
Abstract
Background:
The Lysholm Knee Score (LKS) is a widely utilized patient-reported outcome measure for knee injury patients, due to its robust psychometric properties. It has been translated and validated in several languages, but it has not been translated into Persian.
Purpose:
To perform psychometric validation and cultural adaptation for the Persian version of the LKS (P-LKS) in patients with anterior cruciate ligament tears.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Method:
The LKS was translated into Persian using a forward-backward translation procedure. To assess the reliability and validity of the P-LKS, responses were gathered from 100 consecutive patients (mean age, 35 ± 13 years; 91 male and 9 female). These participants also fulfilled the Persian versions of the International Knee Documentation Committee Subjective Form (IKDC-SF) and the 36-Item Short Form Health Survey (SF-36). Construct validity was evaluated by correlating the scores from the P-LKS with those from the Persian IKDC-SF and SF-36. Reliability was determined by examining test-retest reliability and internal consistency. Additionally, floor and ceiling effects, as well as measurement errors, were assessed. The Bland-Altman method was utilized to evaluate absolute agreement.
Results:
Construct validity was strong, as >80% of the predetermined hypotheses regarding correlations between the P-LKS and other measures were verified. The P-LKS exhibited a high correlation with the Persian IKDC-SF (r = 0.92) and the physical component of the Persian SF-36 (r = 0.85). Bland-Altman analysis indicated no systematic bias among the test and retest phases. The test-retest reliability and internal consistency for the P-LKS were excellent (ICC = 0.97; Cronbach alpha = 0.88). Floor and ceiling effects for the overall score of the P-LKS were <15% (0% and 2%, respectively). The standard error of measurement was 1.04; the minimal detectable change at the individual level was 2.88, and at the group level, it was 0.29.
Conclusion:
The study demonstrated that the P-LKS successfully preserved the attributes of the original version. It can be regarded as a reliable tool for Persian-speaking patients with complete anterior cruciate ligament tear.
Keywords
Knee injuries are frequently associated with participation in physical activities, notably among adolescents and athletes. 20 The incidence of anterior cruciate ligament (ACL) injuries is about 0.04% annually among various nations. 31 Knee joint complications can lead to a variety of symptoms and significantly affect an individual's functionality and quality of life. Evaluations can draw on both symptoms and clinical examination findings to determine the clinical outcomes for individuals with knee injuries. Various questionnaires have been developed to evaluate knee function, serving as important tools in both clinical settings and research.4,14,23,24,28,33,39,43 For assessing general knee injuries in Persian-speaking patients, the Persian version of the International Knee Documentation Committee Subjective Form (IKDC-SF) is frequently utilized. 18
The Lysholm Knee Score (LKS) is a frequently utilized patient-reported questionnaire designed to evaluate outcomes for individuals with knee complications. LKS, introduced in 1982 and subsequently revised in 1985, aims to assess the functional condition of patients after ACL surgery. 28 Its reliability, validity, and responsiveness have been proven for a wide range of knee issues, such as injuries to the ACL with or without meniscal injury,6,7,19 patellofemoral disorders,11,12,16,36 cartilage disorders, 26 knee arthroplasty, 42 and even the assessment of healthy knees. 8 This instrument has been validated and culturally adapted into numerous languages, demonstrating great validity and reliability.2,11,17,25,46
The LKS has some advantages compared with other knee outcome scores. While some knee assessment tools only focus on a subgroup of knee injuries, such as the Oxford Knee Score, which is specific to knee osteoarthritis, or the IKDC-SF, which focuses on knee ligament evaluation, the LKS offers broader utility.4,14,24,43 Additionally, the Western Ontario and McMaster Universities Osteoarthritis Index and the Knee injury and Osteoarthritis Outcome Score contain 24 and 42 questions, respectively, and can take between 5 and 10 minutes to complete. The LKS is more concise, with 8 items, allowing quicker completion time.10,13,28
The LKS serves as a comprehensive assessment instrument that mirrors the total outcome of knee function and level of physical activity. Prior to this study, an official cultural adaptation and Persian translation of the LKS did not exist. The Persian language often referred to as “Farsi,” is spoken by a significant number of people across various countries, including Iran, Tajikistan, Afghanistan, Azerbaijan, and several Persian Gulf states such as Bahrain, Iraq, and the United Arab Emirates.40,41 When applying these questionnaires across culturally diverse populations, it is crucial to assess the psychometric features of the instruments instead of merely translating their content. This approach is necessary to prevent errors in evaluation that could be caused by cultural disparities, especially for LKS, which is a self-report questionnaire.9,34
The goal of this study was to perform a cross-cultural adaptation of the original English LKS into Persian (P-LKS) and assess the validity and reliability of this version among Persian-speaking patients with ACL injurie. We hypothesized that the P-LKS would demonstrate good validity and reliability in this patient population.
