
Abstract
Background:
Posterior tibial slope (PTS) is commonly measured on lateral radiographs, but there is an ongoing discussion on which criteria are essential as quality standards.
Purpose/Hypothesis:
The purpose of this study was to evaluate the effect of malrotation of the tibia on lateral radiographs for PTS measurement. It was hypothesized that malrotation alters the measured PTS.
Study Design:
Descriptive laboratory study.
Methods:
An infratuberositary osteotomy was performed on a tibial saw bone model, and 3 conditions—2 with increased PTS—were tested with the same experimental setup (series 1, closed osteotomy; series 2, 5-mm anterior opening; series 3, 10-mm anterior opening). Long lateral radiographs were taken from +12.5° of external tibial rotation (ETR) to −20° of internal tibial rotation (ITR), in steps of 2.5°. PTS was measured with the mechanical axis (MA) and the proximal anatomic axis (PAA). In addition, the distance between the medial and lateral posterior tibial condyles was measured (in mm).
Results:
In test series 1, between +12.5° to 0° of ETR and 0° to−20° of ITR, a change in PTS of 2.8°± 1.0 (ETR) and 3.7°±1.3 (ITR) for the MA and 3.7°± 1.4 (ETR) and 4.1°±1.5 (ITR) for the PAA was detected. In test series 2, changes of 1.5°± 0.5 (ETR) and 3.7±1.3 (ITR) for the MA and 1.6°± 0.6 (ETR) and 4.3°±1.4 (ITR) for the PAA were observed; likewise, in test series 3, changes of 1.8°± 0.7 (ETR) and 3.7°±1.3 (ITR) for the MA and 2.2°± 0.9 (ETR) and 4.2°±1.3 (ITR) for the PAA were observed. ETR of +12.5° resulted in a distance of 5 mm, and ITR of −20° resulted in a distance of 10 mm between the posterior tibial condyles in all testing conditions. There was no significant difference among the 3 testing conditions (P > .05). A change of 1 mm in distance was equivalent to 2° (ITR) or 2.5° (ETR) of change in rotational alignment and 0.4° of change in PTS measurement, irrespective of whether MA or PAA was used.
Conclusion:
Tibial malrotation strongly influences PTS measurement on lateral radiographs. ETR leads to an underestimation, and ITR to an overestimation, of PTS. Every 1° of change in rotational alignment was equivalent to 0.2° of change in PTS measurement. For a reliable PTS measurement on lateral radiographs, the posterior tibial condyles should be superimposed exactly.
Clinical Relevance:
Dependent on PTS values, surgical correction of the PTS can be indicated. For a correct indication, it is of utmost importance to be able to determine the posterior slope exactly. This investigation demonstrates the effect of tibial rotation on PTS measurement and defines quality criteria, as well as a simple grading system for lateral radiographs for the measurement of the PTS. This helps surgeons to interpret radiographs correctly, allowing a better decision-making process, if and when a corrective osteotomy for PTS correction is indicated.
Keywords
The posterior tibial slope (PTS) is of great interest in the field of cruciate ligament reconstruction, as changes of the PTS have been described not only as an anatomic risk factor for graft insufficiency and rerupture, but also for primary anterior cruciate ligament (ACL) injuries.7,12,15,17,20,21
Different methods have been published to estimate the PTS. 18 They can be divided into 2 groups, one using the proximal part of the tibia to determine the PTS and the other using full-length lateral radiographs of the tibia. A proximal anatomic axis (PAA) is widely used to measure PTS values, as these measurement methods can be applied on standard short lateral radiographs.4,21 For PTS measurement on full-length lateral radiographs, comparable with deformity analysis in the frontal plane, there must be a distinction between measurements made using PAA and made using the mechanical axis (MA).14,24 Full-length lateral radiographs do have the advantage of detecting PTS deformities of the distal tibia as well. Multiple publications have addressed this topic, even comparing the different measurement methods with each other.3,6,24
Depending on the values measured for the PTS, the performing of corrective osteotomy may be indicated.5,22 For this reason, it is of utmost importance to provide reliable and reproducible lateral radiographs of the knee to allow a standardized measurement.
