
Abstract
Background:
Patellofemoral joint chondral lesions (PFCLs) are one of the most common chronic knee problems in all populations in young adults. Despite their high frequency, there is still no consensus about treatment options. All PFCL grades can be treated with surgery, nonoperative treatment, or both.
Purpose/Hypothesis:
The purpose of this study was to compare patients with PFCLs who underwent Fulkerson osteotomy surgery followed by physical therapy and rehabilitation with those patients who only received physical therapy and rehabilitation. It was hypothesized that patients who underwent unilateral Fulkerson osteotomy surgery would have superior results compared with patients who only received nonoperative treatment.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This was a prospective study with a case-control design and included 20 patients who underwent Fulkerson osteotomy and 20 patients with PFCL who were managed nonoperatively. The follow-up period was a median of 13.25 months (range, 12.03-14.71 months) for patients who underwent Fulkerson osteotomy and 12.85 months (range, 12-14.37 months) for patients who were treated nonoperatively. Knee joint position sense and gait kinematics were assessed using the DrGoniometer Application and Zebris FDM-T device. The functional level was determined using the single-leg hop test, the single-leg squat test, and the Kujala subjective knee evaluation form.
Results:
When comparing gait kinematics of the affected sides between patients who underwent Fulkerson osteotomy and those who received nonoperative treatment (physical therapy and rehabilitation only), differences were observed in step length, cadence, stance phase percentage, and swing phase percentage (P < .05). In knee joint position sense of the affected sides at 60° target angle, patients who underwent Fulkerson osteotomy had significant improvements after surgery (P < .05), whereas patients who were managed nonoperatively showed continued impairment both before and after treatment (P < .05). No significant differences were observed in single-leg hop and single-leg squat test results between the 2 groups (P > .05). Kujala scores were significantly higher in the Fulkerson osteotomy group (89.79 ± 12.67 vs 80.10 ± 13.20, respectively) (P < .05).
Conclusion:
Patients who underwent Fulkerson osteotomy had superior gait kinematics, joint position sense at 60° of flexion, and Kujala scores. No significant changes were observed in terms of the joint position sense at 15°, 45°, and 90° of flexion, the single-leg hop test, and the single-leg squat test compared with those who received nonoperative treatment.
Introduction
Patellofemoral joint chondral lesions (PFCLs) are one of the most common knee problems in all populations and are particularly prevalent as a cause of chronic knee pain in young adults.11,15,22,23,39 Despite its frequency, debates about their pathogenesis and treatment continue.1,34 PFCLs are characterized by anterior knee pain within a histopathological spectrum that ranges from softening and minimal degeneration of the patellar cartilage to the formation of large ulcerative areas.33,46 Functional impairments and changes in lower extremity biomechanics may occur at the end-stages of the PFCL3,43 (magnetic resonance imaging [MRI]—Modified Outerbridge stages 3-4).
Malalignment of the patellofemoral joint predisposes to instability, anterior knee pain, chondropathy, and arthrosis. 12 While malalignment in the patellofemoral joint is initially attempted to be treated nonoperatively, surgical interventions may be necessary when nonoperative methods fail. Various surgical techniques have been proposed for the treatment of patellofemoral instability and chondropathy/arthrosis—including lateral release, medial reefing, medial patellofemoral ligament reconstruction, patellofemoral arthroplasty, and Fulkerson osteotomy.21,25,31
Patellar maltracking can lead to proprioceptive loss by damaging the peripatellar proprioceptive plexus endings. 1 Fulkerson osteotomy is one of the preferred surgical methods for solving patellofemoral problems caused by patellofemoral malalignment, as it can restore the patellar alignment and decrease the patellofemoral contact force.13,41,46 Fulkerson anteromedial tibial tubercle transfer can be performed for patellofemoral pain, patellar maltracking, and instability.13,41 After surgery, patellofemoral contact force improves, positively affecting lower extremity alignment. 45
Fulkerson osteotomy has the advantage of lowering pressure on patellofemoral forces with an anteriorization component and addresses mechanical alignment issues with the medialization component. This combined anteromedialization process most effectively transfers the loads on the distal and lateral aspects of the patella to the more proximal and medial cartilage. Previous studies demonstrated that Fulkerson osteotomy is a valuable option, especially for active and elderly patients with PFCLs. 8
We hypothesized that patients who underwent unilateral Fulkerson osteotomy surgery would have superior results compared with patients who only received nonoperative treatment in terms of knee joint position sense, gait kinematics, and functional level.
