
Abstract
Background:
Adolescents and young adults comprise a growing cohort at risk for exercise-related injuries. Recent studies compare the effects of cardiovascular and strength exercise on mental health, cardiovascular disease, and mortality; however, there remains a gap in the literature about acute injuries from these exercise types.
Hypothesis/Purpose:
The purpose was to compare acute orthopaedic injuries sustained during cardiovascular exercise versus strength training in adolescents and young adults. A secondary aim was to compare the distribution of age, sex, and injury characteristics with the types of exercise. Finally, it was hypothesized that injuries would have increased throughout the previous 5 years.
Study Design:
Descriptive epidemiology study.
Methods:
This retrospective study used a National Electronic Injury Surveillance System (NEISS) query to identify patients aged 14 to 22 years with orthopaedic injuries due to exercise activities from 2018 to 2022. Injuries were attributed to cardiovascular exercise or strength training, which included weightlifting. Descriptive data were reported, and statistical comparisons were conducted via chi-square tests, Fisher exact tests, or linear regressions.
Results:
The NEISS query identified 3105 cases. A total of 1474 (50.9%) cases were attributed to cardiovascular exercise and 1423 (49.1%) to strength training—including 1136 (39.2%) to weightlifting. Also, 48.4% of cardiovascular-related and 75.1% of strength-related injuries occurred in men. The number of patients with cardiovascular-related (b = −7.983; P = .013), strength-related (b = −15.05; P = .001), and weightlifting-related (b = −11.78; P = .004) injuries decreased with increasing age. Most injuries were sprains/strains (68.2% cardiovascular-related vs 50.4% strength-related). There were more upper extremity injuries during strength training (65.9%) than cardiovascular exercise (16.3%) (P < .001). No significant changes were observed in the annual number of injuries (b = −20.70; P = .442).
Conclusion:
Thousands of adolescents and young adults are injured each year while exercising. Strength training injuries were more common in men, but cardiovascular exercise injuries were comparable between men and women. Young age was associated with higher injury rates from all exercise types. Cardiovascular and strength exercises were associated with different injury patterns. Future studies should consider longer periods and overall participation to compare the incidence between cardiovascular and strength exercise.
Keywords
Because of increased sports participation, greater accessibility to gyms, and more attention to bodily appearance or wellness, more young people are participating in aerobic and strength training.1,8,9 According to the International Health, Racquet & Sportsclub Association (IHRSA) global report, 19 gym attendance has been steadily increasing each year, with 66.5 million Americans holding gym memberships in 2021. Newly renamed as the Health and Fitness Association, this trade group has represented and conducted research with over 200,000 gyms and fitness centers worldwide since 1981. The IHRSA report 1 also found that young adults, defined as individuals aged between 18 and 34 years, were the largest age group who frequented the gym at 60.60% in 2020. Exercise has been found to have significant health benefits at all ages, ranging from decreasing anxiety and depression to reducing risks for cardiovascular diseases, strokes, and diabetes. 17 Exercise has also been associated with increased bone and muscle strength, cognitive development, and academic performance in children and adolescents.12,17
Studies have compared the benefits and risks of aerobic and strength training.3,5,11,14 Both forms of exercise have been shown to decrease mortality risk at just 1 hour a week. 3 Aerobic exercise has been widely accepted to improve cardiovascular health, and recent studies have shown that muscle-strengthening activities are also associated with decreased risk of cardiovascular diseases and cancer.11,14 However, there has been controversy surrounding the benefits of weight training among children and adolescents.5,15,20 In 2008, the American Academy of Pediatrics (AAP) stated that “strength training is only a small part of an overall fitness or sports program” and neither necessary nor appropriate for every child, highlighting the risks of injury during weight training and unclear benefits to athletic performance and injury prevention. 4 Their safety concerns were based on a large number of weightlifting and equipment injuries among 8- to 19-year-olds, especially while unsupervised.5,15 In addition, growth plate injuries could have lasting effects on young children, and soft tissue and lower back injuries were common in adolescents and young adults. 5 Yet, the AAP revised its recommendations in 2020 because of the continual rise in strength training and its proven benefits for injury prevention and sports performance. The AAP now supports strength and resistance training in adolescents, particularly under supervision. 20
While many studies compare long-term health benefits and mortality risk reduction of aerobic and strength exercises, there is a gap in the literature about acute injuries between these forms of exercise, especially among adolescents and young adults. This age group is increasingly participating in physical activities and, thus, is at risk for associated injuries. Therefore, this study aimed to compare the number of exercise-related injuries between cardiovascular exercise and strength training in adolescents and young adults. In addition, we anticipated a difference in the distributions of age and sex between patients injured during cardiovascular exercise and those injured during strength exercise. We also hypothesized that injury types and body parts injured would differ between the 2 groups. Last, we hypothesized that the annual incidence of exercise-related injuries would increase with rising participation in cardiovascular and muscle-strengthening activities.
