
Abstract
Background:
The primary etiology of Little League shoulder (LLS) is rotational torque caused by repetitive throwing motion. However, there are few reports on the assessment of rotational torque during physical examination.
Purpose:
To investigate the usefulness of the resisted external rotation test (RERT) and the resisted internal rotation test (RIRT) in diagnosing LLS and determining the time to return to sports (RTS).
Study Design:
Case series (diagnosis); Level of evidence, 4.
Methods:
In total, 101 patients were diagnosed with LLS by proximal humeral physeal widening on radiography and tenderness on palpation over the lateral aspect of the proximal humerus, and the RERT and the RIRT were performed. During the 2 tests, the examiner lifted the patient’s elbow joint with one hand toward the humeral shaft and held the patient’s wrist joint with the other hand. In the RERT/RIRT, the patient was instructed to apply a maximal force of external/internal rotation from neutral alignment. The examiner resisted the force of external/internal rotation and maintained the setting position while holding the wrist joint. These test results were positive if either or both tests elicited shoulder pain. Positive test results and their association with radiographic findings were examined. In case of positive test results, the time to achieve negative test results and the time to RTS were investigated.
Results:
The RERT and RIRT were correlated with severity of LLS. The sensitivity of RERT/RIRT for LLS was 94.1%/36.6%, respectively. In RIRT, patients with advanced-stage LLS were more likely to have positive results than those with early-stage LLS (67.4% vs 10.9%; P < .001). The mean time to achieve negative RERT and RIRT results was 6.7 and 4.7 weeks, respectively (P = .01). Patients with advanced-stage LLS had a longer mean time to achieve negative RERT results than those with early-stage LLS (6.7 vs 4.7; P < .001). The time to RTS was 8.8 weeks in the group that resumed throwing after achieving negative RERT, while the group that resumed throwing before RERT became negative took 12.7 weeks (P < .001).
Conclusion:
The RERT may be useful in determining the presence of LLS and when RTS can be allowed.
Little League shoulder (LLS) is one of the most common throwing disorders in skeletally immature overhead athletes, such as baseball players. The incidence of LLS in young overhead athletes has been increasing approximately 8% per year on average. 6 LLS is often reported as a proximal humeral epiphysiolysis, and LLS diagnosis can be confirmed based on radiographic findings.1,3,2 The most common physical examination finding in LLS diagnosis is tenderness on palpation over the growth plate on the lateral aspect of the proximal humerus. However, it is not specific to LLS. 1 The current treatment recommendations for LLS comprise throwing cessation and physical therapy. Although return to sports (RTS) is an extremely important issue in sports injuries, there are no clear criteria for return to throwing and RTS in LLS. 1 Furthermore, despite the presence of an LLS grade classification system based on radiographic findings, 7 there are no reports on differences in time to RTS based on such a classification.
The LLS pathophysiology is strongly related to the number of throws and cumulative external rotational torque in the humeral shaft.9,10 This repetitive microtrauma damages the epiphyseal cartilage of the proximal humerus, which is the most vulnerable part of the structures surrounding the shoulder joint. 11 Considering the fact that the cartilage is more vulnerable to torsion than it is to tension, the primary etiology of LLS can involve torque application on the epiphysis by the throwing motion. Therefore, the torque applied on the proximal humeral epiphysis of patients with LLS can be an important finding for LLS diagnosis and management. To apply the torque to the proximal humeral epiphysis and to assess the symptom, the resisted external rotation test (RERT) and the resisted internal rotation test (RIRT), which are novel stress tests, have been developed.
The aims of the current study were to investigate (1) the sensitivity of the RERT and the RIRT for LLS, (2) the association between radiographic and physical findings using the RERT and the RIRT, and (3) the usefulness of these 2 tests as indicators of RTS.