In this study, we aimed to compare knee joint position sense, gait kinematics, and functional levels of patients who underwent Fulkerson osteotomy for unilateral PFCL associated with cartilage damage, followed by physical therapy and rehabilitation, with those who only received physical therapy and rehabilitation.
Methods
This study was approved by Uskudar University Clinical Research Ethics Committee (May 4, 2020, Decision No. 61351342/2020-211). Participants were provided with detailed information about the purpose and assessment methods of the study. Informed consent forms were signed by those who agreed to participate in the study. This study was not funded by any company or individual.
This was a prospective study with a case-control design, which was conducted at a single center to compare knee joint position sense, gait kinematics, and functional levels of patients who underwent Fulkerson osteotomy, followed by physical therapy and rehabilitation, with those who only received physical therapy and rehabilitation. Operative and nonoperative treatments were conducted between October 2020 and March 2021.
Patients with anterior knee pain were evaluated clinically and radiologically. MRI was used to evaluate the cartilage pathology using the Modified Outerbridge Classification 35 (Table 1). A total of 112 patients diagnosed with grade 3 or 4 PFCLs were included in our study (Figure 1). A treatment algorithm with an 8-week physical therapy program was offered for all patients. Operative treatment was offered to the patients with no or poor clinical improvement after physical therapy. A total of 20 patients underwent Fulkerson osteotomy, and all patients were included in our study. All operatively treated patients had a body mass index (BMI) of <35 kg/m2, no concomitant preoperative pathology or major surgical complications, and no loss to follow-up. A total of 92 patients were provided with physical therapy only. A total of 37 patients were lost to follow-up. The remaining 16 patients had a BMI of >35 kg/m2 and were excluded from the study. A simple coin-flipping randomization was made among the remaining 39 patients to reduce their number to 20 patients to compare the 2 groups in a 1 to 1 ratio.
Modified Outerbridge Classification With FS PD MRI a
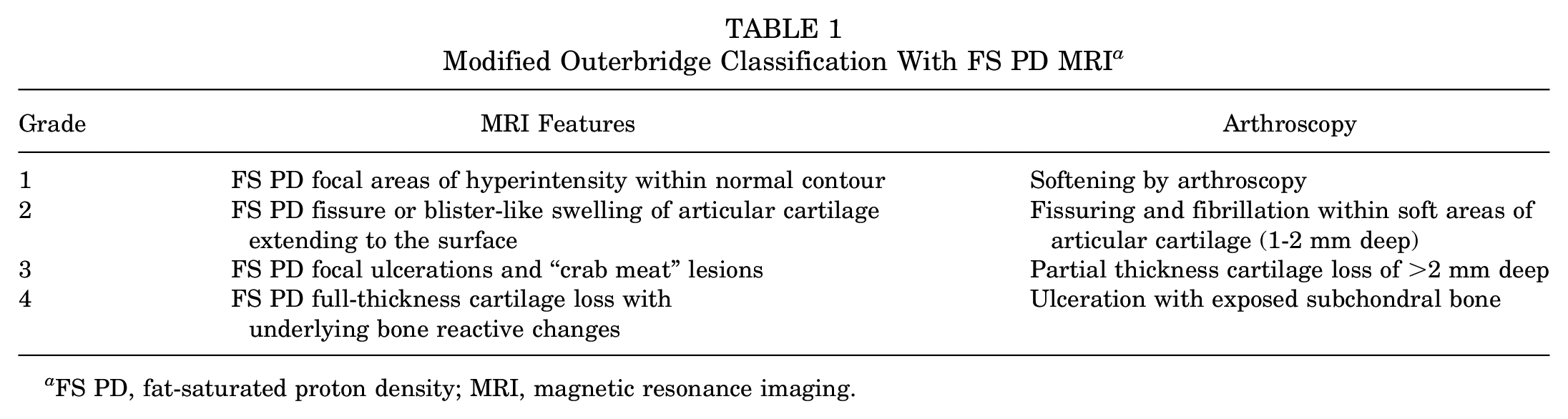
FS PD, fat-saturated proton density; MRI, magnetic resonance imaging.
