
Abstract
Background:
The Anterior Cruciate Ligament–Return to Sport after Injury (ACL-RSI) scale measures psychological readiness to return to sport after an anterior cruciate ligament (ACL) injury or ACL reconstruction (ACLR). The 6-item short version of this scale has demonstrated psychometric properties similar to those of the original 12-item version.
Purpose:
To translate the short ACL-RSI scale into Thai and assess its psychometric properties via the COSMIN (COnsensus-based Standards for the selection of health Measurement INstruments) checklist.
Study Design:
Cohort study (Diagnosis); Level of evidence, 3.
Methods:
This prospective cohort study was conducted from August 2022 to April 2024. The Thai version of the short ACL-RSI scale was translated according to international guidelines. A psychometric evaluation was performed on athletes aged 18 to 50 years who had undergone ACLR at 6 months to 5 years prior. Participants completed the study questionnaires at baseline and 2 weeks later. The construct validity of the Thai version of the short ACL-RSI scale was evaluated by testing predefined hypotheses regarding its associations with other assessment tools. Reliability was assessed using internal consistency, test-retest reliability, and measurement error. Interpretability was assessed based on floor and ceiling effects and the minimal important change.
Results:
The short ACL-RSI scale was successfully translated into Thai. A total of 142 participants (mean age, 30.7 ± 8.9 years; 83.1% male) were included. Overall, 8 of 9 (88.9%) predefined hypotheses were confirmed, supporting good construct validity. The scale demonstrated good internal consistency (Cronbach alpha = 0.88) and test-retest reliability (intraclass correlation coefficient = 0.79). No floor or ceiling effects were observed. The minimal important change, which was calculated via a distribution-based method, was 9.2 points.
Conclusion:
The study demonstrated that the Thai version of the short ACL-RSI scale is a valid and reliable tool for assessing psychological readiness to return to sport after ACLR.
Keywords
Anterior cruciate ligament (ACL) injuries are prevalent among athletes and often necessitate surgery, followed by extensive rehabilitation. The primary objective of ACL reconstruction (ACLR) is to restore athletes to their preinjury level of sport performance. However, despite advances in surgical techniques and rehabilitation, a meta-analysis reported that only 65% of athletes return to their preinjury level after ACLR. 4 Psychological factors, particularly a fear of reinjuries, significantly hinder return to sport.4,7,30 Psychological readiness assessments should be integrated with physical conditioning to identify athletes who may require psychological interventions and to evaluate their readiness to return to sport.11,26
The Anterior Cruciate Ligament–Return to Sport after Injury (ACL-RSI) scale, developed by Webster et al 37 in 2008, is a psychological assessment tool designed to evaluate emotions, confidence in performance, and risk appraisal related to return to sport after an ACL injury or ACLR. The 12-item scale has been widely used in clinical and research settings to assess psychological readiness in injured athletes. Previous studies have shown a strong association between the ACL-RSI scale and rate of return to preinjury levels of sport after ACLR.5,15,32 Additionally, McPherson et al 25 demonstrated that younger patients with lower ACL-RSI scale scores face an increased risk of a second ACL injury after returning to sport.
In 2018, Webster and Feller 35 developed a short version of the ACL-RSI scale to reduce the burden on respondents and administrators in clinical settings. This shortened scale consists of 6 items while maintaining the ability to assess the same 3 dimensions of psychological readiness as the full version. The short ACL-RSI scale has demonstrated comparable psychometric properties to the 12-item version and can effectively differentiate between athletes who have returned to sport and those who have not. It has also been translated and cross-culturally adapted into several languages, demonstrating acceptable measurement properties.1 -3,34
This study aimed to translate the short ACL-RSI scale into Thai and evaluate its psychometric properties via the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) checklist. 28 We hypothesized that the Thai version of the short ACL-RSI scale (ACL-RSI-TH scale) would be a valid and reliable tool for assessing athletes’ psychological readiness to return to sport after ACLR.
Methods
Study Design
This prospective cohort study was conducted from August 2022 to April 2024 at Mahidol University. The study comprised 2 parts: (1) developing the short ACL-RSI-TH scale through translation and cross-cultural adaptation and (2) evaluating the validity and reliability of this scale in athletes who had undergone ACLR. The institutional review board approved the study protocol (322/2022), and all participants provided written informed consent.
