
Abstract
Background:
Tears of the subscapularis are not as common as the other rotator cuff muscles and hence not as many arthroscopic repair techniques have been previously described in the literature. The purpose of this study is to evaluate the clinical outcomes in patients undergoing arthroscopic subscapularis repairs (with and without repairs of the other cuff muscles) using a technique devised by the senior author of this study.
Methods:
A retrospective study of 40 consecutive patients who underwent arthroscopic subscapularis repair at a single centre, by a single surgeon from 2009 to 2014. All patients were assessed preoperatively and post-operatively at 3, 6, 12 and 24 months. The Visual Analogue Scale (VAS), Constant–Murley Shoulder Score (CMSS), University of California at Los Angeles (UCLA) Shoulder Score and Oxford Shoulder Score (OSS) were recorded and used.
Results:
At 24 months follow-up, the VAS for pain improved from 6 (±2) points preoperation to 0 (±1) points. The CMSS improved from 41 (±18) points preoperation to 71 (±15). The relative CMSS improved from 55 (±24%) preoperation to 96 (±22%; % of the uninjured side). The ULCA Shoulder Score improved from 15 (±5) points preoperation to 30 (±4). The OSS improved from 28 (±12) points preoperation to 45 (±5). p < 0.001 for all outcomes measured.
Conclusion:
Overall clinical outcomes are favourable at 2 years post-operatively. The described technique is an effective method for arthroscopic subscapularis repair in the Asian population.
Keywords
Introduction
Rotator cuff tears are increasingly prevalent in ageing population. These frequently involve the supraspinatus tendon/muscle and sometimes the subscapularis. Compared with the supraspinatus, subscapularis tears can be technically challenging to repair and were traditionally repaired with the open technique, 1 –3 but recent studies have shown arthroscopic techniques have also managed to produce functionally good results. 4 –11
Isolated tears of the subscapularis tendons are not common, 3 and frequently occur in conjunction with other rotator cuff muscles like the supraspinatus. Most commonly patients complain of pain and weakness in the shoulder which may or may not be precipitated by an injury/dislocation of the shoulder.
The subscapularis attaches to the lesser tuberosity of the humerus and its anatomical footprint is of significance when attempting to repair the tendon. An anatomical cadaveric study by D’Addesi et al. 12 showed that the subscapularis tendon footprint is broad proximally and tapered distally. A more recent anatomical cadaveric study by Yoo et al. 13 described the footprint in facets and concluded that the first two facets (the superior facets) together represent approximately 60% of the tendon’s insertion area. As such, repairs should be made with these considerations in mind.
In this study, we describe a novel surgical technique which takes into account the anatomical footprint of the subscapularis tendon and aim to report the clinical outcomes at 24 months post-operation.
Methods
This study was approved by our hospital’s ethics committee (Singhealth Centralised Institutional Review Board (CIRB): 2016/2397) and carried out in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki. Informed consent was obtained from all the patients.
Between 2009 and 2014, 40 consecutive patients who underwent arthroscopic subscapularis repair by a fellowship-trained shoulder surgeon (the senior author) were prospectively followed up for 2 years. The indications for surgery are: (1) persistent shoulder pain limiting patients’ function and (2) subscapularis tears confirmed with either ultrasonography or magnetic resonance imaging arthrography. Tears were re-examined intraoperatively and graded using the Lafosse classification 3 (see Table 1). All patients who underwent arthroscopic repair of the subscapularis muscle whether isolated or in combination with repair of other structures were included. Patients who had not been followed up for a minimum of 2 years post-operation were excluded from the study.
Lafosse subscapularis tear classification. 3

Technique
All patients underwent general anaesthesia for the operation and were placed in the beach chair position. After cleaning and preparation in a sterile manner, the standard posterior arthroscopic portal was introduced into the shoulder (see Figure 1). The working arthroscopic portals for instruments used were the anterosuperior and anterolateral portals (see Figure 2). After inspection of the glenohumeral joint and the other tendons, the subscapularis tendon was identified and its footprint on the lesser tuberosity of the proximal humerus was prepared with an arthroscopic shaver, a radio frequency ablation device and an awl. The torn ends of the subscapularis tendon would be derided and freshened with an arthroscopic shaver. If the subscapularis tear was complete, anterior (from the posterolateral coracoid and deltoid fascia), superior (from the undersurface of coracoid neck and base) and posterior (from glenoid neck) releases were carried out to mobilize the tendon.