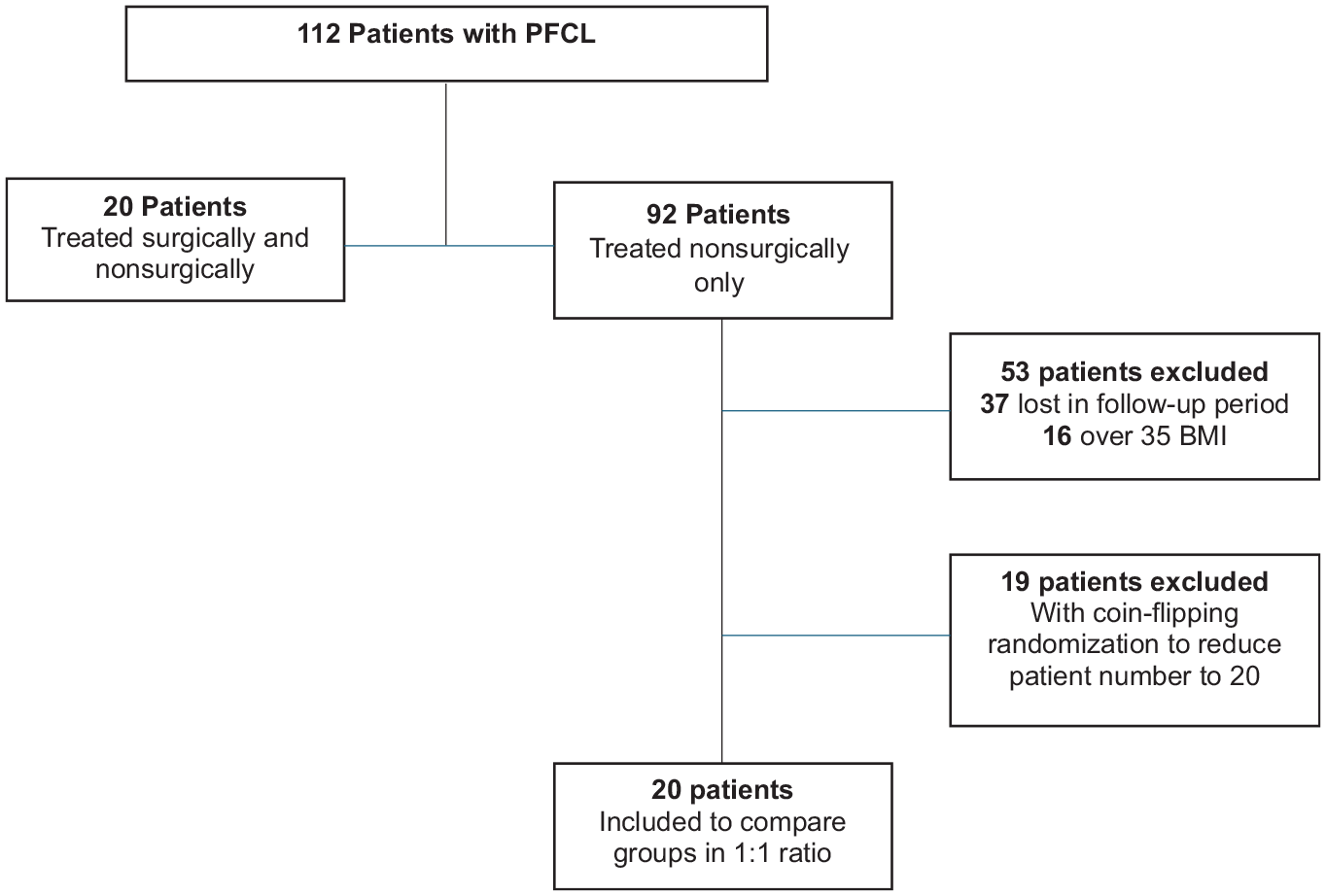
Flowchart of the patients. BMI, body mass index; PFCL, patellofemoral joint chondral lesion.
Patients were divided into 2 groups: (1) The operative group consisted of patients who had unilateral Fulkerson osteotomy followed by physical therapy and rehabilitation; (2) the nonoperative group included patients who only received physical therapy and rehabilitation. A total of 40 patients were included in the study. There was a 1-year follow-up period for patients after surgery in the operative group and a 1-year follow-up period after initiation of physical therapy in the nonoperative group. All patients’ operative and nonoperative treatments were performed by the same surgeon (T.B.) and the same physical therapist team (F.B.Y.).
Patients having patellar subluxation or dislocation, inflammatory processes in the knee, a history of previous surgeries, concomitant ligament tears, diffuse knee arthritis, and bilateral Fulkerson osteotomy were excluded from this study.
