
Abstract
Background:
Extensor mechanism ruptures are career-threatening injuries for professional athletes, especially in the National Football League (NFL).
Purpose:
To determine the overall return to play (RTP) rate after extensor mechanism ruptures in the NFL, to identify factors influencing injury and return, and to compare postinjury outcomes between patellar tendon (PT) and quadriceps tendon (QT) tears.
Study Design:
Case series; Level of evidence, 4.
Methods:
A search of all available PT and QT injuries in NFL history was performed using publicly accessible data. Demographic and player performance data were compared to assess factors influencing the occurrence of either injury type and overall RTP. Among players that returned, mean performance data were compared at 1 and 2 full seasons before and after injury.
Results:
A total of 74 extensor mechanism injuries were identified, including 45 PT tears and 29 QT tears. The overall RTP rate after extensor mechanism ruptures was 56.8% with a median time to return of 11.3 months. No differences in RTP rates or timing were observed between PT and QT tears. Higher body mass index, lineman positions, and longer preinjury careers were significantly correlated with QT tears. Preseason injuries were associated with significantly lower RTP rates. Overall, athletes who returned played significantly fewer snaps and had lower approximate value in the first full season after return compared with 1 season before injury, with reductions in approximate value persisting into the second season after injury. PT tears were associated with worse deficits in approximate value at 1 season after injury compared with QT tears.
Conclusion:
Extensor mechanism ruptures in NFL athletes are associated with a low rate of RTP and an extensive recovery period. Athletes and staff should expect reductions in game play and performance in the first season after return, with worse performance deficits after PT tears compared with QT tears. This study highlights the challenges that professional athletes face in resuming play after extensor mechanism ruptures, emphasizing the need for improved prevention and rehabilitation measures tailored to these career-threatening injuries.
Keywords
The physically demanding nature of the National Football League (NFL) exposes players to heightened risks of all injuries, including debilitating knee extensor mechanism injuries. 15 Extensor mechanism ruptures, encompassing patellar fractures, patellar tendon (PT) tears, and quadriceps tendon (QT) tears, are rare yet severe injuries that usually require surgical intervention and extensive recovery periods. 8 QT tears are more prevalent in the general population, typically occurring after age 40 and often linked to medical comorbidities, whereas PT tears are associated with sports injuries in individuals <40 years of age5,7,24
Professional athletes, despite their peak physical condition, typically experience these injuries without prodromal symptoms, highlighting their unpredictable nature. 3 The primary mechanism for both PT and QT tears involves an eccentric overload of the extensor mechanism with the knee in a flexed position, most commonly during noncontact events.2,3,5,24,27 This can be seen in routine athletic actions including landing from a jump, suddenly stopping and changing direction while running, or attempting to maintain balance to prevent a fall.9,17 Overuse inflammation and microtrauma from repetitive high-power sports events are widely believed to contribute to the vulnerability of an otherwise healthy quadriceps or PT to rupture.3,5,11,12
A recent systematic review reported high return to play (RTP) rates of 88.9% for PT and 89.8% for QT tears in the general athlete population. 8 However, in professional athletes, the RTP rates decreased to 76.9% for PT tears among baseball, basketball, football, and soccer players and 70.9% for QT tears among football and soccer players, reflecting the unique challenges faced by elite athletes in their recovery. 8 NFL players, when compared with their counterparts in other professional sports, exhibit the worst postoperative outcomes, characterized by the lowest RTP rates and a significant decline in performance during the initial postoperative season. 14 Existing studies on RTP rates in NFL players have yielded varied results, ranging from 50% to 79% for PT tears2,8,13,14 and 50% for QT tears. 3 We suspect that the discrepancy among RTP rates for studies involving PT tears is likely attributed to differences in inclusion time frames across studies.