Translation and Cross-cultural Adaptation
With permission from the original developers, the short ACL-RSI scale was translated into Thai following established guidelines for the cross-cultural adaptation of health status measures. 9 Forward translation was independently performed by 2 translators: an orthopaedic surgeon and a professional translator unfamiliar with the study. Discrepancies between their translations were resolved during a consensus meeting, resulting in a preliminary version of the short ACL-RSI-TH scale. This preliminary version was then back-translated into English by 2 professional translators with no prior knowledge of the study. All translations, along with the original scale, were reviewed to create a prefinal version of the short ACL-RSI-TH scale. The prefinal questionnaire was tested for comprehensibility with 30 patients who had undergone ACLR. As no comprehension issues were identified, no further modifications were needed, and the prefinal version was adopted as the final version of the short ACL-RSI-TH scale.
Evaluation of Psychometric Properties
The psychometric properties of the short ACL-RSI-TH scale were evaluated using the COSMIN checklist recommendations. 28 Eligible participants were athletes aged 18 to 50 years with a preinjury Tegner Activity Scale score of ≥5 and a history of unilateral primary ACLR performed between 6 months and 5 years prior. Patients were excluded if they had undergone bilateral ACLR or multiligament reconstruction, lacked sufficient proficiency in Thai, or had medical conditions affecting questionnaire comprehension.
The participants were instructed to complete 2 sets of questionnaires over a 2-week period. Patient recruitment and baseline data collection were conducted in an outpatient setting during postoperative follow-up visits of the patients. During the initial visit, they completed the first set, which included the short ACL-RSI-TH scale, the Injury–Psychological Readiness to Return to Sport (I-PRRS) scale, the Tampa Scale for Kinesiophobia (TSK), the International Knee Documentation Committee subjective knee form (IKDC-SKF), the Knee injury and Osteoarthritis Outcome Score (KOOS), and the Simple Knee Value (SKV). The estimated time to complete all patient-reported outcome measures (PROMs) was 15 minutes. A stamped, preaddressed envelope containing the second set of questionnaires, which included the short ACL-RSI-TH scale and the Global Rating of Change (GRoC) scale, was provided for completion 2 weeks later. The 2-week interval was considered sufficient to minimize recall bias for test-retest reliability.28,33
Questionnaires
The participants completed the Thai versions of the following assessment tools:
Validity
The construct validity of the short ACL-RSI-TH scale was evaluated according to the COSMIN checklist recommendations. 28 This evaluation involved testing a priori hypotheses regarding the scale’s associations with other assessment tools (Table 1). The Spearman rank correlation coefficient (r s) was used to assess the strength of these correlations, which was categorized as small (0.10-0.29), medium (0.30-0.49), or large (0.50-1.00). 12 Construct validity was considered acceptable if at least 75% of the a priori hypotheses were confirmed.
A Priori Hypotheses Concerning Correlations Between Short ACL-RSI-TH Scale Score and Scores of Other Questionnaires a

ACL-RSI-TH, Thai version of Anterior Cruciate Ligament–Return to Sport after Injury scale; IKDC-SKF, International Knee Documentation Committee subjective knee form; I-PRRS, Injury–Psychological Readiness to Return to Sport; KOOS, Knee injury and Osteoarthritis Outcome Score; SKV, Simple Knee Value; TSK, Tampa Scale for Kinesiophobia.
Reliability
The reliability of the short ACL-RSI-TH scale was assessed using 3 measurement properties: internal consistency, test-retest reliability, and measurement error.
Interpretability
Floor and ceiling effects were evaluated to determine if >15% of participants had the lowest or highest possible score, respectively, as these effects can impact a scale’s validity and reliability. 33 The minimal important change (MIC) was calculated via a distribution-based formula proposed by Norman et al, 29 which is 0.5 times the SD of all participants at baseline.
Statistical Analysis
Descriptive statistics summarized the patient data and outcomes of the assessment tools. Continuous data are presented as means and SDs, whereas categorical data are displayed as frequencies and percentages. All statistical analyses were performed with PASW Statistics for Windows (Version 18.0; IBM). A Bland-Altman plot was generated via MedCalc for Windows (Version 22.023; MedCalc Software). A P value of <.05 was considered statistically significant.
Results
Translation and Cross-cultural Adaptation
The short ACL-RSI scale was successfully translated into Thai. No items or responses required cross-cultural adaptation. Pretesting of the translated scale revealed no comprehension issues among the participants.