Methods
This was a retrospective study using the National Electronic Injury Surveillance System (NEISS) data set, which is based on a probability sample of United States emergency departments (ED). NEISS data are managed by the United States Consumer Product Safety Commission and are representative of all national EDs based on department size and geographic location. 22 This study was exempt from institutional review board approval, as it used previously collected and publicly available data.
The NEISS database was queried by a single investigator (H.L.) for patients aged 14 to 22 years who sustained orthopaedic injuries while participating in “exercise without equipment,”“exercise with equipment,” and “weightlifting” activities. The query covered 5 years from January 1, 2018, to December 31, 2022, to include a large number of patients with the most recent injuries. All query results were reviewed by 5 authors (H.A.L., A.A., O.S.A., H.S.K., and T.L) for validity. Demographic data of interest included sex and age. Of the queried cases, injury types and diagnosis codes included avulsion (code 72), crushing (code 54), dislocation (code 55), fracture (code 57), and sprain/strain (code 64). Diagnoses were predetermined by ED records and assigned to NEISS codes accordingly. 23 According to the NEISS coding manual, avulsion diagnoses are defined as soft tissue tears—including lacerations and degloving—and crushing is defined as severe external pressure.18,23 The query also used codes to search for injured body parts of the upper extremity—shoulder (code 30), upper arm (80), elbow (code 32), lower arm (code 33), wrist (code 34), hand (code 82), and finger (code 92)—and lower extremity—upper leg (code 81), knee (code 35), lower leg (code 36), ankle (code 37), foot (code 83), and toe (code 93). As there was no code for the back, injuries of or around the spine were not included.
Exercise type was determined by descriptions in the NEISS narrative. While certain exercises fell under query categories, such as running under “exercise without equipment,” pull-up bars and yoga balls under “exercise with equipment,” and dumbbells under “weightlifting,” each result had to be individually sorted under the exercise cohorts. For example, cardiovascular exercise included running, jogging, biking, jump roping, using the elliptical or stationary bicycle, jumping, walking, or hiking. Strength exercises included squats, lunges, push-ups, pull-ups, calisthenics, using free weights or weight machines, yoga, mat exercises, and stretching. Weightlifting exercise was the subset of strength exercise involving any free weights such as barbells, dumbbells, or any weight machine. Some narratives described “working out” or “exercising” activities that could not be classified as either cardiovascular or strength exercise and were excluded from the comparative analysis (N = 208). Injuries sustained during organized or recreational sports were excluded by the query to maintain the study's focus on gym- and fitness-related exercise.
National case estimates were calculated by NEISS weighted estimates using 95% CIs. 21 The Pearson chi-square test was used to compare proportions of injuries between exercise types with respect to sex, injury type, and injured body parts. The Fisher exact test (2-tailed) was used in cases where the number of injuries was <5. Linear regression was used to analyze differences with each year of age and over time. All statistical analyses were performed using SPSS Statistics Version 29.0.2.0 (IBM). 10 The alpha value of this study was set at .05, and any calculated P values less than this level were considered statistically significant.