Despite previous research on this population, the overall RTP percentage and the factors influencing extensor mechanism injuries in NFL players remain poorly defined. This study aims to comprehensively evaluate the RTP dynamics in all NFL players who have experienced extensor mechanism injuries, with a particular focus on PT and QT tears. Our primary objective is to evaluate overall RTP rates after extensor mechanism injury, with secondary objectives focused on assessing performance metrics before and after injury and identifying demographic factors associated with extensor mechanism injury and RTP. Through this study, we hope to guide decision-making strategies regarding management of extensor tendon injuries in professional American football and encourage the development of prevention protocols.
Methods
Institutional review board approval was not required for this study because of the utilization of publicly available data. A previously established online database of NFL injury reports, 19 with records dating back to the 1920s, was utilized to identify potentially eligible records using the search terms “patella” and “quadriceps.” Inclusion criteria included professional American football athletes that sustained an isolated PT or QT tear while actively rostered in the NFL. Injuries that did not require operative repair were excluded. All reports were then verified by 2 study members (S.G.E. and H.C.) via reviewing press releases regarding each athlete’s injury details and surgical procedures from various online media sources. Injuries and surgeries were considered verified if they were consistent across ≥2 sources. Players that sustained >1 extensor mechanism injury on separate occasions were included more than once if the subsequent injury occurred in the contralateral limb. Players that sustained bilateral extensor mechanism ruptures in the same event were included as a singular injury. Sample size was determined by the availability of injury reports in the existing database.
Demographic characteristics and seasonal performance data were collected for all eligible players using a separate online database. 18 Demographic variables included age at injury, age at career start, body mass index (BMI), number of seasons in the NFL before injury, number of seasons in the NFL after injury, number of seasons in the NFL total, draft round, overall draft pick number, and the primary position played. Player positions were categorized into offensive and defensive positions, skilled positions (including quarterback running back, fullback, wide receiver, tight end, cornerback, linebacker, and safety), and linemen (both offensive and defensive; including offensive tackle, guard, center, defensive tackle, and defensive end). Successful RTP was defined as playing in ≥1 regular season NFL game after operative repair as of the end of the 2022-2023 regular season. Time to return was defined as the number of months between the athlete’s date of injury and the date of his first regular season game played after return. Among players that returned, game participation and performance data was catalogued from ≤4 seasons before the injury season and ≤4 seasons after the player returned, through the 2022-2023 regular season. Participation parameters included number of games played, games started, and snaps played (snap count) per season, while seasonal performance was measured via “approximate value.” Approximate value is a numerical metric that attempts to summarize the seasonal value of a given player via interpolation of position-specific data points. 1
Statistical analysis was performed to identify potential differences in characteristics between cohorts of PT and QT tears and between cohorts of athletes that did and did not RTP. Among athletes that returned to play, further analyses were performed to assess changes in seasonal participation and performance data at 1 and 2 full seasons before the injury season versus 1 and 2 full seasons after return from injury. Athletes who did not complete a full NFL season before injury were included in the analyses of characteristics and RTP rates but were excluded from comparisons of preinjury versus postinjury performance. Normality was determined for all continuous variables using the Shapiro-Wilk test. Continuous data were recorded as mean ± SD for parametric data and median (IQR) for nonparametric data. Categorical data were reported as counts and percentages. Unpaired t tests and Mann-Whitney U tests were used to assess unpaired continuous variables for parametric and nonparametric data, respectively. Paired t tests and Wilcoxon signed-rank tests were used for the comparison of in-game participation and performance data before and after injury, when appropriate. The Fisher exact test was used for comparison of categorical data. All statistical analyses were performed using GraphPad Prism Version 10.2.0 (GraphPad Software Inc) with a significance level of .05.
Results
A total of 74 extensor mechanism injuries in 72 NFL athletes occurring between the 1982-1983 and 2022-2023 seasons were included in this study, including 45 PT tears and 29 QT tears (Figure 1). Two players sustained bilateral PT tears during the same event while 2 players sustained a second PT tear in the contralateral limb during their first season back from their initial injury. The incidence of extensor mechanism injury was highest during the regular season (73.0%; 54/74), followed by preseason (24.3%; 18/74), and offseason (2.7%; 2//74).

