
Abstract
Background:
Peripheral tears of complete discoid lateral meniscus (DLM) display a wide spectrum of clinical manifestations. However, a staging system for such tears has not yet been established.
Purpose:
To determine whether there is a progression in the pattern of peripheral tears in complete DLM and establish a comprehensive staging system that categorizes these tears into distinct stages.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A consecutive series of 298 knees diagnosed with complete DLM between July 2006 and December 2022 were retrospectively reviewed. A staging system based on clinical symptoms, presence of tears on magnetic resonance imaging (MRI), and stability during arthroscopic examination was used to classify patients into seven stages (stage 0–6). Patient demographic data and International Cartilage Regeneration & Joint Preservation Society (ICRS) grade on MRI were assessed.
Results:
A total of 18 knees were classified as stage 0, 27 as stage 1, 46 as stage 2, 51 as stage 3, 22 as stage 4, 122 as stage 5, and 12 as stage 6. Each stage was defined by characteristic clinical features. A higher ICRS cartilage grade in both the lateral femoral condyle (Spearman coefficient, r = 0.893) and the lateral tibial plateau (r = 0.929) were correlated with an increase in stage.
Conclusion:
Progressive stages characterize the development of peripheral tears in a complete DLM. Higher stages are associated with more severe displacement of tears and increased cartilage degeneration.
The discoid lateral meniscus (DLM) is a congenital anomaly of the knee with an estimated incidence of 0.4% to 17%,7,8,10,20,23 but the true prevalence remains elusive because of the condition’s often asymptomatic nature and a wide spectrum of pathomorphological variations.11,12 This heterogeneity, ranging from asymptomatic DLM with minimal deviations in shape and stable peripheral capsular attachments to symptomatic DLM with marked alterations in dimensions and absent capsular attachments, challenges the traditional methods of description and classification.2,16
Previous studies have highlighted the significant variability in DLM morphology, peripheral attachment, and stability.6,14,20,23 While multiple classification systems for DLM have been established based on arthroscopic appearance, peripheral rim instability, presence of tears, and direction of shift, none has outlined any staged or temporal relationship among DLM tears.1,6,9,14 Even though the presence of peripheral tears in DLM has been extensively documented, their pathogenesis and trajectory remain obscure12,24 The absence of a standardized staging system has hindered our ability to understand the natural history of these tears and determine the most appropriate course of intervention (Figure 1).

Right knee magnetic resonance imaging (MRI) of 32-year-old female patient. (A, B) Complete discoid lateral meniscus is seen without associated tear, but hiatus widening is visible. Patient was asymptomatic on the right knee. (C, D) Right knee MRI of same patient taken 7 years later. Patient complained of knee pain and swelling. Peripheral tear is visible, but patient did not receive treatment. (E, F) Right knee MRI of same patient 6 months later. Tear has progressed and is seen displaced into the intercondylar notch.
The purpose of this study was to ascertain whether there is a pattern of progression in peripheral tears of complete DLM (CDLM) and to establish a comprehensive staging system that categorizes these tears into distinct stages. Additionally, the potential clinical and prognostic implications associated with the temporal evolution of peripheral tears in CDLM was investigated.
Methods
Patient Selection
The medical records and radiographic studies of 903 consecutive patients (1038 knees) diagnosed with DLM at a tertiary hospital between July 2006 and December 2022 were retrospectively reviewed. Diagnosis of DLM was based on physical examination and magnetic resonance imaging (MRI) findings. Data collected included age at time of diagnosis, gender, laterality, presence of symptoms, type of DLM, presence of meniscal tear, type of meniscal tear, meniscal stability, and cartilage status of the lateral femoral condyle (LFC) and lateral tibial plateau (LTP). Tear pattern was classified as peripheral tear, horizontal tear, radial tear, and flap tear. Meniscal stability was determined based on direct examination during arthroscopy; the meniscus was deemed unstable if there was evidence of hypermobility upon probing or if there was peripheral detachment. After excluding knees with incomplete DLM (n = 516) and nonperipheral tears (n = 224), 252 patients (298 knees) were included in the final analysis. This study was approved by the institutional review board of our hospital.