Patient Characteristics
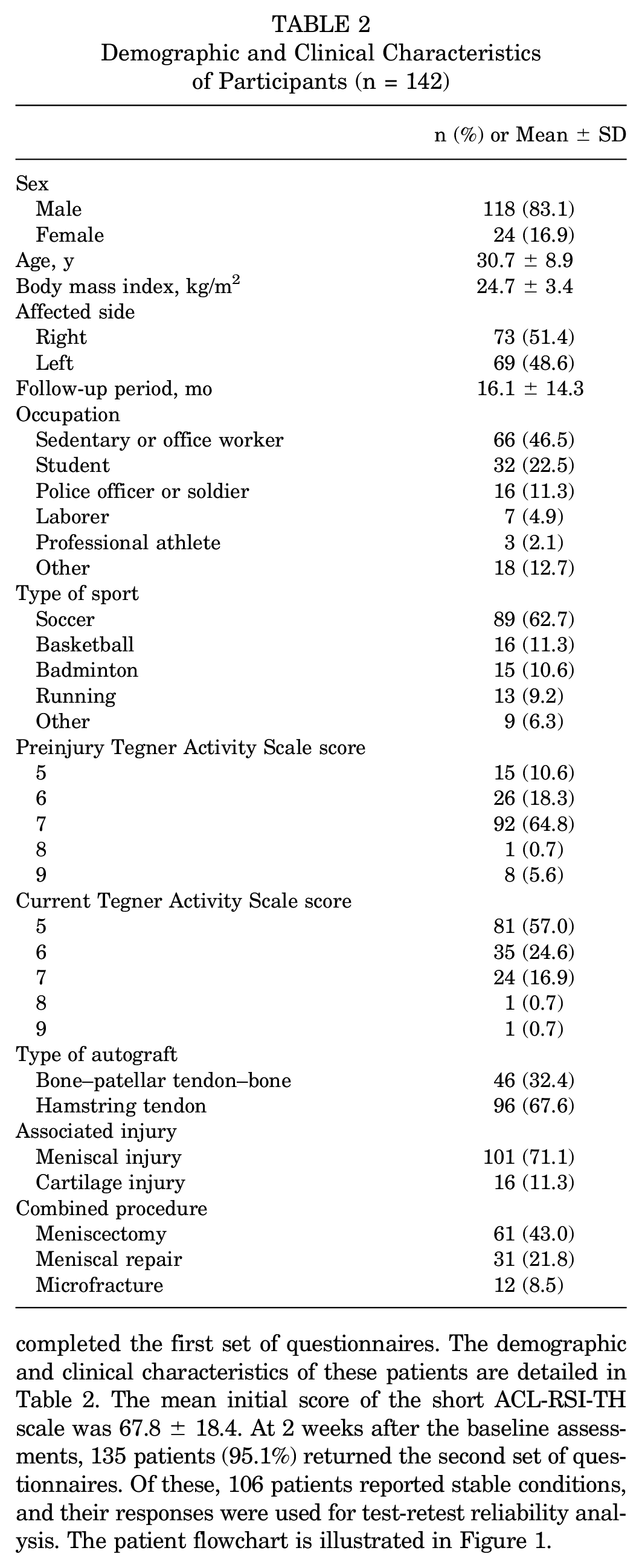
Between August 2022 and April 2024, a total of 142 patients (mean age, 30.7 ± 8.9 years; 83.1% male) completed the first set of questionnaires. The demographic and clinical characteristics of these patients are detailed in Table 2. The mean initial score of the short ACL-RSI-TH scale was 67.8 ± 18.4. At 2 weeks after the baseline assessments, 135 patients (95.1%) returned the second set of questionnaires. Of these, 106 patients reported stable conditions, and their responses were used for test-retest reliability analysis. The patient flowchart is illustrated in Figure 1.