Methods
Patient Selection
This study included patients diagnosed with LLS who performed the RERT and the RIRT. Proximal humeral physeal widening on radiography and tenderness on palpation over the growth plate on the lateral aspect of the proximal humerus were used as criteria for the diagnosis of LLS.6,8,12,2 If other throwing shoulder disorders, such as superior labral anterior and posterior lesion, rotator cuff inflammation, or thoracic outlet syndrome, were suspected based on physical examinations (eg, O’Brien active compression test, full can test, empty can test, and Roos test), ultrasound, or magnetic resonance imaging (MRI) were performed for a confirmed diagnosis. The cases with these other disorders were excluded in this study. As a result, the cases in which these physical examinations were positive were not included in this study.
Radiographic evaluation was performed by conducting anteroposterior radiography on external rotation of both shoulders. The LLS diagnosis was made based on a greater width of the proximal humeral physis in the throwing side than in the nonthrowing side. The LLS severity was investigated using the Kanematsu classification, which is a 3-grade LLS classification system based on radiographic findings (Figure 1). 7

The 3 Kanematsu classification grades included (A) grade I, widening of the epiphyseal plate only in the lateral area, (B) grade II, widening of the epiphyseal plate in all areas and demineralization of the metaphysis, and (C) grade III, a slipped epiphysis.
These radiographs were measured 3 times at different times by 2 authors (Y.S. and T.U.). Whenever there was a difference of opinion in determining the classification, the 2 discussed and agreed on the classification.
All patients were treated with nonoperative management comprising physical therapy and/or throwing cessation based on the same rehabilitation protocol. Physical therapy stretching exercises were performed with the aim of improving the tightness of the shoulder, trunk, and lower extremity. In principle, the patients returned to competition with a gradual increase in throwing intensity based on the 1-month throwing protocol established by our department (Supplemental Material, available separately; Tables A1 and A2).
Resisted External Rotation Test (RERT) and Resisted Internal Rotation Test (RIRT)
The RERT and the RIRT were performed with the patient seated, the shoulder joint positioned in approximately 30° of flexion and 30° of abduction, and the elbow joint in 90° of flexion (Figure 2). The position was not in the scapular plane. The examiner lifted the patient’s elbow joint with 1 hand toward the humeral shaft. This was performed to eliminate the effect of the deltoid muscles on the upper limb weights. The examiner held the patient’s wrist joint with the other hand. During the setting position, the examiner instructed the patient to relax to prevent muscle tension. In the RERT, the examiner applied a force with the hand holding the wrist joint in the direction of internal rotation of the patient’s shoulder joint. The patient was instructed to resist the force of internal rotation and maintain the setting position (Figure 2A). The examiner assumed the same setting position in the RIRT as in the RERT. The examiner applied a force with the hand holding the wrist joint in the direction of external rotation. The patient was instructed to resist the force and maintain the setting position (Figure 2B). A positive test result was defined as shoulder pain during the test. A negative result is defined as no shoulder pain during the test. All tests were performed by a single assessor (Y.S).

In the (A) resisted external rotation test (RERT), the patient was instructed to apply a force of external rotation (ER). The examiner resisted the force of ER and maintained the setting position while holding the wrist joint. In the (B) resisted internal rotation test (RIRT), the patient was instructed to apply a force of internal rotation (IR). The examiner resisted the force of IR and maintained the setting position while holding the wrist joint.
Clinical Examination
The positive rates of the RERT and the RIRT in LLS cases were investigated. We also investigated the time to achieve negative RERT and RIRT results and the time to return to competition. The time to RTS was defined as the ability to return to the initial level of competition without any change in position. The time to return to competition was compared between 2 cohorts: group 1, who started throwing after achieving negative test results, and group 2, who started throwing before achieving negative test results. The patients who returned to throwing despite symptoms did so because of team circumstances, such as a limited number of players or personal ambitions. Therefore, there were variable decisions in whether to return to throwing before or after resolution of symptoms. Two cases were excluded from the evaluation of return to competition: first, cases of unknown resumption time to throw; and second, cases with concomitant diseases, as pain from concomitant diseases may have delayed their return to competition.
Statistical Analysis
The Mann-Whitney U test was used to compare continuous variables. The Fisher exact test or the chi-square test was utilized to compare categorical variables between the 2 groups. P values of <.05 were considered statistically significant. A post hoc power analysis was performed with G*Power Version 3.1. According to P values of .05, the sample size could achieve a power of 0.80 based on a 2-tailed significance test. Prism9 (Version 9.5.1; GraphPad Software) was used for statistical analysis.