Patient Stratification and Staging
The proposed staging system was developed after a comprehensive review of all the available clinical and radiographic data to determine distinct features and key characteristics that would define each stage. According to the presence of a palpable or subjective clunk on physical examination, type of meniscal tear on MRI, and stability during arthroscopic examination, patients were classified into 7 stages. Each stage had a characteristic defining feature, which we described as a "hallmark" finding, and is detailed in the bottom row of Table 1.
Staging System of Complete Discoid Lateral Meniscus Peripheral Tears a

MRI, magnetic resonance imaging; OA, osteoarthritis.
− : no clunk, + : clunk ; ± : equivocal finding.
The rationale for having 3 components in the staging system was to compensate for the limitations inherent in each evaluation method. MRI alone may be insufficient to diagnose peripheral tears, as a meniscus with peripheral instability may be reduced at the time when MRI is performed. Thus, a careful physical examination to detect the presence of a palpable clunk during range of motion provides valuable information. Additionally, even though arthroscopy may be considered the most direct method for visualization of intra-articular pathology, the limited field of vision of arthroscopic instruments and the bulky and deformed anatomy of the discoid meniscus may make complete delineation of the meniscus infeasible. Thus, all the previously mentioned methods of evaluation should be considered together for a holistic diagnostic approach.

Stage 0: right knee of 38-year-old female patient. (A) Complete discoid lateral meniscus (CDLM) was incidentally discovered on magnetic resonance imaging taken for suspected medial meniscal (MM) tear. The patient had no lateral symptoms. (B, C, D) Arthroscopic examination of the lateral compartment was performed during surgery for MM horizontal tear, and CDLM was stable in all directions upon probing.

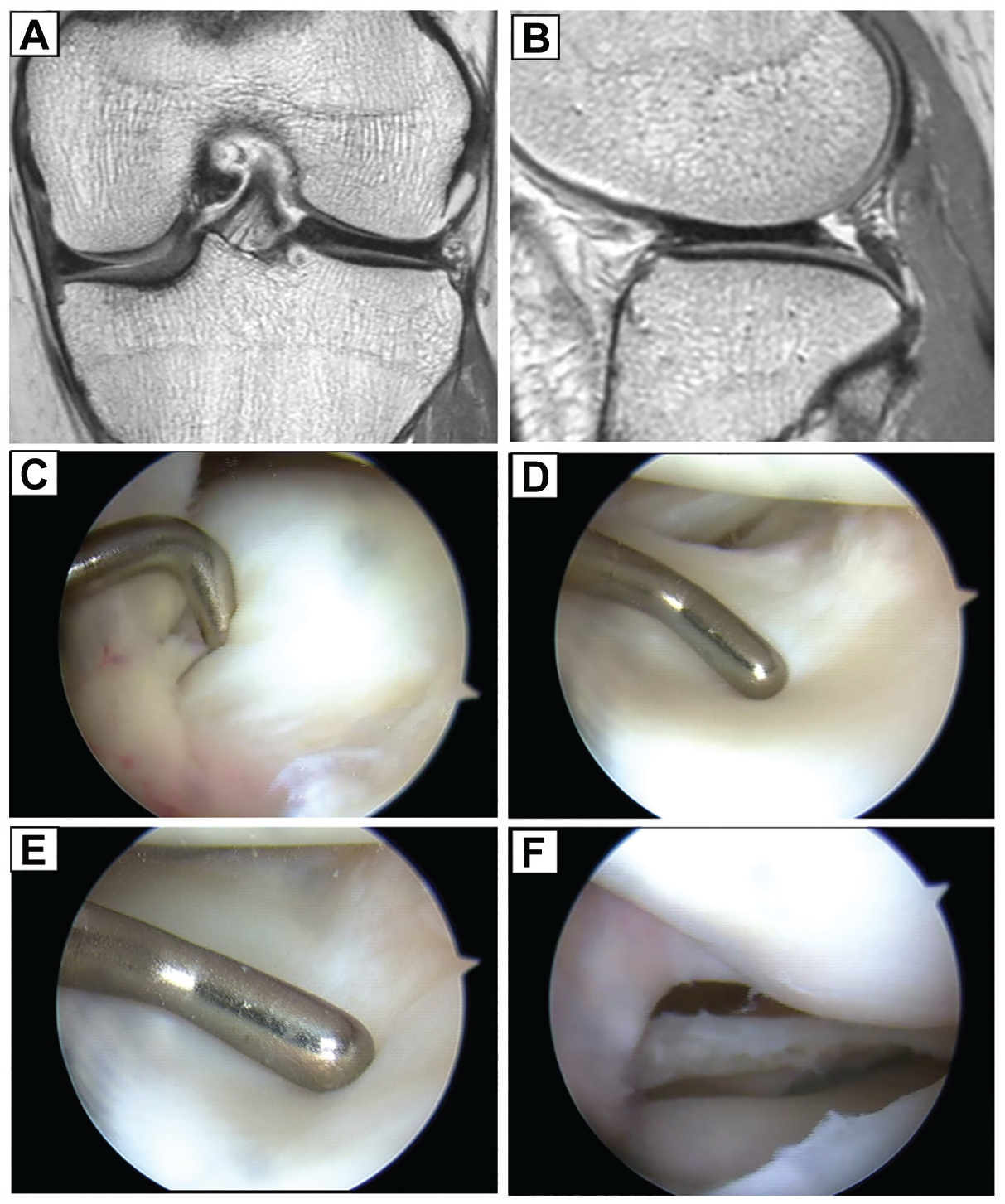
Stage 1: right knee of 49-year-old female patient. (A) No tear was visible on magnetic resonance imaging (MRI), but the patient complained of intermittent lateral knee pain, which worsened during squatting. (B) Slight forward slanting of the meniscus with subtle widening of the popliteal hiatus is noted on MRI sagittal image. (C, D, E) Arthroscopic examination showed complete discoid lateral meniscus with a stable peripheral rim. (F) Partial central meniscectomy was performed.
Stage 2: left knee of 21-year-old female patient. Physical examination revealed demonstrable clunk during range of motion. (A, B) Magnetic resonance imaging (MRI) shows peripheral thinning on coronal images and mass shifting anteriorly on sagittal sequence, but no definite tear. (C, D, E) Arthroscopic examination showed friable peripheral tissue, which proved unstable upon probing. (F) Partial meniscectomy and rim stabilization with repair were done.