Demographic and Clinical Characteristics of Participants (n = 142)
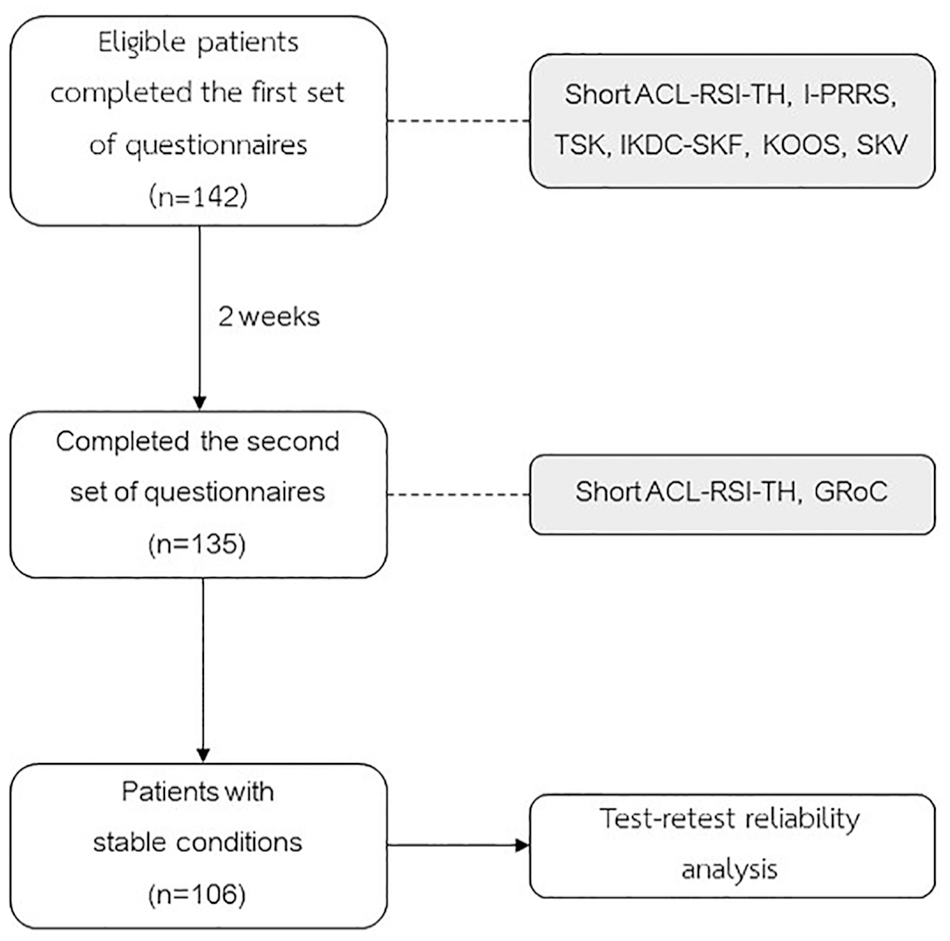
Flowchart of patient enrollment and participation. ACL-RSI-TH, Thai version of Anterior Cruciate Ligament–Return to Sport after Injury scale; GRoC, Global Rating of Change scale; IKDC-SKF, International Knee Documentation Committee subjective knee form; I-PRRS, Injury–Psychological Readiness to Return to Sport scale; KOOS, Knee injury and Osteoarthritis Outcome Score; SKV, Simple Knee Value; TSK, Tampa Scale for Kinesiophobia.
Validity
The correlations between the short ACL-RSI-TH scale and other PROMs are shown in Table 1. Overall, 8 of 9 (88.9%) a priori hypotheses were confirmed, demonstrating good construct validity of the short ACL-RSI-TH scale.
Reliability
The short ACL-RSI-TH scale showed high internal consistency, with a Cronbach alpha of 0.88. The reliability results are presented in Table 3, with an ICC of 0.79 (95% CI, 0.67-0.86), indicating good test-retest reliability. The Bland-Altman analysis for agreement between measurements is displayed in Figure 2.
Reliability of Short ACL-RSI-TH Scale Among Patients With Stable Conditions (n = 106) a

Patients with stable conditions based on the Global Rating of Change scale score at the 2-week time point. ACL-RSI-TH, Thai version of Anterior Cruciate Ligament–Return to Sport after Injury scale; ICC, intraclass correlation coefficient; SDCgrp, smallest detectable change at the group level; SDCind, smallest detectable change at the individual level; SEM, standard error of measurement.

Bland-Altman plot evaluating the test-retest reliability of the Thai version of the short Anterior Cruciate Ligament–Return to Sport after Injury (ACL-RSI-TH) scale.
Interpretability
No floor or ceiling effects were observed for the total score of the short ACL-RSI-TH scale. However, for individual items, 15.5% of patients reported the maximum score for item 1, whereas 29.6% reported the maximum score for item 5 (Table 4). The MIC for the short ACL-RSI-TH scale was calculated to be 9.2.