Results
In total, 124 patients diagnosed with LLS from July 2012 to January 2022 were retrospectively evaluated. These patients were all baseball players. Patient information was extracted from hospital medical records according to the diagnostic name. Patients were examined and treated by a single orthopaedic surgeon (Y.S.). The intervals between follow-up visits after an LLS diagnosis were typically every 4 weeks. Among 124 patients, 23 were excluded from this study due to the following reasons: absence of follow-up after the initial presentation (n = 15) and anteroposterior radiography of the shoulder obtained on the throwing side alone (n = 8). After the application of the exclusion criteria, 101 patients were selected (Table 1). All patients had an open proximal humeral physis. There were 2 cases where the time from the onset of disease to visit was unknown.
Patient Characteristics

In total, 99 boys and 2 girls, with a mean age of 13.3 years (range, 7-17 years), were included in the retrospective analysis. Table 1 shows the baseline demographic characteristics of the patients, including age, throwing side and position, the time from the disease onset to visit (≤1 month or >1 month), and concurrent diagnoses. Although 55 and 46 patients had grade I and II disease, respectively, none of the patients had grade III disease, based on the Kanematsu classification. We also compared these demographic characteristics between grade I and grade II (Table 2). The patients with grade II were significantly younger than the patients with grade I, but there were no significant differences in other demographic variables.
Comparison Between the Kanematsu Classification Grade I and Grade II in Patient Background
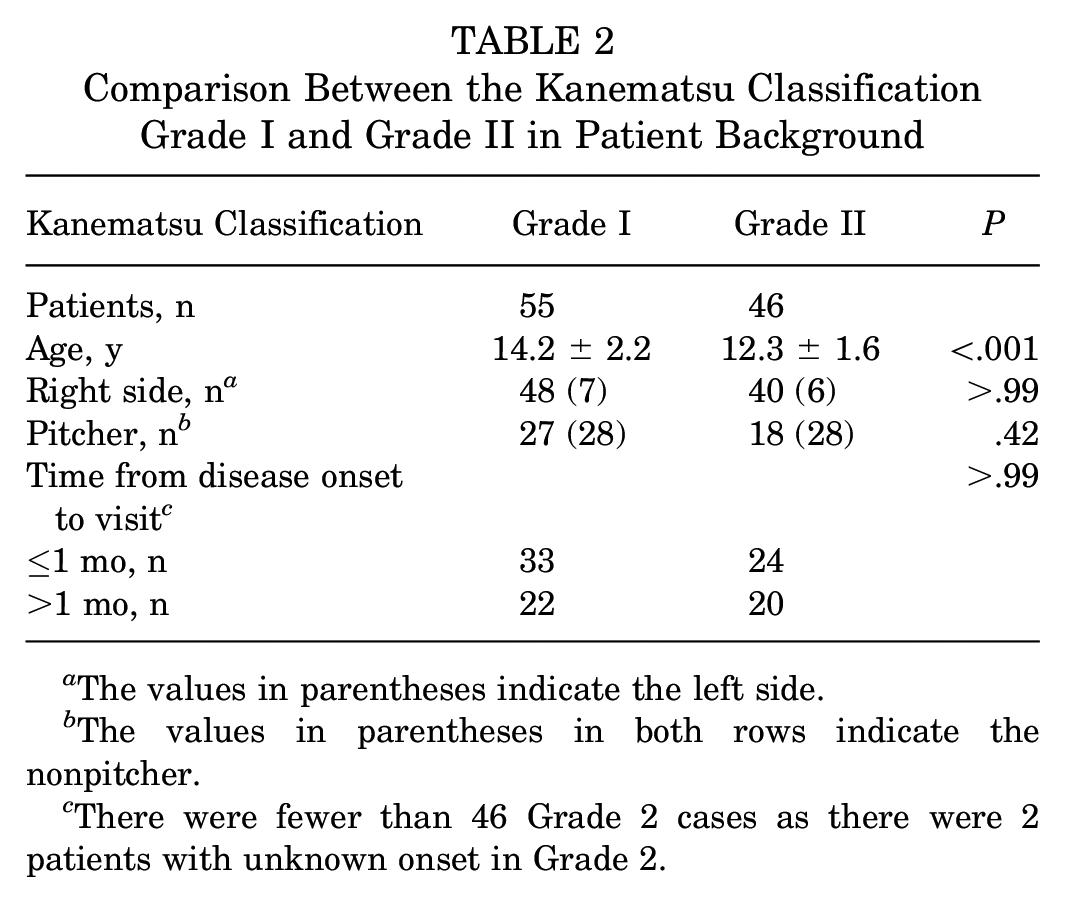
The values in parentheses indicate the left side.