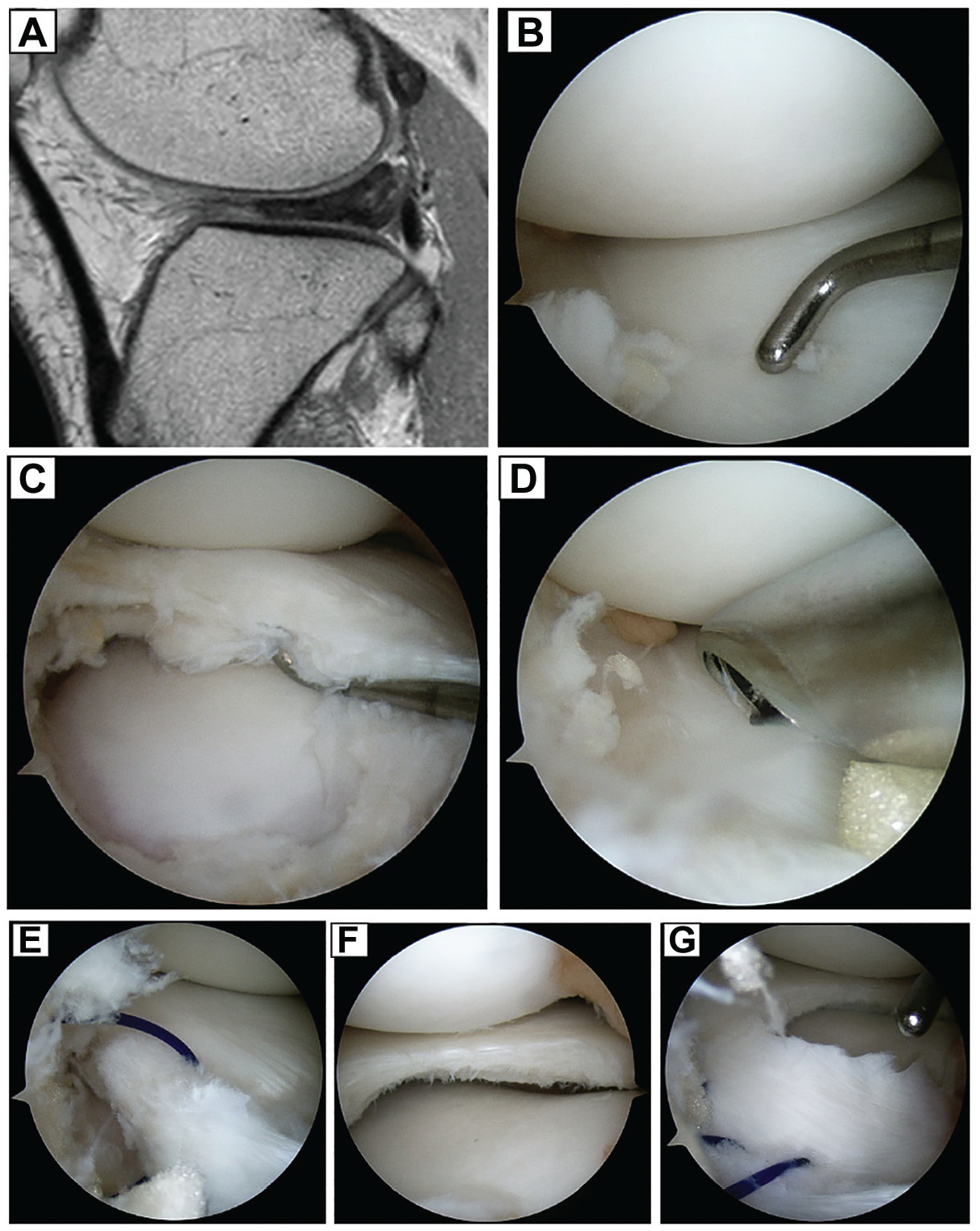
Stage 2: right knee of 15-year-old female patient. Physical examination revealed demonstrable clunk during range of motion. (A) MRI shows mass shifting posteriorly on sagittal sequence, but no definite tear. (B, C, D) Arthroscopic examination showed flimsy and non-functional peripheral tissue around the anterior horn, which collapsed after minimal debridement, revealing substantial instability. (E, F, G) Traction suture was placed, and partial meniscectomy followed by rim stabilization with repair was done.
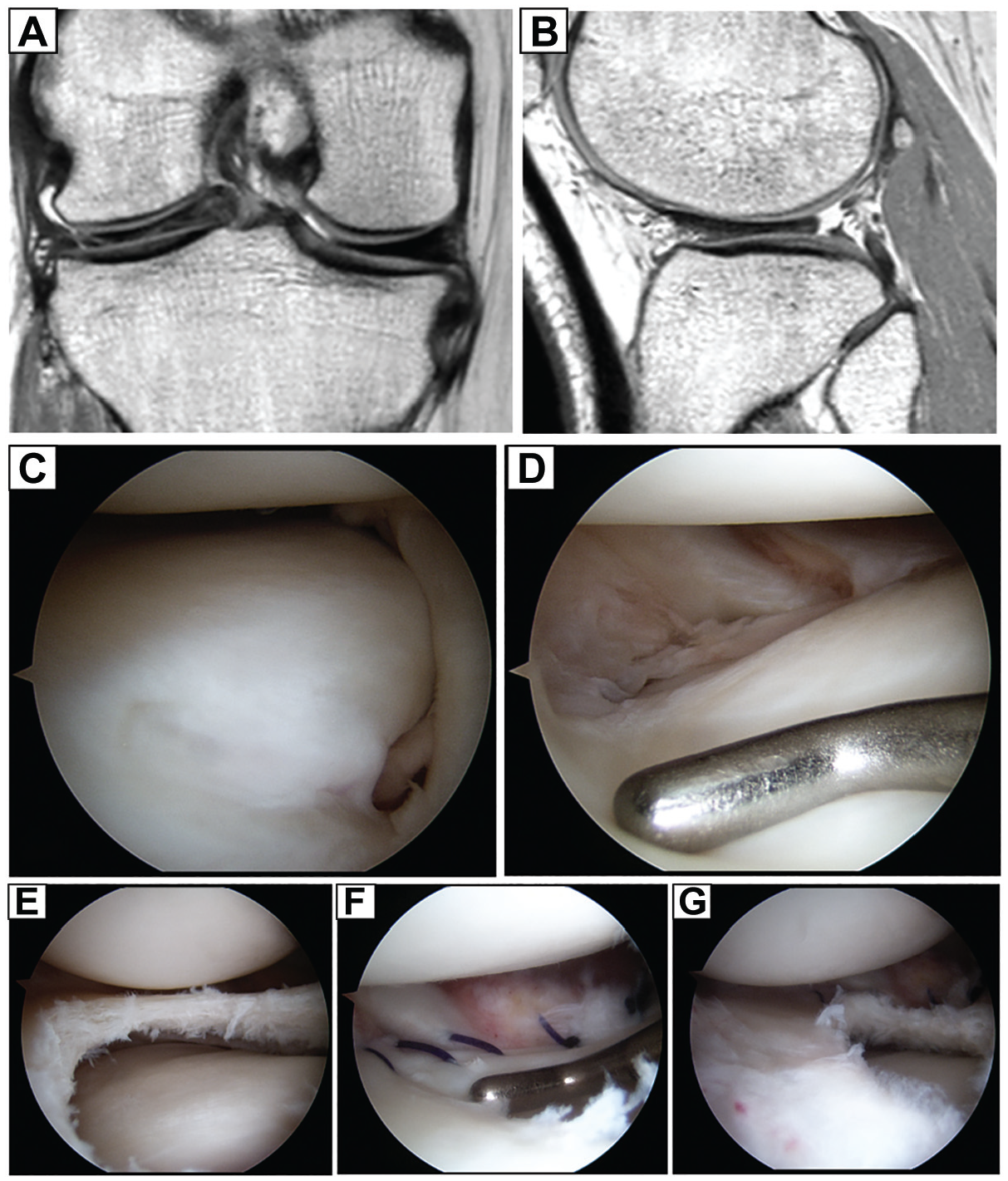
Stage 3: right knee of 37-year-old female patient. (A, B) Magnetic resonance imaging (MRI) showed a peripheral tear at the posterolateral corner. (C, D) The corresponding tear was unstable upon arthroscopic probing. (E, F, G) Treatment consisted of partial meniscectomy and repair.

Stage 4: left knee of 7-year-old female patient. (A) Magnetic resonance imaging (MRI) coronal sequence shows a lateral discoid meniscus completely translocated tear displaced into the intercondylar notch. (B, C, D) The displaced fragment was amenable to reduction using sutures. (E, F) Partial central meniscectomy was performed, followed by meniscocapsular repair.