Floor and Ceiling Effects and MIC for Short ACL-RSI-TH Scale a

ACL-RSI-TH, Thai version of Anterior Cruciate Ligament–Return to Sport after Injury scale; MIC, minimal important change.
Discussion
The short ACL-RSI-TH scale was successfully developed through translation and cross-cultural adaptation from the original English version. Its psychometric properties were evaluated according to the COSMIN checklist recommendations in patients who had undergone ACLR. The major findings of our study demonstrated that the scale has good validity and reliability in assessing psychological readiness to return to sport in this population. Overall, 8 of 9 (88.9%) predefined hypotheses regarding the scale’s associations with other PROMs were confirmed. The scale demonstrated good internal consistency (Cronbach alpha = 0.88) and test-retest reliability (ICC = 0.79). No floor or ceiling effects were observed. The MIC was 9.2 points.
The short ACL-RSI-TH scale showed good construct validity, with 88.9% of the a priori hypotheses confirmed. The strongest correlation was observed between the short ACL-RSI-TH scale score and the I-PRRS scale score (r s = 0.65). Both tools assess psychological readiness in injured athletes, but while the I-PRRS scale is a generic tool applicable to various injuries, the short ACL-RSI scale is specific to ACL injuries. Similarly, the Dutch version of the short ACL-RSI scale has shown a large correlation (r s = 0.63) between the performance domain score of the ACL-RSI scale and the I-PRRS scale score but a medium correlation (r s = 0.45) for its emotion domain. 34 Another psychological assessment tool used in the current study, the TSK, demonstrated a significant correlation with the short ACL-RSI-TH scale score (r s = −0.34); however, this did not confirm the corresponding hypothesis. In contrast, the Brazilian version of the short ACL-RSI scale has shown a stronger correlation with the TSK (r s = −0.45). 2
The short ACL-RSI-TH scale also showed significant correlations with other knee-specific PROMs, particularly with the KOOS quality of life subscale and the SKV. The KOOS quality of life subscale includes 4 items that may relate to the 3 domains assessed by the short ACL-RSI-TH scale. A validation study of the Arabic version of the short ACL-RSI scale also utilized the KOOS, with the KOOS quality of life subscale demonstrating the highest correlation (r s = 0.59), comparable to the correlation found in the present study (r s = 0.57). 3 The strong correlation between the short ACL-RSI-TH scale score and the SKV score highlights the importance of psychological factors in patients’ perceptions of healthy knee function.
The internal consistency of the short ACL-RSI-TH scale was high, with a Cronbach alpha of 0.88. This value is consistent with those of other language versions, which range from 0.73 to 0.92.1 -3,34 The test-retest reliability of the short ACL-RSI-TH scale was also high, with an ICC of 0.79, although it was slightly lower than the ICC values reported for other versions (0.85-0.89).2,3,34
No floor or ceiling effects were observed for the short ACL-RSI-TH scale, which agrees with the findings for other versions.2,3,34 The MIC of the short ACL-RSI-TH scale, which was calculated via a distribution-based approach, was 9.2. This MIC was higher than the SDC at both the individual and group levels, indicating that a change in the score of ≥9.2 is meaningful and not caused by measurement error. Webster and Feller 36 reported an MIC of 15.1 for the short ACL-RSI scale using an anchor-based method.
Limitations
This study has several limitations. First, most participants were male, which could influence the findings. Previous studies have reported higher ACL-RSI scale scores in male athletes after ACLR,21,27 although Cronström et al 13 found no differences between the sexes. Second, the study did not include athletes who had undergone revision ACLR. A matched case-control study demonstrated that patients with revision ACLR scored lower on the ACL-RSI scale than those with primary ACLR. 14 Finally, a responsiveness analysis was not performed. Webster and Feller 36 showed comparable responsiveness between the short and full versions of the original ACL-RSI scale.
Conclusion
Our study demonstrated that the short ACL-RSI-TH scale has good validity and reliability for assessing psychological readiness to return to sport after ACLR.
Footnotes
Acknowledgements
The authors gratefully acknowledge the original authors of the short ACL-RSI scale for granting permission to translate the English version into Thai. The authors also thank Panisa Khaminta for her assistance with data collection and statistical analysis.
Final revision submitted September 5, 2024; accepted November 22, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by a research grant (R016531066) from the Faculty of Medicine Siriraj Hospital, Mahidol University. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Siriraj Institutional Review Board (322/2022).