The values in parentheses in both rows indicate the nonpitcher.
There were fewer than 46 Grade 2 cases as there were 2 patients with unknown onset in Grade 2.
Table 3 shows the association between the RERT results and the Kanematsu classification. The sensitivity of RERT to LLS was 94.1% (95/101). The sensitivity to grade I was 89.1% (49/55) and to grade II was 100% (46/46).
The Association Between the RERT Results and the Kanematsu Classification a

RERT, resisted external rotation test.
The association of RIRT and the Kanematsu classification is presented in Table 4.
The Association Between the RIRT Results and the Kanematsu Classification a

RIRT, resisted internal rotation test.
The sensitivity of RIRT to LLS was 36.6% (37/101). The sensitivity to grade II was significantly higher than that of grade I (P < .001) (grade I, 10.9% [6/55]; grade II, 67.4% [31/46]) in the RIRT. There were no cases in which only the RIRT result was positive. As this study included only cases diagnosed with LLS, it was not possible to calculate the true specificity, positive predictive value, or negative predictive value. However, these values could be calculated under the condition that these tests were used to determine the presence of grade II. The sensitivity of RERT for grade II was 100% (46/46), the specificity was 10.9% (6/55), the positive predictive value was 48.4% (46/95), and the negative predictive value was 100% (6/6). On the other hand, the sensitivity of RIRT for grade II was 67.4% (31/46), the specificity was 89.1% (49/55), the positive predictive value was 83.8% (31/37), and the negative predictive value was 76.6% (49/64). From these results, RIRT may help assess the severity of LLS.
We examined the time to achieve negative RERT and RIRT results in patients with positive test findings (Table 5).
The Time to Achieving Negative RERT and RIRT Results a

RERT, resisted external rotation test; RIRT, resisted internal rotation test.
In the cases of Kanematsu classification grade II disease, the time to achieve negative RIRT results was earlier than the time to achieve negative RERT findings (P = .01). Patients with grade I disease had a significantly earlier time to achieve negative RERT results than those with grade II disease (P = .003).
The patients were also divided into 2 groups in terms of the time to return to throwing after (group 1) and before (group 2) achieving negative test results. In total, 29 patients with concurrent complications (Little League elbow, 19 cases; medial collateral ligament insufficiency, 2 cases; osteochondral dissecans, 3 cases; olecranon stress fracture, 1 case; spondylosis, 1 case; Sever disease, 3 cases) and 12 with uncertain time to return to throwing were excluded from the analysis (Table 1). Because there were only 3 cases of Kanematsu classification grade I disease in group 2, we selected only grade II cases for investigating the time to achieve negative RERT and RIRT results and the time to return to competition (Figure 3).

Flow diagram of patient selection. RERT, resisted external rotation test.
Finally, 14 cases in group 1 and 11 cases group 2 were involved. Table 6 shows the summary results. Group 1 had a significantly earlier time to achieve negative RERT results (P < .001) and time to return to competition (P < .001) than group 2.
Comparison Between the 2 Groups in Terms of Time to Return to Throwing After and Before Achieving Negative Test Results a

Group 1 started throwing after achieving negative test results. Group 2 started throwing before achieving negative test results. RERT, resisted external rotation test; RIRT, resisted internal rotation test.
The values in parentheses in both rows indicate the left side.
The values in parentheses in both rows indicate the nonpitcher.