Flow diagram of selection criteria for extensor mechanism injuries in the National Football League.
Descriptive characteristics for all athletes and by injury type are listed in Table 1. The median age at the time of injury was 26.0 years (IQR, 25.0-28.0) with a median BMI of 31.6 kg/m2 (IQR, 28.0-36.3). Among the 74 athletes, 37 (50.0%) played offensive positions, including 35 (47.3%) skilled offensive positions and 34 (45.9%) linemen positions. A breakdown of position counts is shown in Table 2, with defensive tackle being the most common position overall (13.5%; 10/74). Athletes played a median of 4.0 seasons (IQR, 1.8-5.0) in the league before injury and had a median total career length of 6.0 seasons (IQR, 4.0-8.0) in the NFL, as of the 2022-2023 season. Of the 59 (79.7%) players that were drafted, the median draft round was 3.0 (IQR, 1.0-4.0) with a median overall draft pick of 72.0 (IQR, 21.0-128.0).
Athlete Characteristics for All Extensor Mechanism Ruptures and Among Cohorts of Patellar Tendon Tears and Quadriceps Tendon Tears a

Values are presented as median (IQR) or n (%). Bold P values indicate a statistically significant difference (P < .05) between groups. Continuous data analyzed by the Mann-Whitney U test; categorical data analyzed by Fisher exact test. BMI, body mass index; NFL, National Football League; PT, patellar tendon; QT, quadriceps tendon.
As of the 2022-2023 season, including the injury season.
Among those who were drafted (n = 59).
Includes quarterbacks, running backs, fullbacks, wide receivers, tight ends, cornerbacks, safeties, and linebackers.
Position Counts for All Extensor Mechanism Ruptures and Among Cohorts of Patellar Tendon Tears and Quadriceps Tendon Tears a

Values are presented as n (%). C, center; CB, cornerback; DB, defensive back; DE, defensive end; DT, defensive tackle; FB, fullback; G, guard; LB, linebacker; PT, patellar tendon; QB, quarterback; QT, quadriceps tendon; RB, running back; S, safety; T, tackle; TE, tight end; WR, wide receiver.
Factors Influencing Injury Type
Compared with the PT group, the QT tear group played in the NFL significantly longer before injury (4.0 years vs 3.0 years; P = .04), had significantly higher BMI (35.2 kg/m2 vs 29.7 kg/m2; P = .004) more linemen (65.5% vs 33.3%; P = .009), and less skilled players (31.0% vs 57.8%; P = .03) (Table 1).
Return to Play
Overall, 42 athletes (56.8%) returned to play in ≥1 regular season game after injury, including 26 PT tears (57.8%) and 16 QT tears (55.2%) (Table 3). Rate of return was not significantly different between injuries (P≥ .99). Among the 42 athletes that returned, the median time to return was 11.3 months (IQR, 9.9-12.6 months; range, 7.6-26.2 months). Athletes with PT tears returned to play after a median of 11.4 months (IQR, 9.7-12.6), whereas players with QT tears returned after a median of 11.2 months (IQR, 9.9-12.7). This difference was not significant (P≥ .99). The median career length after return from injury was 2.0 seasons (IQR, 1.0-4.3). Of those who returned, 16 (38.1%) played just 1 additional season while 26 (61.9%) played in ≥2 additional seasons, as of the 2022-2023 regular season. No athletes returned to play during the same season in which they were injured, including players who were injured during the preseason. In total, 38 athletes (90.5%) returned to play in the season immediately after their injury season, while 4 athletes (9.5%) returned 2 seasons after their injury season.