In the coronal plane, it is well known that malrotation of the tibia and the femur may lead to inaccurate measurement of axis deformities.1,2,10,13,16 Similar effects were reported for radiographs of the sagittal plane.11,23 These publications reported on incorrect measurement of the PTS due to protectional errors resulting from malrotation of the tibia on lateral radiographs.
The purpose of this study was to investigate the influence of tibial rotation on PTS measurement in lateral radiographs of the knee. We hypothesized that malrotation alters the measured PTS. Furthermore, as a result of the investigation, quality criteria for PTS measurement and a grading system for tibial malrotation on lateral radiographs should be defined.
Methods
The investigation was performed with a saw bone model of a human tibia (No. 116-20; Sawbones Europe). An osteotomy was performed on the saw bone model, comparable with an infratuberositary osteotomy to correct slope pathologies (Figure 1). An anterior opening was performed (0 mm, 5 mm, and 10 mm) to simulate 3 different PTS conditions, as increased PTS was more likely to be detected in patients with ACL insufficiency or ACL rerupture.

Anterior tibial osteotomy with an infratuberositary approach and a stable posteriorly positioned hinge for adapation of the posterior tibial slope to the 3 different testing conditions.
Long lateral radiographs of the tibial saw bone model were taken. An automated capturing technique was used. To avoid projection errors due to beam divergence, 2 radiographs were automatically captured, one with the central ray centered to the tibial plateau and a second one centered to the distal third of the tibia. The distance from source to target was 180 cm. The pictures were then automatically stitched together to display the full length of the lateral tibia. The experimental setup is shown in Figure 2. Additionally, a reference sphere with a diameter of 25 mm was used for calibration of the measurements.

Experimental setup: the saw bone model was positioned in front of the x-ray detector plate. A K-wire was fixed at the level of the distal tibia to indicate the change in rotation on a scale. The fixation of the saw bone to the baseplate allowed for adapation of the rotational alignment.
Three different PTS setups were tested, as shown in Figure 3.
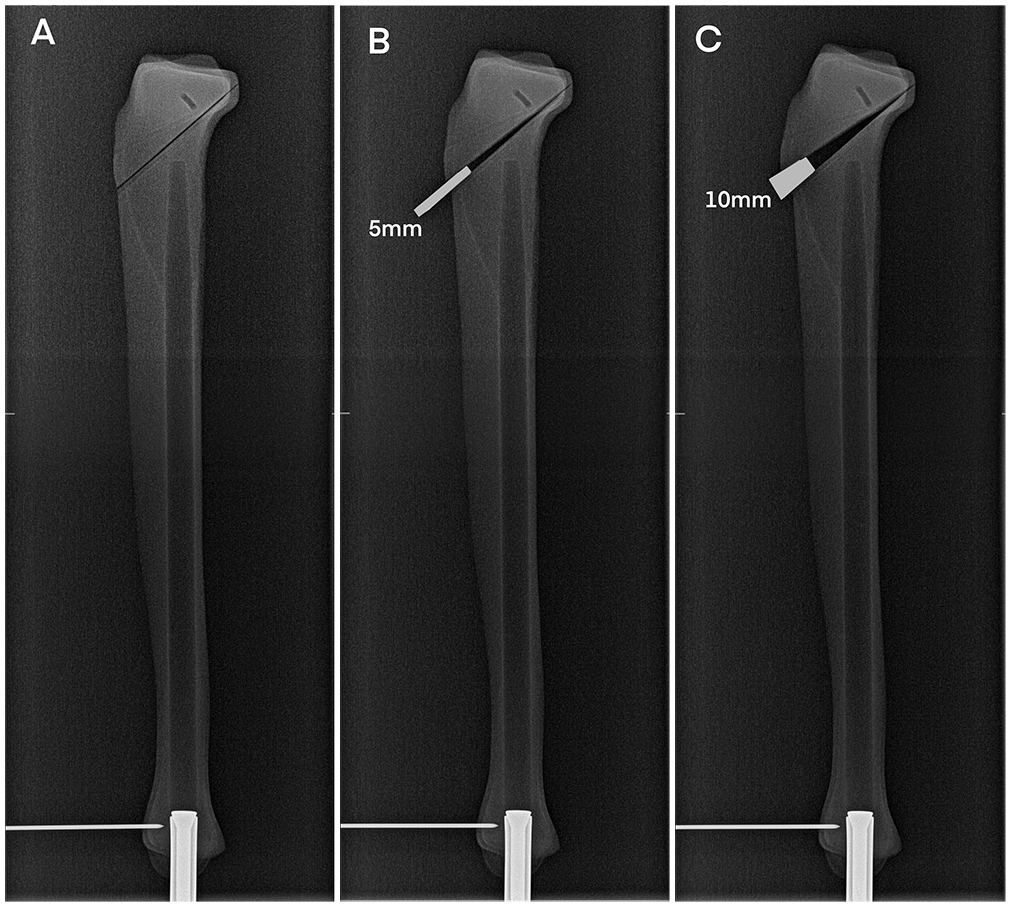
Three different posterior tibial slope setups were tested: (A) test series 1: with closed osteotomy; (B) test series 2: osteotomy with 5-mm opening; (C) test series 3: osteotomy with 10-mm opening.