Subscapularis tendon tear viewed from a posterior arthroscopic portal.

Anterosuperior and anterolateral working arthroscopic portals with a posterior viewing portal.
All cases were repaired using double-loaded bioabsorbable suture anchors (HEALIX®, Mitek (Raynham, United State) with ORTHOCORD® sutures or HEALICOIL®, Smith & Nephew (Tolaram, Singapore) with ULTRABOND® sutures).
The first suture anchor would be placed onto facet 1 of the subscapularis footprint via the anterior superior portal and screwed into place. The suture threads would then be pulled through the anterior superior portal and separately held by artery forceps to prevent entanglement. Three limbs of suture thread were then subsequently loaded onto an arthroscopic suture passing device (e.g. EXPRESSEW, Mitek; or TRUEPASS, Smith & Nephew) and threaded through the subscapularis tendon sequentially. Each time a suture was threaded through the tendon, it would then be pulled through a different portal. The first two suture threads (from one load) would be threaded through with one superiorly and another inferiorly approximately 1 cm apart to create a horizontal mattress about 1 cm medial from the edge of the subscapularis tendon (depicted as red threads in Figure 3, sequence 3). One suture thread from the second load would then be threaded through the tendon in between the two existing threads but in a more medial position (depicted as blue thread in Figure 3, sequence 3). The two threads from the first load (red threads) would then be pulled through the anterior superior portal and tied outside the shoulder with a Duncan knot. This would then be further secured with two simple half hitch knots. The suture ends from the first load would then be cut with an arthroscopic suture cutter. The first suture from the second load (that was threaded medially) would then be tied with simple sutures perpendicular to the secured vertical mattress stitch. Duncan knots are similarly used. This creates a cruciate-like suture configuration: a vertical mattress suture crossed with a simple horizontal stitch (Figure 3, sequence 5). Usually at this point, it is noticed that this does not secure the top most portion of the subscapularis tendon firmly onto the footprint. Hence, a technique is used in which one of the suture threads from the second load would then be used to re-enforce the superior portion of the subscapularis with a whip stitch (Figure 3, sequence 6). The two suture threads from the second suture load would then be threaded through the snare of a knotless suture anchor (outside the portal; Figure 3, sequence 7), and then this would then be placed just lateral to the bicipital groove (Figure 3 sequence 8). The suture threads would be tightened and tensioned (shoulder in neutral rotation) before using a mallet to advance the knotless suture anchor into the bone. Examples of knotless suture anchor devices used were VERSALOK® (Mitek) and FOOTPRINT® (Smith & Nephew). The completed repair would be tested with an arthroscopic probe, and then passive range of motion of the shoulder would be assessed.

Illustration of the repair technique.
In cases where there were other structures repaired (Superior Labral tear from Anterior to Posterior [SLAP] lesion, bankart, supraspinatus), these were repaired prior to the subscapularis. The long head of the biceps tendon would be assessed intraoperatively, if found to be frayed or torn, either a biceps tenodesis or tenotomy was performed depending on the patient’s premorbid function and age. Generally, those above the age of 60 underwent a biceps tenotomy while those younger than 60 underwent a subpectoral tenodesis.
Post-operatively, the patients were admitted to the ward for overnight observation. The arm would be placed in an arm sling. They were allowed passive range of motion exercises from post-operation day 1, before starting on strengthening exercises at 6 weeks post-operation with regular outpatient physiotherapy.
All patients were assessed preoperatively and post-operatively at 3, 6, 12 and 24 months. The Visual Analogue Scale (VAS), Constant–Murley Shoulder Score (CMSS), University of California at Los Angeles (UCLA) Shoulder Score and Oxford Shoulder Score (OSS) were recorded by an independent healthcare professional during these outpatient visits. Repeated surgery within 24 months was also documented.
Statistical analysis
Power analysis was done prior to the conduct of this study, based on the improvement in CMSS and OSS from preoperation to 24 months post-operation. The minimally clinically important difference (MCID) of CMSS and OSS were reported to be 10.4 and 6 points, respectively. 14,15 To detect an 11-points improvement in CMSS from a baseline of 41 at a power of 0.80, a sample size of at least 24 patients would be required. To detect a 6-points improvement in OSS from a baseline of 28 at a power of 0.80, a sample size of at least 34 patients would be required.
We carried out the statistical analysis using SPSS® 19.0 (IBM, Armonk, New York, USA). Statistical significance was defined as a p value of ≤0.05. The Student’s paired t-test was used to compare preoperation scores with post-operation scores at 3, 6, 12 and 24 months follow-up.
Results
The age (mean ± standard deviation) was 62 ± 9 (range 41–79) while the body mass index was 25.4 ± 4.0 kg/m2 (range 17.0–36.0). There were 19 males and 21 females; 9 left shoulders and 31 right shoulders. All cases not followed up for at least 2 years were excluded from the statistical analysis.
Majority of the cases were Lafosse type 1 (28 of 40), with the remainder consisting of type 2, 3 and 4 tears (see Table 2). Majority of the subscapularis tears were repaired together with other structures including the supraspinatus, labral tears and biceps tenodesis (see Table 3). There were a total of five cases of isolated subscapularis repairs.
Type of tear distribution.