RTP Rates and Timing for All Extensor Mechanism Ruptures and Among Cohorts of Patellar Tendon Tears and Quadriceps Tendon Tears a
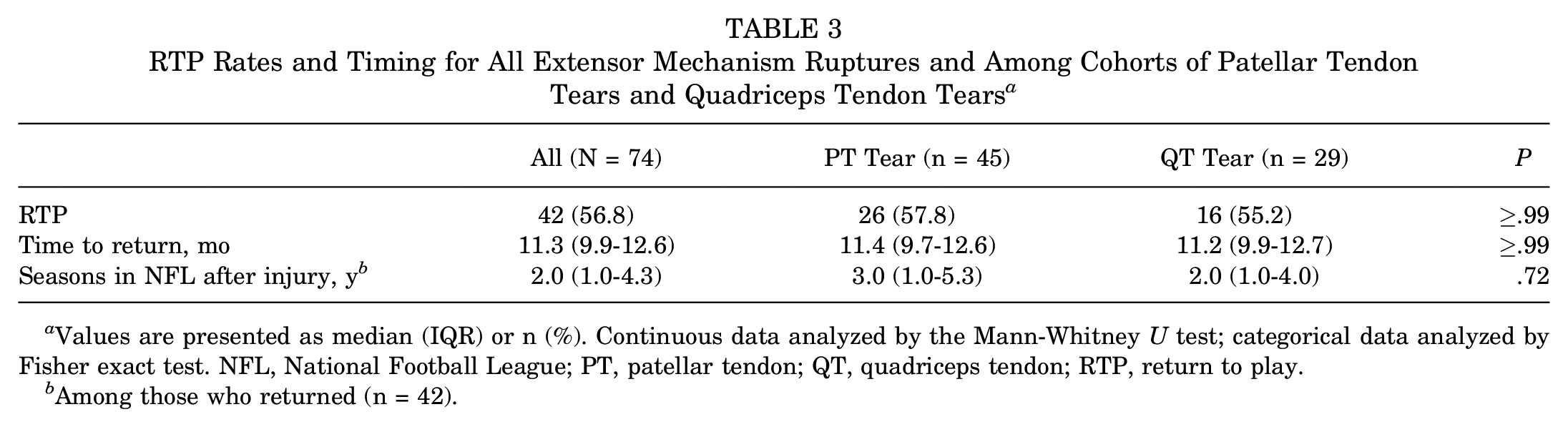
Values are presented as median (IQR) or n (%). Continuous data analyzed by the Mann-Whitney U test; categorical data analyzed by Fisher exact test. NFL, National Football League; PT, patellar tendon; QT, quadriceps tendon; RTP, return to play.
Among those who returned (n = 42).
Factors Influencing RTP
Table 4 displays descriptive characteristics for athletes who returned to play and those who did not. There were no significant differences in age at injury (P = .25), age at career start (P = .55), BMI (P = .51), number of seasons in the NFL before injury (P = .16), draft round (P = .20), overall draft pick (P = .09), number of undrafted free agents (P = .40), offensive positions (P = .82), skilled positions (P = .82), or linemen (P = .35) between groups. Preseason injuries were significantly associated with failure to RTP (11.9% vs 40.6%; P = .006). Of the 5 players who were injured during the preseason of their rookie season, only 1 went on to play a regular season game in the NFL, playing for a total of 5 games after injury. Unsurprisingly, players that returned to play had significantly longer NFL careers (median of 8.0 total seasons [IQR, 6.0-10.0] vs 4.5 total seasons [IQR, 1.3-5.8]; P < .001).
Athlete Characteristics Among Cohorts of Athletes Who Returned to Play in the National Football League and Those That Did Not a

Values are presented as median (IQR), n (%), or mean ± SD. Bold P values indicate a statistically significant difference (P < .05) between groups. Continuous data analyzed by the Mann-Whitney U test; categorical data analyzed by Fisher exact test. BMI, body mass index; NFL, National Football League; RTP, return to play.
Parametric continuous data analyzed using the unpaired t test.
As of the 2022-2023 season, including the injury season.
Among those who were drafted (n = 59).
Includes quarterbacks, running backs, fullbacks, wide receivers, tight ends, cornerbacks, safeties, and linebackers.