All 3 testing series were tested from +12.5° of external tibial rotation (ETR) to −20° of internal tibial rotation (ITR) in steps of 2.5° between each measurement. Measurements were repeated twice, resulting in a total of 84 measurements. On each radiograph, the PTS was measured with the technique using the PAA and the MA as displayed in Figure 4.

Different methods for measuring the posterior tibial slope on lateral radiographs. Transparent angle, measurement of the tibial slope using the sagittal mechanical axis. White angle, proximal anatomic axis; measurement of the distance between the posterior tibial condyles.
The PAA, as described by Yoo et al, 24 was defined as a line connecting the midpoint of the tibial shaft 5 cm and 15 cm below the joint line. The angle between a tangential line to the medial tibial plateau and a line orthogonal to the PAA expressed the PTS.
Measurements of the PTS using the sagittal MA of the tibia were performed on a full-length tibial radiograph. The MA of the tibia in a sagittal plane was measured as a line connecting the midpoint of the medial tibial plateau and the midpoint of the tibial plafond. The angle between a tangential line to the medial tibial plateau and a line orthogonal to the MA expressed the PTS. 24
In addition, the distance between the medial and lateral posterior tibial condyles was measured on every lateral radiograph (in mm). Quality criteria for lateral radiographs were applied as follows: neutral rotation was defined as an exact superimposition of the posterior tibial condyles. This definition for a neutral rotation was used because this is the exact intraoperative position required for an anterior tibial closing-wedge osteotomy to correct the PTS. In our opinion, this represents the most consistent way, because the preoperative measurement and the surgical correction with an intraoperative radiographic control is based on the same radiographic projection of the lateral tibia. Any distance between the medial and lateral posterior tibial condyles as a result of tibial rotation was measured in millimeters, as described above. In addition, a clear visualization of the joint line (medial and lateral tibial plateau) was obligatory. If a radiograph failed to fulfill these criteria, it was repeated until it met the requirements described.
Radiographs were measured twice, blinded by previous results and with at least 6 weeks apart, to determine intra-observer, reliability (P.M.). In addition, radiographs were measured by a second specialist orthopedic surgeon, blinded by previous results, to determine inter-observe reliability (J.L.). All radiographs were analyzed by a trained orthopaedic knee surgeon (P.M. and J.L.). The PTS values measured by the 2 investigators were transformed into mean values before further analysis. Delta values were calculated from the raised mean values. The measurements were performed with a picture archiving and communication system system (Xero Viewer; Agfa HealthCare).
Statistical Analysis
Statistical analysis was performed with SPSS for Windows (Version 28; IBM Corp), descriptive data are shown as mean ± SD (with range). For parametric data, a 2-tailed t test was used. A linear correlation analysis (Pearson correlation) was applied to detect correlations between rotational alignment and the PTS measurement.
The intra- and interobserver reliability was calculated for the measurement of the PTS with the PAA and MA using the intraclass correlation coefficient (ICC). According to the ICC values, reliability was defined as poor (<0.5), moderate (0.5 ≤ ICC < 0.75), good (0.75 ≤ ICC < 0.90), or excellent (≥0.90).
Results
The results of the PTS measurements for the 3 different test series are shown in Table 1 and Figure 5.