Type of repair distribution.

aOther structures include biceps tenodesis and labral repairs.
Overall, there was significant improvement in all of the shoulder scores at 24 months post-operation (see Figure 4 and Table 4). There was one patient who required a revision of arthroscopic subscapularis repair due to re-tear of the subscapularis tendon and another patient who required a subsequent arthroscopic supraspinatus repair (prior subscapularis repair was intact). No patients were lost to follow up.

Scores for preoperative, 3 months, 6 months, 1 year and 2 years post-operative.
Scores for preoperative, 3 months, 6 months, 1 year and 2 years post-operative.
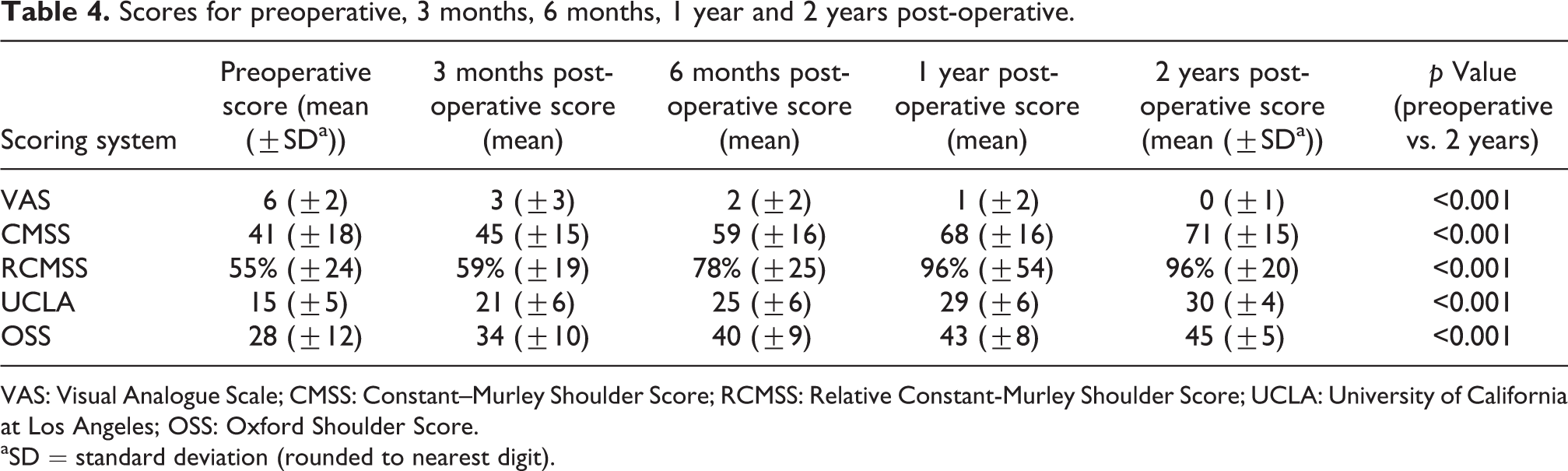
VAS: Visual Analogue Scale; CMSS: Constant–Murley Shoulder Score; RCMSS: Relative Constant-Murley Shoulder Score; UCLA: University of California at Los Angeles; OSS: Oxford Shoulder Score.
aSD = standard deviation (rounded to nearest digit).
The VAS improved from 6 ± 2 points preoperation to 0 ± 1 points at 24 months follow-up. The CMSS improved from 41 ± 18 points preoperation to 71 ± 15 at 24 months. The relative CMSS (when compared to the uninjured side) improved from 55 ± 24% preoperation to 96 ± 22% at 24 months (% of the uninjured side). The UCLA Shoulder Score improved from 15 ± 5 points preoperation to 30 ± 4 at 24 months. The OSS improved from 28 ± 12 points preoperation to 45 ± 5 at 24 months (p < 0.001).
Discussion
The footprint of the subscapularis is of great importance when carrying out its repair, and this has been recognized by many other authors as it is evident in their repair techniques. In this study, we described a novel repair technique developed by the senior author of our study and reported its clinical outcome at 24 months follow-up. Recognizing that the bulk of the insertion area is situated more superiorly, our repair technique emphasizes on reinforcing the superior portion of the tendon providing greater support in the area likely to be under the most strain during contraction of the subscapularis and ensuring good contact between the torn tendon and the footprint.
One of the weaknesses of our study is that majority of the tears are partial (Lafosse grade 1), and so it is not entirely clear whether higher grade tears would yield similar results due to the sparse number of high-grade tears. However, we are of the view that the technique would still be as effective in higher grade tears as the superior portion of the tendon and footprint comprises majority of the contact area and this is the portion of the tendon that our repair technique targets and re-enforces.
The overall outcomes for general shoulder function have been favourable at 24 months post-operatively. It appears that the most improvement was seen in the early post-operative phase between 3 months post-op and 1 year post-op. After which, the improvements seemed to have plateaued. Our study like many others includes cases in which other structures were also repaired (e.g. supraspinatus, labral lesions).