Performance After Injury
One Season Before Versus After Injury
Among the 42 athletes who returned to the NFL after extensor mechanism repair, 33 athletes played ≥1 full season before and after their injury season. Compared with the first full season before injury, these athletes played significantly fewer total snaps (mean ± SD of 558.6 ± 276.1 vs 656.8 ± 290.8; P = .03) and had a significantly lower median approximate value (4.0 [IQR, 2.0-5.5] vs. 6.0 [IQR, 2.0, 7.0]; P = .002) during the first full season after injury (Table 5). Overall, there were no significant reductions in the number of games played (P = .71) or games started (P = .09) between the first full season before and after injury. Among athletes that returned after PT tears, there were no significant reductions in the number of games played (P = .51), games started (P = .33), or snaps played (P = .17); however, approximate value was significantly decreased during the first postinjury season (median of 4.0 [IQR, 2.5-5.5] vs 6.0 [IQR, 3.5-7.5]; P = .03). Athletes that returned from QT tears did not have significant decreases in the number of games played (P = .91), games started (P = .16), snap count (P = .12), or approximate value (P = .07) in the first postinjury season compared with the first full season before injury.
In-Game Participation and Performance Averages From the First Full Season Before Injury Versus the First Full Season After Injury a

Values are presented as median (IQR) or mean ± SD. Continuous data analyzed by the Wilcoxon matched-pairs signed-rank test. Bold P values indicate a statistically significant difference (P < .05) between groups. PT, patellar tendon; QT, quadriceps tendon.
Parametric continuous data analyzed using the paired t test.
Two Seasons Before Versus After Injury
A total of 20 athletes played ≥2 full seasons after return from injury and 2 full seasons before the injury season (Table 6). Overall, there were no significant reductions in games played (P = .38), games started (P = .06), or snap count (P = .91); however, approximate value was significantly diminished during the second postinjury season when compared with 2 seasons before injury (median of 6.0 [IQR, 4.0-8.0] vs 3.0 [IQR, 2.0-6.0]; P = .048). Looking specifically at athletes who returned from PT tears, there were no significant differences in games played (P = .86), games started (P = .39), snap count (P = .62), or approximate value (P = .37). Likewise for the QT tear group, there were no significant reductions in games played (P = .16), games started (P = .08), snaps played (P = .36), or approximate value (P = .13) during the second full postinjury season when compared with 2 seasons before injury.
In-Game Participation and Performance Averages From the Second Full Season Before Injury Versus the Second Full Season After Injury a

Values are presented as median (IQR) or mean ± SD. Continuous data analyzed by the Wilcoxon matched-pairs signed-rank test. Bold P values indicate a statistically significant difference (P < .05) between groups. PT, patellar tendon; QT, quadriceps tendon.
Parametric continuous data analyzed using the paired t test.
Discussion
Extensor mechanism ruptures are rare but potentially career-threatening injuries for professional athletes.3,14,26,27 PT and QT tears are known to cause significant declines in game participation and on-field performance after return to football. 15 However, the overall rate of return and influencing factors after repair in NFL players remain poorly defined. The purpose of this study was to perform a comprehensive analysis of RTP from extensor mechanism ruptures in the NFL and to identify factors that may predispose players to injury or influence their odds of return.
In this cohort, representing the largest series of extensor mechanism ruptures in NFL players, we found a low overall rate of return (56.8%) with a median time to return of 11.3 months. We did not find significant differences between PT and QT tears with regard to rate of return (57.8% vs 55.2%; P≥ .99) or time to return (median of 11.4 months vs 11.2 months; P≥ .99). The median time to return for either injury was considerably longer than return times reported in the general athlete population, such as 9.5 months for PT tears and 4.6 months for QT tears. 8 There are numerous factors that contribute to the challenge of returning to play in the NFL. Physical demands are higher in American football than other sports, with intensive rehabilitation needed to return to the professional level. In addition to surgical repair and extensive recovery periods, RTP in the NFL necessitates the ability to overcome a yearly influx of fierce competition for a limited number of positions. Furthermore, the NFL offseason is the longest in length compared with other professional sports, 26 which contributes to the prolonged return times in our cohort, especially considering no athletes returned to play during the same season in which they were injured.