Results of the Posterior Tibial Slope Measurements (in degrees) a

Values are presented as mean ± SD (range). ETR, external tibial rotation; ITR, internal tibial rotation; MA, mechanical axis; PAA, proximal anatomic axis; PTS, posterior tibial slope.
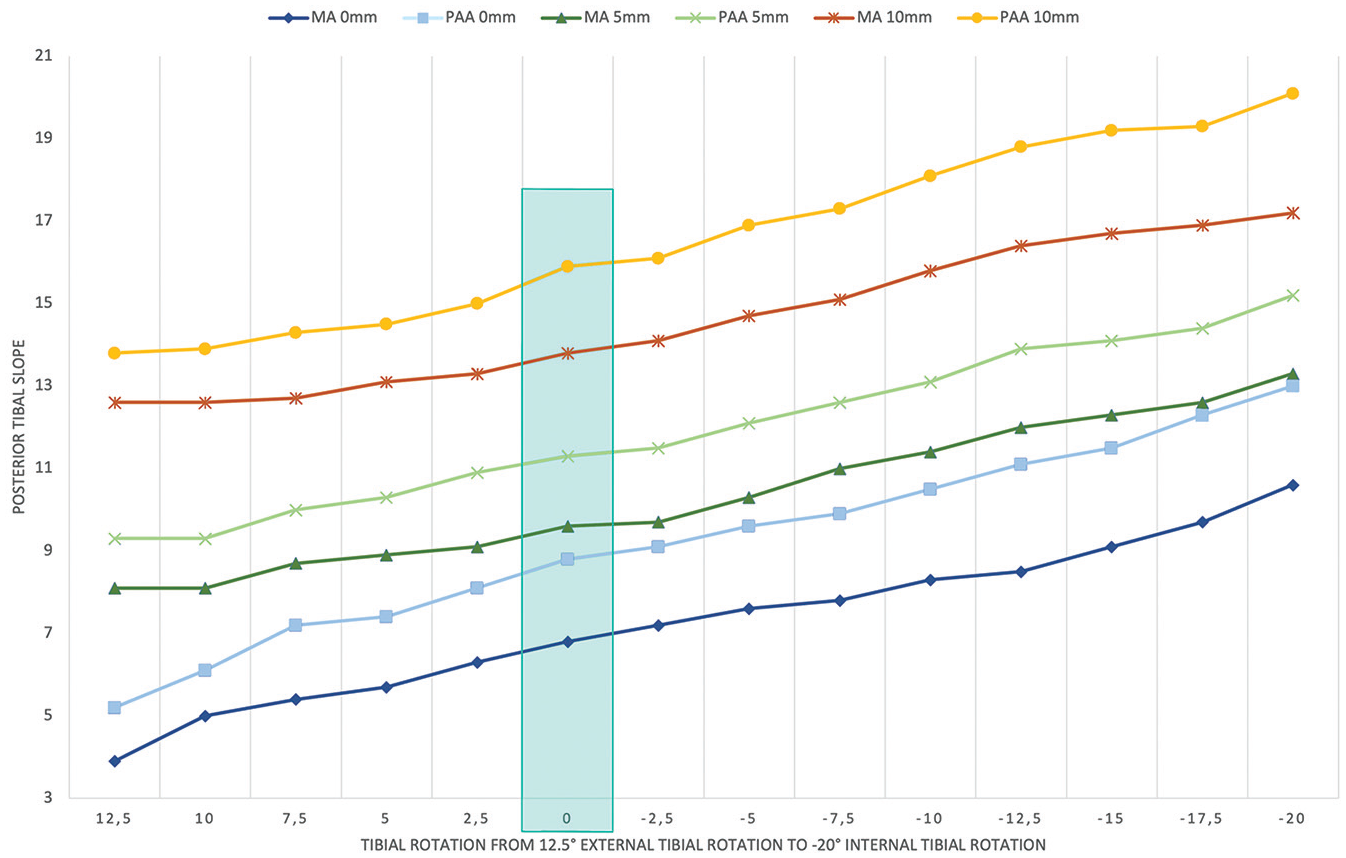
Influence of tibial rotation on posterior tibial slope measurement; test series 1 with closed osteotomy; test series 2 with 5-mm opening; test series 3 with 10-mm opening. Vertical box indicates the neutral rotation with exact superimposition of the posterior tibial condyles. MA, mechanical axis; PAA, proximal anatomic axis.