Stage 5: left knee of 50-year-old female patient. (A) A completely translocated tear of complete lateral discoid meniscus is visible on magnetic resonance imaging coronal sequence. (B) The thick, blunt edge of the displaced fragment is highly suggestive of CDLM tear – shown by a white arrowhead on panel (A) and by a black arrowhead on panel (B). Arthroscopic examination revealed the extent of the tear, which was deemed irreducible and irreparable. (C, D) Severe cartilage degeneration of both the lateral femoral condyle and the lateral tibial plateau was noted. Total meniscectomy was reluctantly performed.

Stage 6: right knee of 62-year-old female patient. Mild intermittent knee pain had persisted for 4 years. The patient was able to walk for 2 to 3 hours without pain. On physical examination, there was no effusion, no locking, and no joint line tenderness, with full range of motion possible. (A) Magnetic resonance imaging showed a chronic translocated and fixed tear of discoid lateral meniscus that appeared to be stable, achieving “secondary congruency.” (B, C) Notably, full-length hip-knee-ankle weightbearing anteroposterior radiographs show the patient having varus alignment, not valgus as typically seen in lateral compartment osteoarthritis. Symptoms resolved with activity modification.
Assessment of Cartilage Status
The cartilage status of the LFC and LTP were assessed on preoperative MRI using the International Cartilage Regeneration & Joint Preservation Society (ICRS) grading system. Both coronal and sagittal sequences were evaluated, and the worst area of the cartilage defect was assumed to represent the entire grade of the LFC or LTP.
