of this study was that arthroscopic SSC repair in cases of isolated SSC tear or combined rotator cuff tears led to significant improvement in PROs and ROM. In total, 47% of patients underwent ultrasound examination. SSC healing, patient satisfaction, and return to previous activity were observed in >80% of patients without differences between groups. In the isolated SSC group, healing status did not affect ASES and SSV scores. However, in the AS-RCT and PS-RCT groups, lower ASES and SSV scores were observed in unhealed SSC cases. Rates of return to previous activity level and satisfaction were higher when the SSC healed in the AS-RCT and PS-RCT groups. However, the isolated SSC group showed comparable return to previous activity level and satisfaction when considering SSC healing status. Isometric muscle strengths were also higher in those whose SSC had healed.
Previous studies have demonstrated that SSC tendon repair improves postoperative outcomes in both isolated SSC tears and combined rotator cuff tears.10,21,24,26 Consistent with previous studies, our research also demonstrated statistically significant improvements in all PROs and ROM after SSC repair, in cases of isolated SSC tears and combined tears. In a retrospective study by Meshram et al 23 comparing isolated SSC (n = 30) and AS-RCT (n = 110) with a minimum 2-year follow-up, postoperative ASES scores were similar among groups (isolated SSC, 93.7 ± 8.9; AS-RCT, 92.0 ± 13.6; P = .52). In line with Meshram et al, Jeong et al 14 reported no differences in PROs and ROM between isolated SSC repair and AS-RCT repair. Monroe et al 24 compared postoperative Patient-Reported Outcomes Measurement Information System for Upper Extremity (PROMIS-UE) and VAS between 4 groups according to the presence of a complete or partial isolated SSC tear and the association of an SS and/or IS tear. No significant difference in the mean postoperative PROMIS-UE score was found among groups, including isolated partial SSC tears, complete SSC tears with SS and/or IS repair, and isolated complete SSC tears (P = .61). On the other hand, in our study, when comparing the ASES pre- to postoperative change between the groups, a significant difference was observed between the AS-RCT group and PS-RCT (43.2 vs 38.0; P = .01), but no significant difference was found when comparing SSV and ROM (P > .05). It is worth noting that PS-RCT patients in the present study were older (AS-RCT, 61.8 ± 9.3 years; PS-RCT, 65.6 ± 8.8; P < .01), had larger SSC tears (tear size for AS-RCT, 47.1% + 25%; PS-RCT, 54.5% ± 28.8%; P < .01), and had worse preoperative ROM. These results demonstrate that despite lower functional scores observed in PS-RCT, significant improvements in PROs and ROM after SSC repair can be achieved, irrespective of the tear combination.
SSC repair not only significantly improves ARCR outcomes but also enhances shoulder stability and function when a tear is present.7,16,28,30 In this study, we did not find differences in SSC healing rates among groups. In line with our results, Meshram et al 23 found no significant differences in the rate of SSC retear after arthroscopic repair in isolated SSC (16.7%) and combined AS-RCT (8.5%) tear patients (P = .34). Similarly, in our study, the rates of SSC healing were 88.1%, 91.6%, and 84.3% for the isolated SSC, AS-RCT, and PS-RCT groups, respectively (P = .24). In contrast, Jeong et al 14 did not report any retear in isolated SSC patients but an 8.8% rate of SSC retear in AS-RCT patients.
In the current study, SSC healing showed better outcomes in terms of ASES and SSV compared with SSC retears in the AS-RCT and PS-RCT groups (P < .01). However, when comparing ASES and SSV for isolated SSC tears, there was no statistically significant difference when considering healing status (P = .48 and P = .40, respectively). In a study by Flury et al, 10 comparing isolated SSC tears (n = 32) with those combined with SS tears (n = 31), they reported a 13% retear rate for SSC across all cohorts. The group with retears showed a lower FF score compared with the intact group (96% vs 69%; P = .009). In a case series of 101 arthroscopic SSC repairs with a minimum of 2 years of follow-up, Shibayama et al 29 reported a 5% retear rate, and the failure-to-heal group demonstrated lower PROs (ASES score, 81 vs 93; P = .003) compared with the intact group. Similar to our study, successful SSC healing in the AS-RCT and PS-RCT groups resulted in better outcomes in terms of ASES and SSV compared with cases with unhealed SSC tears (P < .01). Nevertheless, all groups exhibited improved scores compared with their preoperative status, indicating reduced pain and improved function. In line with our study, Yoon et al 32 reported a 78.6% retear rate in a consecutive case series involving isolated SSC repairs with Goutallier grade 3 to 4 atrophy. Despite the high retear rate, they noted a significant improvement in ASES (△31.6 ± 9.1; P < .001) and SSV (△37 ± 7.6; P < .001). Additionally, our study demonstrated that there is no significant difference in rates of return to previous activity level and satisfaction between individuals with healed and unhealed SSC in isolated SSC; however, those with unhealed SSC in AS-RCT and PS-RCT experience significantly lower rates in both return-to-previous activity level and satisfaction. This demonstrates that SSC healing plays a critical role in overall RCR outcomes. This also underscores that patient satisfaction is influenced not only by pain relief and functional improvement but also by the success of specific repair procedures, particularly the SSC repair.