ETR of 12.5° resulted in a distance of 5 mm between the posterior tibial condyles in all 3 testing series. ITR of −20° resulted in a distance of 10 mm between the posterior tibial condyles in all 3 testing series. A visualization of test series 1 is displayed in Figure 6 showing an overlay of the radiographs with 12.5° ETR and −20° of ITR.

Visualization of the changes in radiographic projection of the tibial saw bone and the medial tibial plateau due to rotation. (A) Radiograph of saw bone (test series 1) with 12.5° of external tibial rotation (medial tibial plateau marked with dashed white line). (B) Radiograph of saw bone (test series 1) with −20° of internal tibial rotation (medial tibial plateau marked with continuous white line). (C) Overlay of the 2 radiographs to visualize the differences of the angulation of the medial tibial plateau.
A strong linear correlation could be found between the rotational alignment and the PTS measurement with the PAA and MA (P < .001) for all testing conditions; test series 1 with MA (R = 0.99); test series 1 with PAA (R = 0.98); test series 2 with MA (R = 0.99); test series 2 with PAA (R = 0.99; test series 3 with MA (R = 0.99); and test series 3 with PAA (R = 0.99).
An excellent intraobserver and interobserver reliability was found using the ICC for both PTS measurement techniques (Table 2).
ICCs for the Different Measurement Techniques a
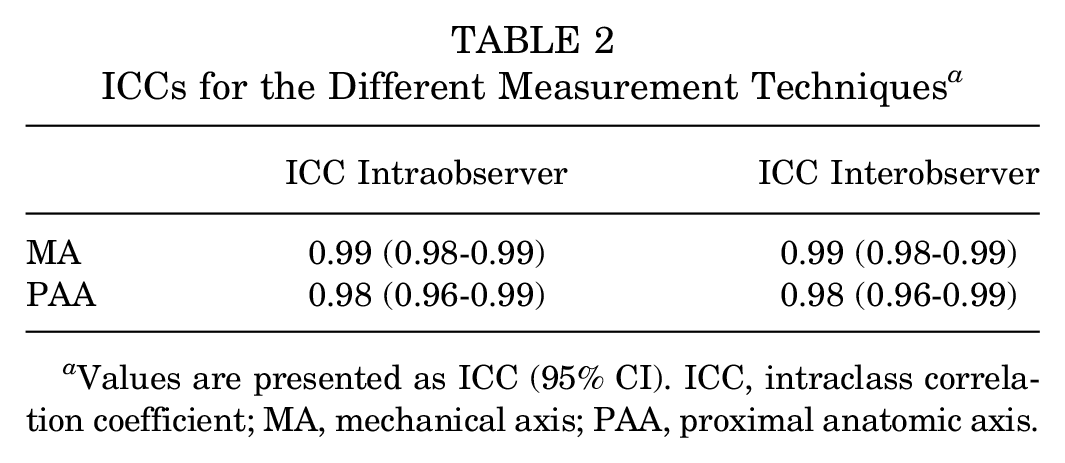
Values are presented as ICC (95% CI). ICC, intraclass correlation coefficient; MA, mechanical axis; PAA, proximal anatomic axis.
There was no significant difference in the mean PTS change between the 3 different testing conditions with rotational change from 12.5° of ETR to −20° of ITR (group 1 vs group 2: P = .09; group 1 vs group 3: P = .12; group 2 vs group 3: P = .34). The relative change of the PTS was consistent with and independent from the amount of PTS.
Change of PTS dependent on degree of rotation or distance between the posterior tibial condyles is displayed in Table 3.