Statistical Analysis
Two board-certified orthopaedic surgeons specializing in knee surgery (H.Y.K., J.J.R.) separately reviewed the data of 298 knees, blinded to each other’s results. Each case was categorized using the proposed staging system. The process was repeated after a 2-month interval. Intraobserver reproducibility and interobserver reliability regarding staging were assessed using kappa statistics to measure agreement among observers. As there were 2 observers and the data involved categorical classification, Cohen kappa coefficient was used. The results were interpreted according to the guidelines described by Landis and Koch 15 as follows: <0 indicating no agreement, 0 to 0.20 as slight agreement, 0.21 to 0.40 as fair agreement, 0.41 to 0.60 as moderate agreement, 0.61 to 0.80 as substantial agreement, and 0.81 to 1 as almost perfect agreement.
Statistical analysis was also performed to investigate the correlation between stage and cartilage status of the LFC and LTP using Spearman correlation analysis. To evaluate the inter- and intraobserver reliability of cartilage status assessment, 50 knees were selected randomly and the ICRS grade of the LFC and LTP were also measured by the 2 observers at an interval of 2 months. The intraclass correlation coefficient was then calculated. Data analysis was carried out using the Statistical Package for the Social Sciences (SPSS) software (SPSS Statistics for Windows, Version 21.0; IBM Corp) and SAS software Version 9.2 (SAS Institute Inc).
Results
The 252 patients (298 knees) had a mean age of 33.7 ± 19.1 years (range, 5-76 years) at the time of diagnosis. There were 79 male (31.3%) and 173 female (68.7%) patients, with 154 right (51.7%) and 144 left (48.3%) knees.
The knees were classified as follows, according to the proposed staging criteria: 18 knees as stage 0, 27 knees as stage 1, 46 knees as stage 2, 51 knees as stage 3, 22 knees as stage 4, 122 knees as stage 5, and 12 knees as stage 6 (Table 2).
Patient Demographics and ICRS Grade by Stage a

Values are presented as n unless otherwise indicated. ICRS, International Cartilage Regeneration & Joint Preservation Society; LFC, lateral femoral condyle; LTP, lateral tibial plateau.
The correlation between an increase in stage and a higher ICRS cartilage grade was significant for both the LFC (Spearman coefficient: r = 0.893; P < .01) and LTP (r = 0.929; P < .01). Thus, higher stages were defined by greater severity of cartilage wear. The intraclass correlation coefficient of inter- and intraobserver reliability were >0.90 for the measurements of cartilage status assessment, indicating high reliability. Although later stages had a trend of increasing age, correlation between stage and age at time of diagnosis was not significant.
With respect to staging, there was high intraobserver reproducibility with kappa values of 0.93 for observer 1 and 0.87 for observer 2. These indicate that each observer had excellent consistency in his classification. Analysis also showed substantial interobserver reliability, with an overall kappa value of 0.79. The kappa values for interobserver reliability of each stage were 0.96 for stage 0, 0.91 for stage 1, 0.84 for stage 2, 0.89 for stage 3, 0.68 for stage 4, 0.71 for stage 5, and 0.75 for stage 6. While the degree of agreement was lower for later stages, the level of agreement among observers can be classified as between “substantial” and “almost perfect” agreement for all stages based on the kappa coefficient.
Discussion
The most important finding of this current study is that the development of peripheral tears in CDLM is characterized by a progressive sequence. The meniscus becomes more unstable as the stages increase, leading to greater meniscal displacement and potential cartilage wear. It is important to point out that stages 5 or 6 are not necessarily the common endpoint of all CDLM peripheral tears, because a high proportion of symptomatic DLM tears will be treated operatively in the lower stages, and conducting a longitudinal study on a symptomatic patient cohort to observe tear progression would be unfeasible. Nevertheless, the pattern of peripheral tears appears to follow a coherent and intuitive sequence of progressive worsening.