Evaluating shoulder strength provides insights into the functional rotator cuff muscle status, which is closely associated with patients’ overall function and quality of life. 20 In this study, there were no statistically significant differences with postoperative isometric muscle strength measurements in ER and BP (P > .05). Consistent with the study by Jeong et al, 14 a comparison of postoperative BP strength between patients with isolated SSC tears and patients with AS-RCT revealed no significant difference between these groups (5.6 kg and 5.4 kg, respectively; P = .25). On the other hand, in our study, FF strength in the PS-RCT group was lower than in isolated SSC or AS-RCT groups (P = .04 or P = .01, respectively). This may be due to PS-RCT’s simply being more extensive compared with isolated SSC or AS-RCT tears. This also may be caused by individuals in the PS-RCT group being older than those in the other groups (P < .01). Cofield et al 4 reported that older age was associated with reduced postoperative FF strength (r = −0.23; P = .02) after a mean follow-up of 13.4 years. Notably, postoperative strengths were significantly higher in those with SSC tendon healing (P < .01). These findings not only emphasize the substantial effect of SSC healing on shoulder functional scores but also underscore its broader influence on rotational strength, reinforcing the critical role of SSC tendon healing in overall postoperative outcomes.
Limitations
This study has several limitations worth noting. First, due to the inherent constraints of a retrospective study design, there was a dropout of some patients who underwent ARCR for isolated or combined SSC tears at our institution. Of the 588 patients, 279 underwent ultrasound assessment of SSC healing. This introduces the potential for selection bias and the possibility of unanticipated confounding factors that could affect the accuracy of the results. Second, the evaluation was limited to assessing postoperative SSC healing exclusively through ultrasound, without considering the status of the other superior cuff tendons. This limitation has the potential to create differences in functional outcome and may affect the overall healing trajectory of the SSC. Also, tendon healing was assessed using only ultrasound assessments, with no concomitant additional validation using MRI or computed tomography. However, it is important to note that ultrasound has been verified to be equivalent or even superior to MRI evaluating RCTs.9,34 Additionally, the evaluation of SSC healing via ultrasound was conducted by a single observer, which may introduce possible observer bias. To minimize this potential bias, an independent orthopaedic surgeon with ultrasound training was assigned to the task. Finally, the comparison of the SSC healing effect on postoperative outcomes in isolated and combined SSC tears may be limited by sample size, and thus caution should be used when interpreting these results.
Conclusion
Both isolated and combined SSC repairs showed improvement in PROs and ROM. SSC healing rates did not differ between isolated and combined SSC tears. While failure to heal did not affect clinical outcomes of isolated SSC tears, an unhealed SSC was associated with lower functional scores in combined tears. Regardless of tear type, a healed SSC was associated with increased shoulder strength.
Supplemental Material
sj-doc-1-ojs-10.1177_23259671251332638 – Supplemental material for Clinical Outcomes of Patients Undergoing Isolated and Combined Subscapularis Repair
Supplemental material, sj-doc-1-ojs-10.1177_23259671251332638 for Clinical Outcomes of Patients Undergoing Isolated and Combined Subscapularis Repair by Ali Ihsan Kilic, Diego Gonzalez-Morgado, Javier Ardebol, Lisa Galasso, Matthew Noble, Mariano E. Menendez and Patrick J. Denard in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted November 19, 2024; accepted December 30, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.N. has received a grant from Arthrex and education payments from Rock Medical Orthopedics. L.G. has received a grant from Arthrex, education payments from Arthrex and Pinnacle, and hospitality payments from Stryker. M.E.M. has received hospitality payments from Arthrex, Stryker, Encore Medical, Steelhead Surgical, Smith & Nephew, and Medical Device Business Services and education payments from Arthrex, Medwest Associates, and Steelhead Surgical. P.J.D. has received nonconsulting fees from Arthrex, consulting fees from Arthrex and Pacira Pharmaceuticals, education payments from Steelhead Surgical, and royalties from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Southern Oregon Institutional Review Boards (No. 22-008).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.