Results
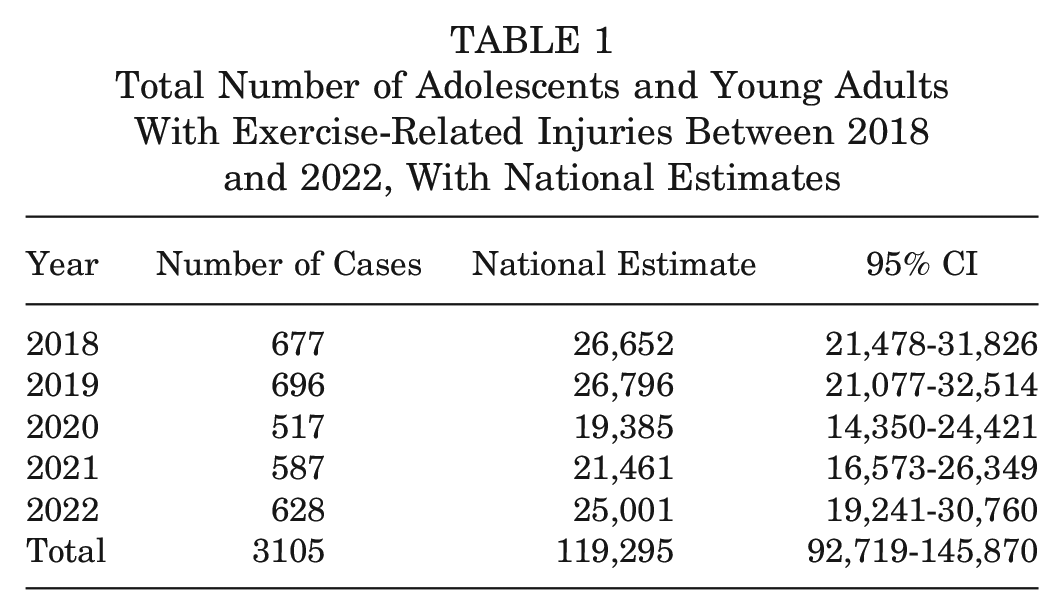
There were 3105 cases in the NEISS data set of patients aged between 14 and 22 years who had avulsion, crushing, dislocation, fracture, and sprain/strain injuries to the upper and lower extremities, according to corresponding NEISS codes. By weighted estimates, this represents 119,295 patients nationally for this age group between 2018 and 2022 (95% CI, 92,719-145,870) (Table 1). On average, this would have been 23,859 patients annually due to exercise-related activity.
Total Number of Adolescents and Young Adults With Exercise-Related Injuries Between 2018 and 2022, With National Estimates
Of these cases, 1904 (61.3%) were male patients (Table 2). The mean age at injury was 17.6 ± 2.6 years. Because 315 patients had ≥1 injury, 3420 individual diagnoses were included in the study query, which included 3214 diagnoses of avulsion, crushing, dislocation, fracture, and sprain/strain injuries. The most common injury type was strain/sprain (60.8%), followed by fracture (25.6%). There were 3369 injuries of the shoulder, upper arm, elbow, lower arm, wrist, hand, fingers, upper leg, knee, lower leg, ankle, foot, or toes. There were more lower extremity injuries than upper extremity injuries (59.1% vs 40.9%, respectively), and the most common body parts injured were the ankle (24.5%), hand (18.3%), and shoulder (17.1%).
Descriptive Data of Adolescent and Young Adult Patients With Exercise-Related Orthopaedic Injuries From the NEISS Data Set Comparing Cardiovascular-, All Strength-, and Weightlifting-Related Injuries a

Data are presented as mean ± SD unless otherwise indicated. NEISS, National Electronic Injury Surveillance System.
A total of 315 patients had multiple injuries, contributing to 3214 diagnoses of avulsion, crushing, dislocation, fracture, or sprain/strain. Of these injuries, 1514 were cardiovascular-related, 1487 strength-related, and 1183 weightlifting-related.
A total of 315 patients had multiple injured body parts, contributing to 3369 injuries to the upper or lower extremities. Of these injuries, 1576 were cardiovascular-related, 1578 strength-related, and 1271 weightlifting-related.
A total of 2897 patients were reported to be injured during either cardiovascular or strength exercise between 2018 and 2022. Also, 1474 patients (50.9%) sustained injuries during cardiovascular exercise, and 1423 (49.1%) sustained injuries while participating in strength exercise. There was a significant difference between cardiovascular (48.4% men vs 51.6% women) and strength (75.1% men vs 24.9% women) exercise injuries with respect to sex (P < .001). Men were about twice as likely to have a strength-related injury instead of a cardiovascular-related injury than women (risk ratio [RR], 1.89 [95% CI, 1.72-2.07]; P < .001) and less likely than women to be injured during cardiovascular exercise (RR, 0.587 [95% CI, 0.548-0.629]; P < .001).
The mean age at injury was 17.7 ± 2.6 years for cardiovascular injuries and 17.4 ± 2.5 years for strength injuries (P = .001). The number of patients with cardiovascular-related (b = −7.983 [95% CI, –13.67 to −2.30]; P = .013) and strength-related (b = −15.05 [95% CI, –21.99 to −8.11]; P = .001) injuries decreased with increasing age (Figure 1).