Results of the Posterior Tibial Slope Measurements Dependent on Tibial Rotation or Distance Between the Posterior Tibial Condyles (in degrees) a
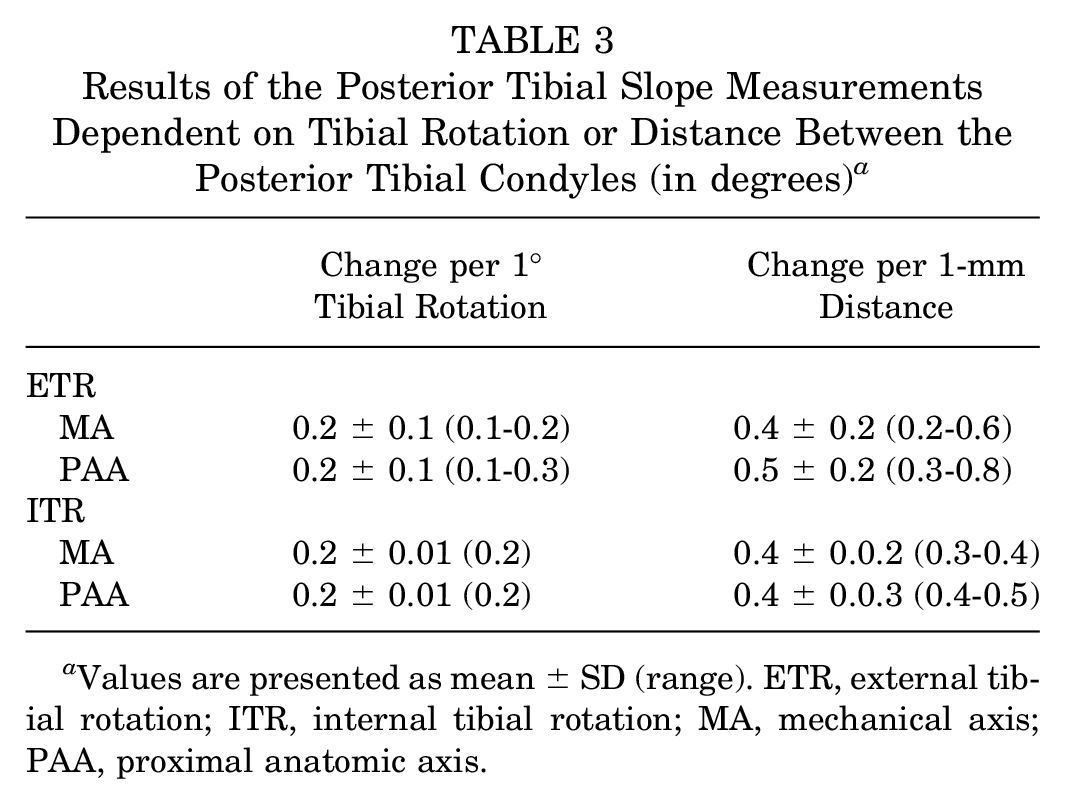
Values are presented as mean ± SD (range). ETR, external tibial rotation; ITR, internal tibial rotation; MA, mechanical axis; PAA, proximal anatomic axis.
Two degrees of ITR change was equivalent to a 1-mm increase in distance between the posterior tibial condyles. For ETR, every step of 2.5° of rotational change was equivalent to a 1-mm increase in distance between the posterior tibial condyles.
Discussion
The most important finding of this study was that tibial rotation strongly influenced PTS measurement on lateral radiographs irrespective of which axis was used for measurement (PAA or MA). A strong linear correlation between tibial rotation and PTS values could be detected. Therefore, the hypothesis of the study was confirmed. For a correct and reproducible measurement of the PTS, the posterior tibial condyles on lateral radiographs should be superimposed exactly, as malrotation of the tibia will lead to inaccurate measurements. This can be visualized in a 3D animation video which was added a supplemental file to this publication.
In the saw bone model used in this study, ETR led to an underestimation of the PTS, whereas ITR resulted in an overestimation of the PTS. Because of the technique commonly used to perform lateral radiographs, it can be expected that an internal tibial malrotation is likely to occur more often. Usually, the foot of the patient will be aligned parallel to the x-ray detector plate. An anatomic ETR can be observed in many individuals, as described by Waidelich et al. 19 This constitutional ETR will result in a relative internal rotation of the tibial head on the lateral radiograph, as the foot remains aligned as described above.