Overall, RTP was associated with fewer snaps played in the first postinjury season and lower approximate value at 1 and 2 seasons postinjury. PT tears had a bigger effect on performance in the first postinjury season, with a significant reduction in seasonal approximate value, whereas players returning from QT tears did not experience the same deficit. In the second postinjury season, however, reductions in approximate value had improved for the PT cohort and remained insignificant for the QT cohort. These findings suggest that despite early deficits in play time, players returning from QT tears were more likely to regain their on-field participation and performance long term. We did observe a near-significant decrease in the number of game starts for all athletes at 2 years after injury compared with before (median of 8 starts after injury versus 13.5 before; P = .06), despite similar numbers of games played (15 games after injury versus 15 before; P = .38) and snaps played (613.6 snaps after injury versus 637.3 snaps before; P = .91). Although not statistically significant, this decrease was more substantial for the QT tear group (median of 3 starts after injury versus 14 before; P = .08) compared with the PT tear group (median of 9 starts after injury versus 12 before; P = .39). Coaches are likely cautious with players recovering from extensor mechanism tears, potentially limiting their starting opportunities to avoid reinjury. This may have been more pronounced in the QT tear group due to the increased proportion of linemen and their unique physical demands, particularly in explosive blocking movements required every play.
Our results indicate that nearly 3 in 4 extensor mechanism ruptures occur during the regular season. This is in contrast to findings from similar studies of anterior cruciate ligament injuries in NFL athletes, which suggest that most injuries occur during the preseason or early in the regular season.6,23 Considering the median age of our cohort was 26 years at the time of injury, with a median of 4 years of experience in the league before injury, it is likely that as players age, they become increasingly susceptible to the accumulation of repetitive tendinous microtrauma that is endured over the course of the rigorous 17-week season. Although prodromal symptoms are typically absent in these athletes, close attention should be paid to new or undiagnosed knee pain involving the extensor mechanism, especially in players with several years of experience in the league or with a recent history of corticosteroid injection.2,3 We did find that players who sustained an extensor mechanism injury in the preseason had a significantly lower RTP rate. Although multiple explanations for this exist, the reality is that many players are released after preseason injuries. Preseason is a highly competitive time for NFL athletes who must showcase their abilities to earn a roster spot, as nonguaranteed contracts enable teams to release players with ease. 26
When characterizing players that returned versus those that did not, several trends emerged. Although not significant, we observed that athletes who returned were more likely to be drafted earlier. These findings are consistent across similar studies,2-4,6,22,26 highlighting that athletes who represent a higher value to their team before injury have a better chance at returning. Players who are drafted earlier tend to represent a higher monetary investment, making teams more likely to prioritize a successful recovery rather than simply finding a replacement. 6 Although RTP in the NFL is multifactorial, these trends demonstrate that successful RTP may be influenced more by a team’s preinjury investment in the player than the player’s postoperative outcomes. In our cohort, the median draft round for the RTP group was 2 with an overall pick of 64 versus a median draft round of 4 and overall pick of 113 in the no RTP group (P = .20; P = .09, respectively).