Linear regression of injuries at each age from 14 to 22 years for all exercise types: cardiovascular (red), strength (dark blue), weightlifting (light blue), and total (black). Coefficients are shown in the table with associated 95% CIs and significance levels.

There was a significant difference between cardiovascular and strength exercise with respect to the distribution of injury types (P < .001) and body parts injured (P < .001). The most common injury type was sprain/strain, which constituted 68.2% of cardiovascular-related injuries and 50.4% of strength-related injuries. There were higher proportions of fractures (29.2% vs 24.2%) and dislocations (11.6% vs 7.1%) from strength exercise than cardiovascular exercise (Figure 2). Upper extremity injuries are composed of 16.3% of cardiovascular-related injuries and 65.9% of strength-related injuries (P < .001). The most common body parts injured during strength exercise were the hand (29.5%) and shoulder (29.3%), whereas the ankle (45.4%) and knee (16.9%) were most frequently injured during cardiovascular exercise (Figure 3).

Distribution of the types of injuries sustained during each type of exercise: cardiovascular (red), all strength (blue), weightlifting (light blue), and total (black).

Distribution of the body parts injured during each type of exercise. The left bars represent upper body injuries—including shoulder/upper arm (yellow), elbow/forearm (orange), and wrist/hand/fingers (red). The right bars represent lower body injuries—including the upper leg (light green), knee (dark green), lower leg (light blue), ankle (dark blue), and foot/toes (purple).
More specifically, 1136 (39.2%) patients were injured while lifting weights. The mean age at injury for these cases was 17.4 ± 2.5 years, and weightlifting-related injuries decreased with increasing age (b = −11.78 [95% CI, –18.24 to −5.325]; P = .004) (Figure 1). Male patients represented 78.3% of weightlifting injuries and were more than twice as likely to be injured while lifting weights than female patients (RR, 2.27 [95% CI, 2.02 to 2.56;] P < .001). The most common injuries due to weightlifting were strains/sprains (48.9%) and fractures (31.9%), and the most common body parts injured were the shoulder (27.1%), hand (32.7%), and foot (19%) (Figures 2 and 3).
Although there was a decrease in injured adolescents and young adults in 2020, there was no significant change in the annual number of injuries over the 5 years from 2018 to 2022 (b = −20.70 [95% CI, –95.33 to 53.93]; P = 0.442). No significant change was observed in the annual number of cardiovascular, strength, or weightlifting injuries during this period (Figure 4).
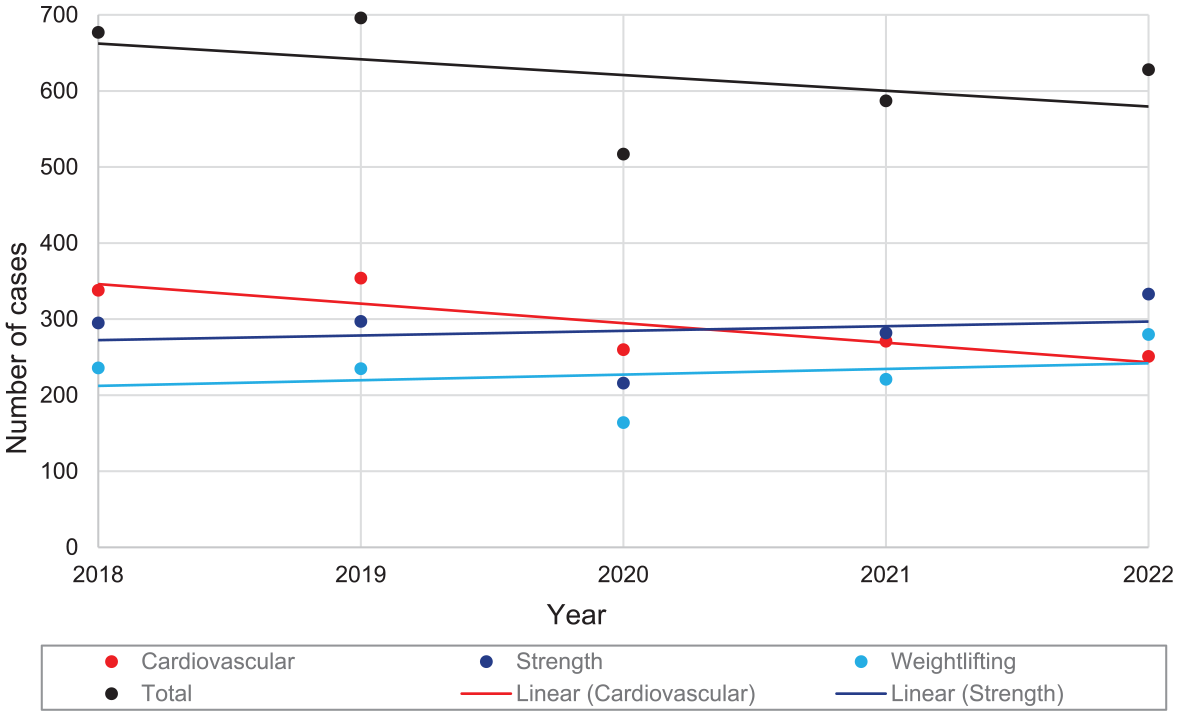
Linear regression of annual injuries from 2018 to 2022 for all exercise types: cardiovascular (red), strength (dark blue), weightlifting (light blue), and total (black). Coefficients are shown in the table with associated 95% CIs and significance levels.