Both groups underwent the same physical therapy program conducted by the physical therapist team. Physical therapy and rehabilitation sessions were conducted 3 times a week for 3 months. Home exercises were assigned to strengthen the knee, hip, and ankle using isometric and isotonic exercises, as well as balance proprioception exercises (15 repetitions × 3 sets). The physical therapy program for the patients was as follows:
Pneumatic cold compression (15 min)
Magnetotherapy (20 min)
Intermittent negative pressure therapy (30 min)
Neuromuscular electrical simulation (15 min)
Soft tissue and joint mobilization (5 min)
Isometric knee, hip, and ankle strengthening exercises (15 reps × 3 sets)
Isotonic knee, hip, and ankle strengthening exercises (15 reps × 3 sets)
Balance-coordination and proprioception exercises (15 reps × 3 sets)
Use of custom-made insoles
Evaluation of Gait Kinematics
The Zebris instrumented gait analysis system (FDM-T; Zebris Medical GmbH) was used to obtain numerical data for kinetic and kinematic gait parameters. Zebris Treadmill provides clinicians a sensitive system to detect changes in spatiotemporal gait parameters and vertical ground-reaction forces. 37 The assessed main spatial-temporal parameters were as follows:
Foot rotation (deg)
Step length (cm)
Cadence (steps/min)
Stance phase (%)
Swing phase (%)
Step width (cm)
Step duration
The evaluation was conducted on a treadmill starting from a fixed speed of 0.5 km/h, gradually increasing by 0.3 km/h every 10 seconds until reaching 5 km/h. Measurements were recorded during 30 seconds at 5 km/h (Figure 2).

Gait kinematics evaluation with the Zebris FDM treadmill.
Evaluation of Knee Joint Position Sense
The DrGoniometer mobile application (DrG) (CDM Srl) was used for evaluating knee joint position sense, which has been shown to have high accuracy and reliability compared with universal goniometers.9,10 Participants were blindfolded and positioned on a standard back-supported chair with their hips and knees at 90° of flexion. They were asked to find the target angles of 15°, 45°, and 60° in the sagittal plane. Participants verbally indicated when they thought they reached the target angle, and an image was captured using the DrG mobile application for angle measurement (Figure 3). Every target angle was repeated 6 times for each patient, and the mean of the 6 repetitions’ degrees was noted. Deviations of up to 5° from the target angle were considered normal, while deviations exceeding this threshold were deemed "pathological," indicating proprioceptive loss.

Angle measurement position and using the DrG application on a mobile phone.
Evaluation of Functional Levels
Participants’ lower extremity functional and physical performance was evaluated through single-leg hopping and single-leg squat tests.
In the single-leg squat test, participants were asked to stand on a “T” mark on the floor maintaining a straight posture with a single-leg stance, with the other knee flexed to 90°, squatting down with the body in a straight position until they could not see the line in front of them (∼45°-60° of flexion) (Figure 4). The test was repeated 3 times and considered successful if the patient properly completed the requested steps at least once. 27

The single-leg squat test is performed with the following postures: (A) straight (A) and (B) squatting down.
In the single-leg hop test, participants were instructed to jump forward as far as possible on 1 leg and pause for 2 to 3 seconds after the jump. The distance (cm) between the tip of the toe in the initial and landing positions was measured17,32 (Figure 5).

The single-leg hop test with (A) a straight posture and (B) after a hopping posture.
Evaluation of Functional Level With Scoring System
The Kujala patellofemoral score, developed by Kujala et al, 24 consists of 13 questions (Figure 6). The scoring system ranges from 0 to 100 points, with higher scores indicating better function. The questions included in the scoring were read to the participants, and the answers were recorded.