The inherent peripheral rim instability of DLM has been well documented in the literature. Good et al 6 reported that 77% of patients who underwent arthroscopic treatment for symptomatic discoid meniscus had meniscal instability, and devised a classification system based on the presence of instability as a result of deficient capsular attachment. Ahn et al 1 described the concept of meniscal “shift,” which is the separation of the peripheral portion of the DLM from the capsule, and showed that shift-type knees had a significantly larger number of peripheral tears compared with non–shift type knees. Kim et al 13 reported that even intact DLM had greater peripheral rim instability compared with normal lateral meniscus upon arthroscopic probing; they concluded that DLM has inborn peripheral instability that predisposes it to tears. In the recent comprehensive Pediatric Research in Sports Medicine classification system for DLM, abnormal stability was included as a major component of subclassification, highlighting its significance in the pathophysiology of DLM tears. 16 Such instability will inevitably lead to mechanical symptoms such as locking, limitation of motion, and giving way. Under such shearing forces and mechanical load, DLM will likely be more susceptible to tear progression and deformation, especially due to its irregular and disorganized arrangement of collagen. 21
In the lower stages, diagnosis of CDLM is relatively straightforward due to its characteristic features on MRI. In the later stages, however, as the meniscus is translocated and deformed, it becomes more difficult to distinguish from other incomplete DLM tears and bucket-handle tears of normal lateral meniscus. While bucket-handle tears of normal lateral meniscus also have a displaced fragment in the intercondylar notch, CDLM is characterized by a thicker blunt free edge. This is more apparent when examined during arthroscopy (see Figure 8). Based on this appearance, cases determined to be originally normal meniscus were excluded from this study, and only those appearing as CDLM were included.
Stage 6 deserves further elaboration. Upon reviewing our institution’s database of patients with lateral meniscal pathology, the authors encountered a cohort of patients with displaced lateral meniscal tear, severe meniscal degeneration, and accompanying lateral compartment osteoarthritis, but only mild clinical symptoms. Further analysis showed that these patients mostly had varus alignment of the affected extremity and were usually middle-aged to old age. Lim and Kim 17 have previously reported on the prevalence of lateral osteoarthritis in varus knees in the Asian population, but the long-term prognosis of lateral osteoarthritis and varus alignment remains unknown and unexplored in the literature. We hypothesized that in certain patients with CDLM and varus knees, a peripheral tear occurs due to the innate rim instability of DLM, but varus alignment naturally unloads the lateral compartment, and thus the tear progresses in a gradual manner with eventual lateral osteoarthritis as the long-term result. However, the steady progression may have conferred a degree of stability to the meniscus through deformation and secondary remodeling. The concept of secondary congruency has previously been used in acetabular fractures, where fracture fragments displace around the femoral head such that the overall congruity of the hip joint is maintained. 17 In our study, secondary congruency denotes a state where stability has been achieved by a translocated meniscal tear, akin to a ring-shaped meniscus. Unraveling the complex interplay between lateral osteoarthritis, varus alignment, CDLM tears, and increasing age is beyond the scope of this paper, and progressing to stage 6 will probably only occur in select cases. Nevertheless, while certain assumptions regarding this final stage are based on conjecture, we believe this final stage should be included in this classification, as it highlights a potential long-term outcome of CDLM peripheral tears that may help elucidate its pathophysiology and prognosis.
The landscape of orthopaedic research has seen a surge in investigations into DLM in recent years, particularly pertaining to the classification of DLM variants and their clinical implications.1,6,9,14,16 The numerous classification systems that have been developed to date have primarily emphasized structural morphology and arthroscopic characteristics. However, none has outlined any staged relationship or dynamic progression of peripheral tears within CDLM, which was a primary motivator for the present study. Our results add a temporal dimension to the existing structural classifications, offering a more comprehensive view of CDLM pathology.
It has been previously reported that simple horizontal tears of DLM are associated with less articular cartilage degeneration compared with nonhorizontal tears in DLM. 5 The authors reported that in simple horizontal tears, there were no differences in the degree of cartilage degeneration according to the duration of symptoms, suggesting a relatively benign prognosis. Our study shows that peripheral tears of CDLM may behave in a different manner.