With respect to location, 372 (12%) injuries occurred at school. Of these, 171 injuries were from cardiovascular exercises and 188 from strength training, of which 143 injuries involved weights. No significant difference was found between cardiovascular- and strength-related injuries in the proportion of injuries that occurred at school (P = .187).
Discussion
Despite the rising popularity of fitness and exercise, there is a gap in the literature about exercise-related injuries, especially among adolescents and young adults. By studying exercise-related orthopaedic injuries in the NEISS data set, this study hypothesized and demonstrated differences between cardiovascular and strength-related injuries. Although there was no difference in the number of injuries, the results found differences in age and sex distributions. Specifically, there was a younger mean age in strength- than cardiovascular-related injuries, as well as a similar number of male and female patients with cardiovascular exercise injuries, but more male than female patients with strength training injuries. In addition, more upper body injuries occurred during strength training whereas most lower body injuries occurred during cardiovascular exercise. Strength exercise was associated with more bony injuries, especially when weights were involved. Overall, the study rejected any annual trend in injuries despite growing participation in cardiovascular and muscle-strengthening activities.
Based on this NEISS sample from 2018 to 2022, there were an estimated total of 23,859 orthopaedic injuries in the ED per year among patients aged between 14 and 22 years due to exercise activities. Although adolescents and young adults are the majority age group at gyms with increasing attendance since 2010, there was not a significant increase in injuries over these 5 years.1,8 However, there was a notable decrease in the number of injuries due to both cardiovascular and strength exercise in 2020, likely related to gym closures and stay-at-home mandates during the coronavirus disease 2019 pandemic. The small increase in exercise-related injuries after 2020 potentially reflects a rise in physical activity and gym attendance as precautions fell. 13
Overall, there were more male than female patients. This difference was driven by strength exercise, as about three-fourths of strength injuries occurred in men. In addition, strength-related injuries were almost twice as likely to be found in men than women, whereas cardiovascular exercise was less likely to be the cause of injury in men than women. This discrepancy is likely attributed to the sex difference in weightlifting, specifically male patients represented almost 80% of weightlifting injuries and were 2.27 times more likely to have been injured while lifting weights than women. This is likely as much of a clinical as statistical difference, because past surveys reported more overall physical activity in male than female adolescents and young adults, and surveys2,6,16 on strength training revealed that 42.4% of male versus 26.1% of female adolescents did strength training most days or every day during 2021 and 2022. The male majority in strength training injuries may be attributed to more participation; however, it is difficult to ascertain if strength exercise is more common as opposed to more dangerous among men, or a combination of both.