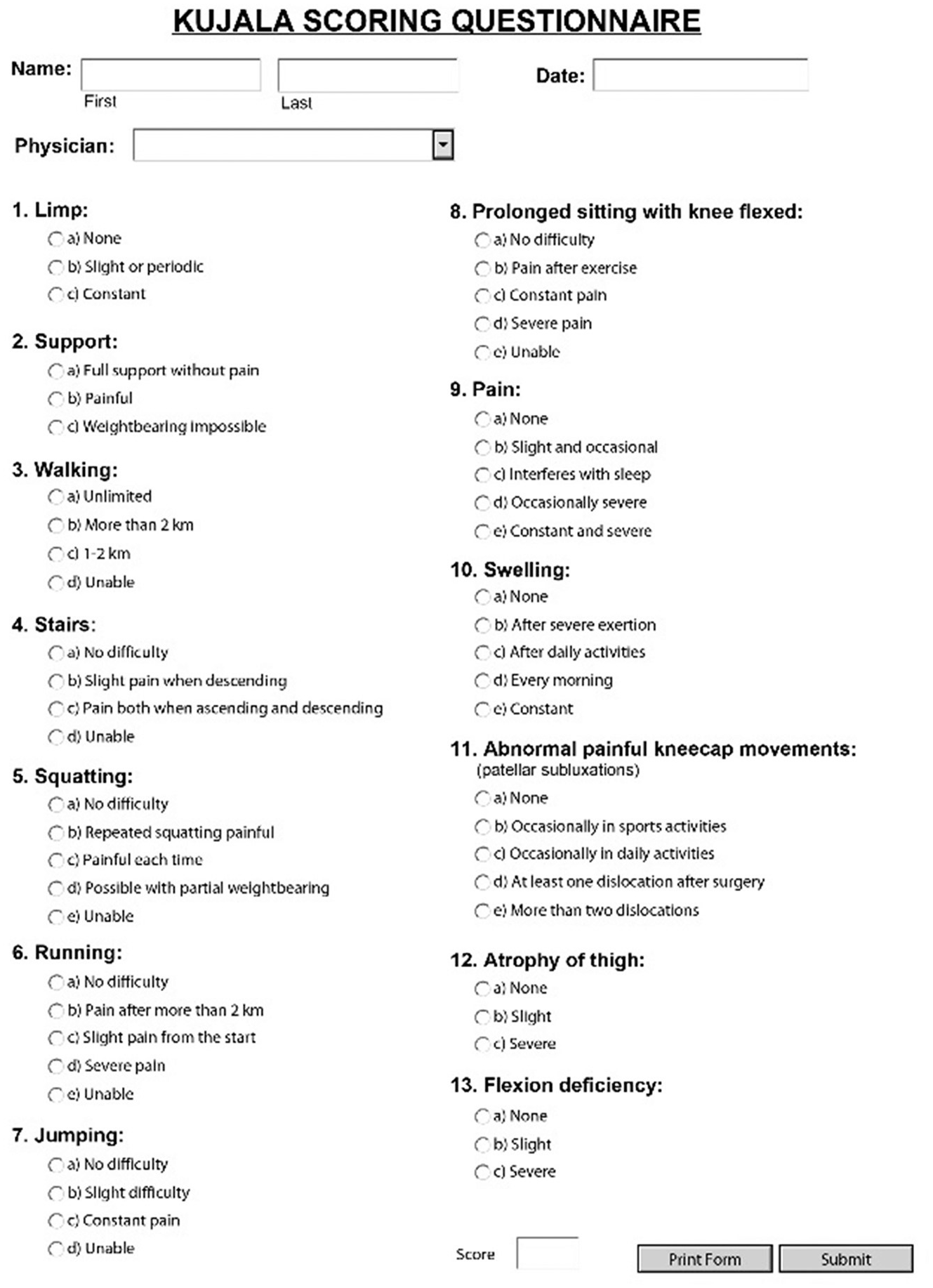
The Kujala Scoring Questionnaire.
Statistical Analysis
Statistical analyses were performed using SPSS Version 17.0 (IBM). Normal distribution of variables was assessed through histograms and the Kolmogorov-Smirnov test. Descriptive analyses were presented using the mean, standard deviation, and median values. Categorical variables were compared using the Pearson chi-square test. Nonparametric values were evaluated using the Mann-Whitney U test. Within-group changes were analyzed using the Wilcoxon test, while between-group changes were examined using the repeated measures analysis of variance. Changes in categorical variables were analyzed using the McNemar test. P < .05 was considered statistically significant.
Results
A total of 40 patients were included in the study and were divided into 2 groups: (1) those who underwent unilateral Fulkerson osteotomy, followed by physical therapy and rehabilitation (operative group); (2) those who only received physical therapy and rehabilitation (nonoperative group).
Comparison of baseline characteristics between the operative and nonoperative groups revealed no significant differences in terms of sex, dominant side, affected side, age, BMI, and time elapsed after treatment (P > .05) (Table 2).