Discussion
This study aimed to investigate the usefulness of the RERT and the RIRT in LLS diagnosis and management. Regarding the comparison between Kanematsu classification and patient background, the patients with grade II were significantly younger than those with grade I, but there were no significant differences in other demographic variables. The RERT had high sensitivity in all LLS grades. The RIRT in Kanematsu classification grade II had a significantly higher sensitivity than that in grade I. In cases with positive RERT and RIRT results, the RIRT had a faster time to achieve negative results than the RERT. Patients with grade II disease had a significantly longer time to achieve negative RERT results than those with grade I disease. Patients who started throwing after achieving negative RERT results had a significantly earlier time to return to competition than those who started throwing before achieving negative RERT findings.
In the comparison between the Kanematsu classification and patient background, the younger the patients were, the more likely they were to have grade II. Progress to grade II, in which the medial proximal epiphysis of the humerus is widening, requires the medial epiphysis to remain open. As the patient ages, the medial proximal epiphysis of the humerus gradually closes from the medial side. Thus, older patients do not typically exhibit a widening of the medial epiphysis. This may be the reason why more cases of grade II were observed in younger patients. If the time from the onset to visit were to be longer, such as ≥3 months, there is a possibility that the number of cases progressing to grade II might increase.
This study showed that the RERT had a high sensitivity for LLS (94.1%). When performing RERT, the patient attempts to externally rotate the shoulder joint. The main external rotators of the shoulder joint are the infraspinatus and the teres minor, which insert proximal to the epiphysis.11,2 In the RERT, the patient contracts the infraspinatus and the teres minor muscles, which exert an external rotational force proximal to the epiphysis. While the examiner resists it, an internal rotation force is applied distal to the epiphysis. Because the insertions of these rotator cuffs involve a greater tuberosity on the proximal lateral side of the humeral epiphysis, a strong rotational torque is produced in the lateral side of the epiphysis in the RERT (Figure 4A).

Schematic representation of the (A) resisted external rotation test (RERT) and the (B) resisted internal rotation test (RIRT) for Little League shoulder (LLS). The solid line is the anterior epiphyseal line, and the dashed line is the posterior epiphyseal line. ER, external rotation; IR, internal rotation; *, insertion of infraspinatus tendon; #, insertion of subscapularis tendon.
Therefore, patients with LLS who had injury on the lateral side of the epiphysis were likely to have positive RERT results. Kanematsu et al 7 have reported that the radiographic staging process of LLS initially begins along the lateral side and then extends medially. Further, the lateral side of the proximal humeral epiphysis is damaged in all LLS stages. This can be the reason why, in the current study, the RERT had high sensitivity in all LLS stages.
Meanwhile, in this study, the sensitivity of the RIRT for LLS was 36.6% (37/101). The sensitivity of the RIRT in patients with grade II disease was significantly higher than that in patients with grade I disease (67.4% [31/46] vs 10.9% [6/55]). When performing RIRT, the patient attempts to internally rotate the shoulder joint. The main internal rotators of the shoulder joint are the subscapularis and pectoralis major, latissimus dorsi, and teres major. Of these muscle groups, only the subscapularis muscle is inserted proximal to the epiphysis. In the RIRT, the patient contracts the subscapularis muscle, which exerts an internal rotation force proximal to the epiphysis. If the examiner resists it, an external rotational force is applied distal to the epiphysis. Because the insertion of the subscapularis involves a lesser tuberosity, a strong rotational torque is applied medially from the lesser tuberosity (Figure 4B). Therefore, the RIRT result can be positive only in advanced-stage LLS with physeal widening medial to the lesser tuberosity.