Among adolescents and young adults, the mean age at injury for all patients was about 17 years, whether during cardiovascular or strength exercise. Even though strength injury patients were statistically younger than those injured during cardiovascular exercise, the difference was not clinically significant. Notably, there were more strength training than cardiovascular exercise injuries in those aged 14 to 17 years, then conversely, there were more cardiovascular than strength injuries in those aged 17 to 22 years. This trend suggests that as adolescents mature, there may be an inflection point when injuries are less likely incurred during strength training and more likely during cardiovascular exercise. This result is consistent with concerns that strength training may be more dangerous for younger individuals. 4
In addition, linear regression analysis revealed that injuries decreased with increasing age in the setting of all exercise types. Without quantifying the total number of participants, it is difficult to estimate incidence rates. Furthermore, recent data 2 show that opportunities, and thus participation, in moderate to vigorous physical activity declines after high school, from 87.9% of male and 78.1% of female adolescents (12-17 years) to 72.6% of male and 61.5% of female young adults (18-24 years). Thus, the decline in injuries with age may be attributed to fewer participants in young adulthood, rather than risks associated with concerns about skeletal immaturity, pubertal hormone deficits, and lack of supervision.4,5,15,20 There was not a difference between cardiovascular- and strength-related injuries that occurred at school; nonetheless, many strength training injuries might have occurred in unsupervised settings.
Of the 3214 diagnoses, the most common injury was strain/sprain for all exercise types. This supports literature reporting a high prevalence of soft tissue injuries among adolescents and young adults, especially for cardiovascular-related injuries. 5 Of the strength-related injuries, weightlifting contributed to almost all avulsion, crushing, and fracture injuries. Therefore, the addition of free weights and weight machines might incur risks of bony injury.
When comparing body parts injured during exercise types, there were more than 4 times more upper extremity injuries during strength than cardiovascular exercise. The majority of the strength-related injuries affected either the upper arm and shoulder or the wrist and hand, which was also true for weightlifting-related injuries. On the other hand, lower extremity injuries occurred most during cardiovascular exercise, with more than half involving the ankle. Previous studies found lower back injuries to be common among active adolescents and young adults, but the query did not include a code for back injuries, which were therefore not included in this study. 5 The exclusion of back injuries implies an underestimation of exercise-related injuries, especially those attributed to weightlifting, which has been associated with lower back injuries in adolescents and young adults. 7 Overall, the body parts injured during cardiovascular and strength exercises are consistent with the biomechanics required to run, jump, perform a push-up or dead-lift, and execute other movements that fall under either cardiovascular or strength exercise.
In addition, only 12% of injuries occurred at school, likely supervised by physical education teachers or coaches. Supervision or instruction could prevent exercise injuries, as counseled by the 2020 AAP recommendations. 20 Most injuries occurred outside of school and at NEISS codes “Home,”“Public,” and “Sports” (recreational sports, gyms and fitness centers, fitness classes, and outdoor sporting activities), which are assumed to be unsupervised. Because it is impossible to definitively claim whether activities were supervised or not based on the NEISS query, further studies are needed to test this hypothesis.
The NEISS data set represents a large national compilation of ED visits; however, this serves only as a representative sample of exercise-related injuries and has some limitations. This study is retrospective and primarily descriptive, intending to inform future studies in comparing injuries sustained during different types of exercise. Also, the NEISS database relies on external reports from around the country that must be verified for quality and consistency. Another limitation to consider is that the study focuses on acute injuries presented to EDs, and does not incorporate all chronic or overuse injuries, or injuries treated by school nurses, athletic trainers, team doctors, or primary care physicians in the outpatient setting. The exclusion of these patients underestimates the number of injuries and may skew our findings toward patterns associated with more acute and emergent problems.
Finally, because the NEISS data set cannot count the total number of exercise participants in the United States, this study reports only the number of NEISS cases and extrapolated national estimates. Thus, these results should be interpreted with the awareness that it was not possible to calculate the true incidence of injuries among adolescents and young adults who exercise. Instead, these findings serve as a representation of exercise injuries and prompt further investigation on this topic.
Conclusion
This study revealed differences between injuries due to cardiovascular exercise and strength training. Overall, young age was associated with higher rates of injuries for all exercise types. There was a comparable number of male and female patients with cardiovascular exercise injuries, but more male than female patients with strength training injuries. Strength training and weightlifting had more bony injuries and upper extremity involvement than cardiovascular exercise, which were associated with soft tissue and lower extremity injuries. While the study did not reveal a significant yearly trend, future studies should examine longer periods to quantify true injury rates and annual trends among adolescents and young adults.
Footnotes
Final revision submitted September 7, 2024; accepted November 27, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.D.K. is affiliated with the Arthroscopy Association of North America and has received hospitality payments from Baxter Healthcare; education payments from Paladin Technology Solutions and Arthrex; nonconsulting fees from Arthrex; and consulting fees from Heron Therapeutics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.