Patient Characteristics a
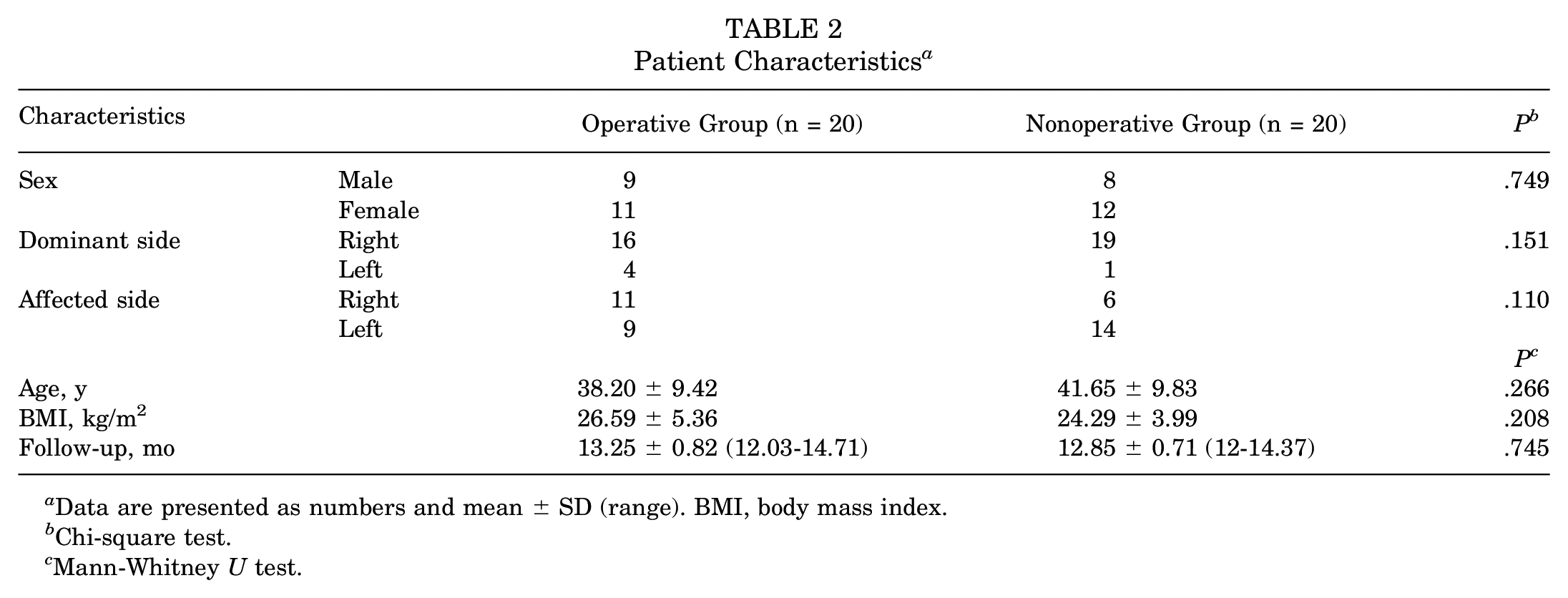
Data are presented as numbers and mean ± SD (range). BMI, body mass index.
Chi-square test.
Mann-Whitney U test.
Comparison of Gait Kinematics Results
Two methods were used to compare the gait kinematics data. First, pre- and posttreatment measures were compared within the group. Second, pre- and posttreatment comparisons were made between the 2 groups.
In the operative group, the posttreatment step length, cadence, and stance phase demonstrated a significant increase compared with pretreatment values (P < .05). Moreover, the duration of posttreatment swing phase decreased significantly (P < .05) (Table 3).
Comparison of Gate Kinematics Between Groups a

Data are presented as mean ± SD unless otherwise indicated.
Wilcoxon test. P b indicates changes before and after treatment in the same group of patients.
Mann-Whitney U test. P c indicates whether there is an intergroup difference before and after treatment.
In the nonoperative group, there were no significant differences in step length, stance phase, swing phase, and cadence values between pre- and posttreatment measures (P > .05) (Table 3).
Between-group comparisons revealed that the posttreatment step length, cadence, stance phase, and swing phase kinematics favored the operative group with significant differences (P < .05) (Table 3).
Comparison of Knee Joint Position Sense Results
In the operative group, comparisons were made between values of the knee joint position sense at 15°, 45°, and 60° target angles before and after treatment, and no significant differences were found in terms of values (P > .05) (Table 4). Using a value of 5°error as the threshold for abnormal proprioception, it was observed that proprioception was pathologically impaired at the 60° target angle in the operative group before treatment, while it was not pathologically impaired after treatment.
Comparison of Knee Joint Position Sense at 15°, 45-, and 60° Between Groups a

Data are presented as mean ± SD.