Many of the studies about arthroscopic subscapularis repairs that have been published have shown great improvement in functional and pain scores post-surgery. Lafosse et al. 9 published a prospective study showing improved constant, pain and UCLA scores post-operatively and intact structural integrity with computed tomography arthrography scans in majority of their patients. More recently, Lanz et al. 8 carried out a study with 52 patients (46 available for follow-up) and they too showed an improvement in constant and UCLA scores for their patients. A bigger study (level 3 evidence) carried out by Toussaint et al. 11 involving 208 patients (103 available for follow-up) also showed improvement in Constant and UCLA scores and radiographic evaluation post-operatively showed healing in 92% of cases, although there was some evidence of muscle wasting in 18.6% of cases.
Our repair technique incorporates a configuration similar to a Mason Allen stitch which is then further reinforced with a simple whip stitch to the superior edge of the subscapularis tendon. The configuration providing good contact and reducing the chances of the sutures tearing through the tendon, while the additional whip stitch secures the superior portion of the tendon to the foot print. The suture ends are secured with a second anchor that is placed more laterally.
A number of different surgical techniques have been described for repairing the subscapularis arthroscopically, each with their proposed advantages. Kircher et al. 16 described an ‘interlocking stitch’ technique which is coupled with a vertical mattress suture that gives the advantages of a reduced risk of the suture cutting through the tendon and increasing the contact pressure onto the lesser tuberosity. Saremi 17 described a technique that takes into account ‘interstitial’ tears of the subscapularis tendon which had not been described in the more popularly used classification systems. Parnes et al. 18 described a ‘combined double pulley simple knot’ technique (originally described by Arrigoni et al. 19 ) for repairing the subscapularis that confers the advantage of avoiding excision of healthy tendon and maximizing tendon to bone contact surface area. Denard et al. 20 described a double row fixation that uses a knotless technique that simplifies the repair for tears of the upper portion of the subscapularis. Park et al. 21 also described a ‘suture bridge’ technique involving a double row repair that is effective for tears involving the first facet of the footprint and large tears. Fox et al. 22 did a technique with a series of 18 patients which showed good improvement in outcome scores and minimal complications.
One of the strengths of our study is describing a novel surgical technique for subscapularis repairs which appears to have favourable outcomes. Other strengths include all patients fulfilling a predetermined set of criteria before surgery has been offered as treatment and a single surgeon performed all the surgeries. These reduced the selection bias in our study.
However, there is limitation in our study. Our sample size is small as subscapularis tears are not as common as supraspinatus tears. Nonetheless, our study is adequately powered to detect the MCID of the CMSS and OSS scores.
Conclusion
Our novel technique of arthroscopic subscapularis repair has shown good overall shoulder clinical outcomes in isolated tears and combined rotator cuff tears. We recommend the routine use of this surgical technique in patients with symptomatic subscapularis tears that have failed conservative treatment.
Footnotes
Author note
This study was done at the Singapore General Hospital Department of Orthopaedic Surgery.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.