While we believe that the natural progression from lower to higher stages is logical and intuitive, stage 2 is especially important, as it represents a key watershed moment for the CDLM. Although symptomatic, an absence of any tears on MRI may present a dilemma for the surgeon on the optimal course of treatment. Upon close inspection, these CDLM may display peripheral thinning or mass shifting, features of what may be considered a “functional tear.” In such cases, surgical intervention should be considered to reshape and repair the meniscus to prevent progression into later stages. On the contrary, the proposed stage 6 represents a chronic, long-standing, and fixed tear of CDLM that has gained a secondary congruency status that confers a certain amount of stability to the lateral compartment. In this case, meniscectomy may in fact destabilize the lateral compartment and potentially accelerate cartilage wear, so surgeons should be cautious of proceeding with operative treatment.
The proposed staging system provides a structured framework for categorizing peripheral tears of CDLM into 7 distinct stages, each associated with specific clinical manifestations and potential prognostic implications. Reliability assessment has demonstrated high intraobserver reproducibility and interobserver reliability of this system. Statistical analysis has demonstrated that this classification system can be used to categorize peripheral tears of CDLM in a highly reliable fashion. As a vital component of the knee joint, the meniscus plays a pivotal role in safeguarding articular cartilage. Our staging system not only characterizes peripheral tear progression but also highlights the potential for cartilage degeneration in later stages. By understanding the staged progression of these tears, surgeons can tailor their interventions according to the identified stage, potentially directing clinical interventions toward the preservation of both meniscal and cartilaginous integrity.
The complex interplay of factors contributing to the progression of DLM peripheral tears remains an area for exploration. Recent studies have shed light on genetic predisposition, joint biomechanics, meniscal morphology, and the role of inflammatory mediators in meniscal pathology.3,4,18,19,22 Future research should endeavor to elucidate the intricate mechanisms governing the progression of DLM tears, potentially offering novel therapeutic avenues.
This study supplements the existing literature by introducing a staging system that characterizes the temporal evolution of peripheral tears of CDLM. Later stages were defined by more severe tear patterns and cartilage degeneration. This does not necessarily mean that prophylactic partial meniscectomy needs to be performed in all stage 0 patients, and defining the appropriate time of surgical intervention is not within the purview of this paper. However, the evidence hints at the possibility that if surgery is performed at an earlier stage, partial meniscectomy may be sufficient instead of meniscal repair or total meniscectomy.
Limitations
This study has several limitations. First, although a longitudinal observational study would be the most ideal design for basing a staging system, this is practically and ethically infeasible for patients with symptomatic meniscal tears. While a small number of patients had serial imaging data (see Figure 1), there were an insufficient number for full-scale observational study. Thus, there are inevitably shortcomings due to the cross-sectional nature of the current investigation, but when viewed holistically, we believe a pattern of tear progression is readily apparent. Second, although stage 0 was included to represent a nonpathologic status, the true prevalence of asymptomatic CDLM is unknown, and not all CDLMs progress to peripheral tears. Further investigation is warranted to identify which factors influence the propagation of peripheral tears in CDLM. Third, while MRI was used for assessment of cartilage status, the gold standard for cartilage evaluation is arthroscopic examination. However, a number of patients in stages 0 and 6 did not receive arthroscopic treatment, and thus MRI findings were utilized instead. Fourth, as the stages progress and the meniscus becomes progressively translocated and deformed, it becomes more difficult to discern the original shape of the lateral meniscus. While this may have caused errors in inclusion of CDLM and exclusion of incomplete DLM and normal lateral meniscus for higher stages, we believe that this doesn’t affect the fundamental findings of this study, as the end stage of chronic tears may be similar regardless of the original morphology of the lateral meniscus. Finally, the retrospective and single-center nature of this study is intrinsically constrained by the potential for selection bias and the limitations inherent in historical patient records. Thus, the generalizability of our staging system warrants external validation through broader multicenter studies.
The clinical relevance of this research aligns with recent trends in personalized medicine and cartilage preservation, emphasizing the criticality of timely and targeted interventions. Despite its limitations, this study sets the stage for further research endeavors to validate and expand upon our findings and delve deeper into the multifaceted dynamics governing the progression of peripheral tears of CDLM.
Conclusion
Progressive stages characterize the development of peripheral tears in a CDLM. Higher stages are associated with more severe displacement of tears. Continued progression may lead to further degeneration of meniscal tears and cartilage erosion.
Footnotes
Final revision submitted November 9, 2024; accepted December 10, 2024.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from University of Ulsan College of Medicine (S2023-1648-0001).