Wilcoxon test. P b indicates changes in the same group of patients before and after treatment.
Mann-Whitney U test. P c indicates whether there is an intergroup difference pre- or posttreatment. The values represent the patients’ sense of where they think their knee is in the target angle position, and the mean values of the result of the 6-repetition were noted.
In the nonoperative group, comparisons were made between values of knee joint position sense at 15°, 45°, and 60° target angles before and after treatment. No significant differences were found (P > .05). Pathological proprioception was observed in the pre- and posttreatment 60° target angle in the nonoperative group.
Between-group comparisons of values of knee joint position sense at 15°, 45°, and 60° target angles revealed no significant differences (P > .05) (Table 4). Comparing the pretreatment values of both groups in terms of deviation, it was found that they both had more deviation at the 60° target angle than at the 5° threshold, indicating pathological proprioception. However, unlike the nonoperative group, the operative group did not exhibit a loss of proprioception at the posttreatment 60° target angle.
Comparison of Functional Level Results
Both groups exhibited statistically significant increases in single-leg hop distance scores and Kujala scores when comparing the pre- and posttreatment values (P < .05) (Table 5). No significant differences were observed between the 2 groups in terms of posttreatment single-leg hop distance scores (P > .05); however, the operative group had higher Kujala scores than the nonoperative group (P < .05) (Table 5).
Comparison of Kujala Scores and Single-Leg Hop Results Between Groups a
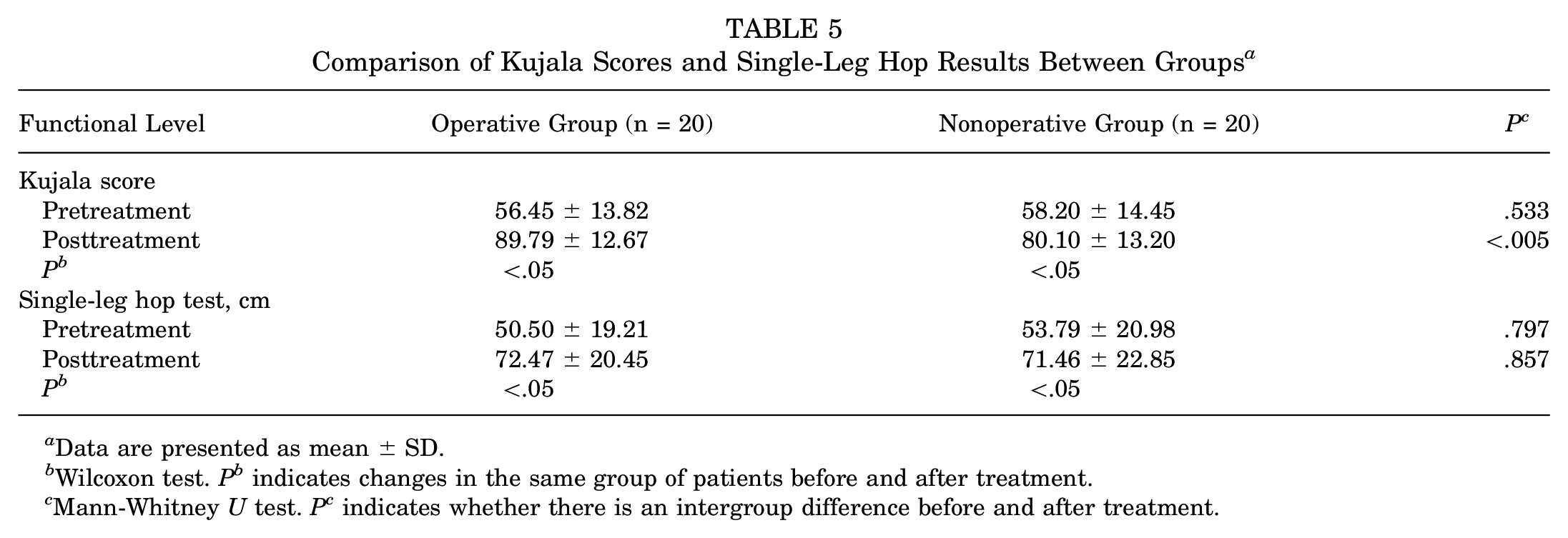
Data are presented as mean ± SD.
Wilcoxon test. P b indicates changes in the same group of patients before and after treatment.
Mann-Whitney U test. P c indicates whether there is an intergroup difference before and after treatment.