These observations are in line with the findings from Weinberg et al, 23 as they reported on a mean increase of the medial PTS of 1.3° and 1.1° for the lateral PTS, due to 10° of ITR. Previously published data by Kessler et al 11 demonstrated a comparable effect in their analyses. They showed an increase of the PTS as an effect of increasing ITR (0°-30° ITR). In contrast to the observations of this study, Weinberg et al found an increase of the medial and lateral PTS after increasing the ETR by 10°. Their measurements were performed with a 3-dimensioinal digitizer, creating digital representations of the proximal tibia. These representations were used to determine the PTS. This different method could explain the differences observed for ETR, in comparison with the current investigation. On lateral radiographs, tibial malrotation results in a shift of the reference points due to projection errors resulting in a change of PTS measurement (Figure 6). This effect can be different when measuring rotational changes in the model from a digitizer. Furthermore, it was not discussed in these studies whether the observed changes were dependent on the individual amount of PTS.11,23 In the current investigation, the changes observed were independent of the initial amount of PTS and were consistent throughout all 3 testing conditions.
When reporting on criteria to achieve reliable lateral radiographs, for example, Gwinner at al 8 recommended a distance of <5 mm between the posterior femoral condyles to allow a proper PTS assessment. When there was an overlap of ≥5 mm between the femoral condyles, they reported a significantly increased likelihood that measurements of both raters would result in a difference of >2°. But, as shown by Huettner et al, 9 interindividual differences of intra-articular torsion is common. This inevitably leads to the conclusion that well-aligned posterior femoral condyles do not guarantee correct rotational alignment of the posterior tibial condyles on lateral radiographs. Therefore, it seems advantageous to use the posterior tibial condyles as an anatomic landmark to detect tibial malrotation, as already advocated by Weinberg et al. 23 To obtain exact PTS measurements, it is recommended by the authors of the current paper that the projection of the posterior tibial condyles be perfectly superimposed without any distance. Rotational malalignment, especially ITR, is a common problem in daily clinical routine. ITR can be identified when the overlay of the fibular head behind the projection of the proximal tibia increases and the posterior edge of the medial tibial plateau rotates backward. ETR is indicated by a smaller overlay and increasingly free projection of the fibular head on the lateral radiograph. To quantify the degree of tibial malrotation, the authors of the current paper attempted to grade the changes observed in this saw bone model. With every 1 mm of increase in distance between the posterior tibial condyles, a mean change of 0.4° in PTS could be detected, irrespective of which axis was used as reference (PAA or MA). A 1-mm distance was equivalent to 2° of ITR and 2.5° of ETR. This should be kept in mind when judging the amount of PTS on lateral radiographs. For example, a distance of 2.5 mm between the posterior tibial condyles of the saw bone model on the lateral radiograph would result in an overestimation of the PTS by 1° in the case of ITR. Following these observations, we suggest that the gold standard for PTS measurement on a lateral radiograph be a full-length lateral radiograph of the tibia, aiming for an exact superimposition of the posterior tibial condyles, including a reference sphere to correct for any potential rotational malalignment.
Limitations
The investigations in this study were performed with only 1 saw bone model. It cannot be estimated to what extent different bony configurations off the tibial head or the tibial shaft may affect the measurement of the PTS in patients. However, as only relative changes of the measured angle values were reported, the results of this investigation can probably be adapted into a clinical setup, respecting patient-specific differences.
Further, to the best of our knowledge, there is no published information about the “true” neutral rotational alignment of the tibial head in the sagittal plane during dynamic loading. It could be expected that there is a broad interindividual variance of the tibial head rotational alignment while walking, which is probably mainly influenced by the constitutional ETR and highly patient specific. Therefore, the neutral rotation alignment of the tibial head in this study was defined as an exact superimposition of the posterior medial and lateral tibial condyle. This approach seems advantageous, as the preoperative measurement and the intraoperative correction were then performed in the exact same position, allowing a reliable and reproducible measurement and surgical correction of the PTS.
Conclusion
Tibial malrotation strongly influences PTS measurement on lateral radiographs. ETR leads to an underestimation, and ITR to an overestimation, of PTS. Every 1° of change in rotational alignment was equivalent to 0.2° of change in PTS measurement. For a reliable PTS measurement on lateral radiographs, the posterior tibial condyles should be superimposed exactly.
Footnotes
Final revision submitted October 18, 2024; accepted November 22, 2024.
The authors declared that there are no conflicts of interesting in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.