Considering RTS in LLS cases, the time to return to throwing can be an important issue. This study compared the group who started throwing after achieving negative test results (group 1) and the group who started throwing before achieving negative test results (group 2). The time to achieve negative RIRT results was significantly shorter than time to achieve negative RERT results in patients with grade II disease. Therefore, healing may occur on the medial side of the epiphysis by reducing the intensity of throwing. Radiographic findings have already revealed the associated mechanism, which is consistent with our thoughts. The time to RTS in groups 1 and 2 were 8.8 and 12.7 weeks, respectively. In addition, in the case of LLS, epiphyseal tenderness to palpation usually becomes negative first, followed by the RERT. Therefore, by the time they resume throwing, the tenderness in these cases has already subsided. Thus, the time to achieve negative test results might be a better indicator to safely shorten the time to RTS. The mean time for radiographic finding improvement with throwing cessation is 18.8 weeks. 8 Meanwhile, previous studies have reported that patients can start throwing after 11.2 to 16 weeks using symptom resolution as the criterion for return to throwing.5,6 In this study, the time to RTS was 8.8 to 12.7 weeks. Although this is a comparison study between different cases and institutions, patients with LLS may return to competition earlier based on improvement in RERT results rather than imaging findings. We believe that this is an important finding because a prolonged period of throwing cessation is not desirable for adolescent athletes who have limited playing years. Recurrence was not considered in this study because follow-up was terminated when the patient fully recovered.
Patients with LLS have a high incidence of RERT and a low incidence of RIRT. The RERT is a better test than the RIRT for determining the presence of LLS. Therefore, the RERT might be used as a screening tool for patients with shoulder pain. If symptom resolution is used to assess readiness to return to throwing, it is preferable to define symptom resolution based on the RERT’s becoming negative, as the RERT turns negative later than the RIRT. Based on the results of this study, the RERT may be useful in determining when RTS can be allowed.
Limitations
This study had several limitations. First, the validity of LLS diagnosis is unclear because there is no gold standard for LLS diagnosis. In the review of past literature, the diagnosis of LLS was based on the presence of physeal widening on plain radiographs and/or MRI and symptoms in 99% of reported cases. 1 Therefore, the presence of physeal widening is essential for the diagnosis of LLS. Although there are various reports on symptoms, tenderness was reported as a symptom in two-thirds of the reports. Therefore, following previous reports, the present study used proximal humeral physeal widening on radiography and tenderness on palpation over the growth plate on the lateral aspect of the proximal humerus as criteria for the diagnosis of LLS.6,8,12,2 Second, we can’t really assess the specificity of the tests because no other shoulder diagnoses were included. We did not investigate the cases of injury to the external or internal rotator muscles of the shoulder joint. The RERT would be positive in cases of infraspinatus muscle injuries. The RIRT findings also could be positive in cases of subscapularis muscle injuries. These tests can have false-positive results in cases of rotator cuff tear. However, the incidence of pediatric rotator cuff tears is extremely rare. 4 If these tests are applied as a diagnostic tool for throwing shoulder injuries, it is necessary to consider that the abovementioned disorders may be masked. Third, there is a lack of biomechanical studies on RERT and RIRT. We have not verified by biomechanical studies that these tests actually impart torque at the epiphysis, and no similar studies have been conducted to date. It would be desirable to investigate whether other muscles are contracting during the test by needle electromyography, but we were not able to investigate that in this study. Therefore, we have no knowledge of how much torque was applied for each patient. Fourth, this study is a survey conducted over a period of about 10 years, and there is a concern about potential recall bias. However, because all data were extracted from the hospital medical records, they are not subject to recall bias. Additionally, the follow-up intervals were typically every 4 weeks. Therefore, we cannot rule out the possibility that the “time to negative RERT/RIRT” was 1, 2, or 3 weeks. Finally, no data comparing pitchers and fielders were included in this study. Thus, further study is needed to elucidate the effect of each position.
Conclusion
The patients with LLS had a high incidence of RERT. The RERT is a better test than the RIRT for determining the presence of LLS. The RERT may be useful in determining when RTS can be allowed.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671251331055 – Supplemental material for Novel Stress Tests for Diagnosing Little League Shoulder and Determining the Timing of Return to Sports
Supplemental material, sj-pdf-1-ojs-10.1177_23259671251331055 for Novel Stress Tests for Diagnosing Little League Shoulder and Determining the Timing of Return to Sports by Takahiko Uchino, Yasunori Shimamura, Taichi Saito, Ryo Nakamichi and Toshifumi Ozaki in The Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted November 20, 2024; accepted December 2, 2024.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.