Both groups showed increased single-leg squat performance after treatment compared with before treatment (P < .05). There was no significant difference in single-leg squat performance between the groups (P > .05) (Table 6).
Comparison of Single-Leg Squat Results Between Groups

Mc-Nemar test.
Chi-square test.
Discussion
We evaluated target angles as commonly used in daily life and sports activities. Although no significant differences were found between pre- and posttreatment measures within and between groups regarding values of the knee joint position sense at 15°, 45°, and 60° target angles, it was observed that in the operative group, the mean deviation of >5° from the 60° target angle, which was considered pathological preoperatively, entered the range of nonpathological values postoperatively. In the nonoperative group, on the other hand, both pre- and posttreatment values had >a 5° deviation from the 60° target angle and were considered pathological.
Knee joint position sense is the most widely used measure of proprioceptive ability in the literature.14,19,42 Studies have reported that measurements of knee joint position sense at 20° and 60° in patellofemoral pain patients, whether performed actively or passively, with 5 repetitions, yield valuable results.18,40 Various equipment types—including electrogoniometers and dynamometers—can be used to measure knee joint position sense, and smartphone applications have also become popular; in our study, measurements were conducted using the DrGoniometer application.9,38,42
The literature review revealed conflicting results regarding knee joint position sense in patients with PFCLs. Some studies demonstrated no significant difference in joint position sense perception between patients with and without PFCLs.6,29,48 Other studies indicated that knee joint position sense was more affected in patients with PFCLs.1,2,4,16 A study by Akseki et al 1 suggested that peripatellar proprioceptive plexus terminations could be damaged due to abnormal patellar positioning, leading to proprioceptive loss. Previous studies evaluating the normal limits of proprioceptive sense have deemed deviations of >5° from the target angle as abnormal. 36
Instrumented treadmills can be used to assess walking parameters. 20 The Zebris FDM-THQ (Zebris Medical GmbH) was used in our study, which has been shown 44 to have a maximum error rate of 5.4%. Studies have reported increased hip adduction, decreased passive hip range of motion, decreased knee flexion angle, delayed peak rearfoot eversion, and shorter step length in patients with PFCLs during walking.5,7,47
In the operative group, posttreatment results showed an increase in step length and cadence, leading to an increase in stance phase duration. In the nonoperative group, the posttreatment step length, cadence, and stance phase percentage increased, but these increases were not statistically significant. Our study found that patients who underwent Fulkerson osteotomy had superior walking kinematics compared with the nonoperatively followed group. This difference is thought to stem from the anatomic correction of patellar alignment in the Fulkerson osteotomy group, which positively affected lower extremity alignment.
The literature suggests that PFCL affects functionality and that compromised knee strength is a risk factor. 30 Increased ipsilateral trunk weakness, contralateral pelvic drop, hip adduction, and deviations in knee position have been observed during single-leg squats.26,28 In our study, the functional levels of the affected sides in both groups were evaluated with single-leg hopping and single-leg squat tests. In both groups, posttreatment hopping distances increased significantly, and single-leg squat percentages improved. However, the operative group showed significantly better Kujala scores than the nonoperative group in posttreatment single-leg hopping. The similarity in the results of single-leg squat and single-leg hopping tests may stem from both groups consisting of sedentary individuals and following the same physical therapy and rehabilitation protocols.
There are limitations to our study. This study was conducted with a limited number of patients, and the minimum follow-up period of this study was only 1 year. Longer periods of follow-up may demonstrate how the operative or nonoperative options alter patients’ contact mechanics and progression to osteoarthritis. In addition, there was a high rate of loss to follow-up in the nonoperative group. Patients with better outcomes in the nonoperative group may be lost to follow-up, which may result in a potential selection bias. Also, the DrGoniometer application may have inaccurate results in obese patients, which may limit the precise angle measurement and alter the result of this study.
Conclusion
In this study, the operatively treated group exhibited better results in terms of gait kinematics, joint position sense at 60° of flexion, and Kujala scores. However, this study found no significant change in terms of the joint position sense at 15°, 45°, and 90° of flexion; the single-leg hop test; and the single-leg squat test between the operatively treated group and the nonoperatively treated group. We believe that the improvement in proprioception of those who underwent Fulkerson osteotomy is associated with the anatomic realignment of the knee. Our study could provide insights into the treatment of pain, limited mobility, and functional levels resulting from patellofemoral joint pathologies.
Footnotes
Final revision submitted November 10, 2024; accepted December 16, 2024.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Uskudar Universitesi (61351342/2020-211).