In this study, PT tears had a 57.8% return rate with a median return time of 11.4 months. Our results are most similar to the findings of Nguyen and Hsu 14 in their comparison of the effects of PT tears in various professional sports. In that study, 57.7% of NFL players with PT tears between 1995 and 2017 returned to play after a mean of 11.6 months. More favorable outcomes were suggested by Boublik et al 2 among 24 PT tears in NFL players between 1994 and 2004, with 79% successfully returning to play. Among the athletes who returned after PT tear in our cohort, no significant differences were observed in games played, games started, or snaps played during the first season back from injury when compared with 1 season before injury. Interestingly, these athletes had a higher median number of games played in the first full season after injury compared with a full season before injury (16.0 [IQR, 14.0-16.0] vs 15.0 [IQR, 10.5-16.0]; P = .51). This could be explained by the higher proportion of skilled positions in the PT group (P = .03), suggesting that teams may have a lower threshold for returning skilled players to the field immediately after being cleared from injury. Despite this, median approximate value remained significantly diminished for these athletes during their first season after injury (P = .03), which begs the question of whether returning players to a high level of play earlier may stunt their ability to recover their preinjury level of performance.
We found the rate of return after QT tears to be 55.2% with a median return time of 11.2 months. QT tears are twice as common as PT tears in the general population; however, they are rare in professional sports.5,7,27 As such, there are fewer articles discussing RTP after QT tears in the literature. A study of QT tears in NFL players by Boublik et al 3 found that 50% of players who suffered a QT tear between 1994 and 2004 were able to return to the league after surgical repair. A slightly higher RTP rate (63%) was reported by Rao et al 20 in a cohort of general athletes <40 years of age, which also noted no differences between competitive athletes and recreational athletes in terms of patient-reported outcomes, rate of RTP, or time to RTP. In our study, the median age at the time of injury for the QT cohort was 27.0 years, which is considerably younger than the mean age of >40 years in the general population.7,17 Athletes who injured their QT also had significantly higher BMI than those who injured their PT (median of 35.2 kg/m2 vs 29.7 kg/m2; P = .004). This difference is likely related to the difference in positional composition between groups, considering the QT group had significantly more linemen, who tend to have higher BMI. The predominance of QT tears among linemen was also demonstrated by Boublik et al. 3 In contrast to PT tears, we did not observe significantly reduced approximate value among QT tears in the first season after return, indicating that players recovering from QT tears were more likely to see earlier improvements in performance.
Limitations
This study has several inherent limitations. We aimed to assess NFL-specific outcomes after RTP rather than traditional orthopaedic outcomes. Assessment of performance in American football is complicated by a limited number of trackable in-game statistics for nonskilled players, such as linemen. To mitigate this, we utilized approximate value from Pro Football Reference, 1 which attempts to quantify the position-specific seasonal value for a given player over a single season. Although this is a somewhat novel metric, it has been used by numerous authors to compare performance before and after injury in NFL athletes.10,13,16,21,25 There is some degree of natural attrition of performance in players who have remained in the league for many years, which is not accounted for in this study. Given the nature of data collection from publicly accessible databases, we did not have access to official medical records or team reports. Therefore, we were unable to incorporate details regarding the severity of injury (partial vs complete tears), past medical history, surgical technique, or rehabilitation protocols in our analysis. We attempted to mitigate the risk of misinformation by confirming all injury and surgical details across multiple sources. Due to the limited availability of detailed media reports for older injuries and for less “popular” players, our sample size is likely an underrepresentation of the true prevalence of PT and QT ruptures in the NFL. In regard to selection bias, all athletes included in this study were male American football players; thus, our results are not generalizable to all professional athletes.
Conclusion
Extensor mechanism ruptures in NFL athletes are associated with a prolonged recovery and low return-to-play rates, regardless of tendon involved. Though performance declines are common, particularly after patellar tendon injuries, most players who return are able to maintain high levels of participation. Quadriceps tendon tears appear to be more common among linemen with higher BMIs and may show more favorable long-term performance recovery. These findings underscore the need for improved prevention strategies, tailored rehabilitation protocols, and informed expectations surrounding recovery and career longevity following these career-threatening injuries.
Footnotes
Final revision submitted April 29, 2024; accepted November 27, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: F.G.P. has received education payments from Rock Medical Orthopedics. R.F. has received education payments from Rock Medical Orthopedics. J.W.L. has received education payments from Rock Medical Orthopedics and hospitality payments from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.