Methods
In this study, the Consensus-based Standards for Measurement Instruments (COSMIN) guidelines for research on measurement tools were followed. 21 The study protocol received approval from our university's ethics committee, and written informed consent was obtained from all participating patients.
Study Patients
This study focused on patients diagnosed with an ACL tear and persistent knee problems and was carried out at a tertiary hospital from July 2022 to August 2023. Confirmatory diagnoses were made through clinical evaluations and magnetic resonance imaging. Patients had to be aged <70 years, Persian speaking, and literate to be included in the study. Exclusion criteria encompassed being <15 years old, undergoing interventions within the test-retest interval, and having infections, inflammatory arthritis, posttraumatic arthritis, or psychiatric or neurological disorders. All patients completed both steps of the questionnaire before their surgery. Eventually, all patients underwent surgical treatment for their ACL injuries. According to Mo et al, 29 Walter et al, 45 and Mundfrom et al, 32 a sample size of ≥100 individuals was considered sufficient for conducting validity and reliability evaluations. In total, 100 consecutive patients with ACL injuries qualified for inclusion and consented to participate in the questionnaire. No patients were lost during the follow-up period.
LKS Scales
The LKS is a questionnaire comprising 8 items, initially created to assess the function of the knee after knee ligament damage. It was later also proven reliable for assessing other knee-related issues.6,8,12,16,26,36,42 It evaluates various aspects such as pain, support type, instability, locking, swelling, limping, the capability of walking upstairs, and squatting. A total score between 0 and 100 is derived from these items, where a higher score suggests fewer symptoms and greater functional capacity (scores are categorized as 91-100 = excellent, 84-90 = good, 65-83 = fair, <65 = poor). 43
Translation Procedure
Before initiating the study, the authors sought permission from the original developers of the LKS to translate and adapt the questionnaires. Forward-backward translation technique was employed, as developed by Guillemin et al, 22 to translate the questionnaire into Persian 3 ; this involved a conversion of the questionnaire from English to Persian, performed separately, by both a professional translator and an expert knee surgeon (F.V.). These 2 versions were merged into a preliminary Persian version after thorough discussion and agreement between the translators. A reverse translation back into English was similarly completed by a second professional translator and an experienced knee surgeon (A.S.V.) following the same protocol. An expert panel, comprising both translators and orthopaedic surgeons (F.V. and A.S.V.) and an additional researcher (I.M.O.) who had not participated in the translation, reviewed the preliminary version. They ensured all items were faithfully consistent with the original English text, making any necessary adjustments. This rigorous review process led to the finalization of the translation.
The final phase of the project included conducting a pretest of the translated questionnaire with a group of patients. Participants completed the survey, followed by interviews to discuss their interpretations of each question and the corresponding answers to ensure that the meanings of both the questions and the responses were clearly understood. This step verified that the translated version maintained its functional equivalence in a practical setting. The expert panel reviewed any items misinterpreted or altered by ≥15% of the respondents. 3 Through this process, the Persian translation and cultural adaptation of the LKS scales was finalized.
The IKDC-SF
Alongside the P-LKS scales, participants filled out the Persian version of the IKDC-SF. 24 This tool assesses the effect of a knee problem on a patient’s physical symptoms, functional limitations, and sports activities. The IKDC-SF contains 10 questions covering symptoms, overall function, and sports participation domains, with the total score being on a scale of 0 to 87, where higher scores represent fewer symptoms and greater functionality. The Persian version has been officially validated among Persian-speaking patients experiencing knee problems. 18
The 36-Item Short Form Health Survey
The 36-Item Short Form Health Survey (SF-36) consists of 35 questions categorized across 8 domains: physical functioning, physical role limitations, bodily pain, general health perceptions, energy/vitality, social functioning, emotional role limitations, and mental health. The scores range from 0 to 100, with higher scores indicating better health status. Additionally, the physical component score is the sum of physical functioning, physical role functioning, bodily pain, and general health perception subscales. Similarly, the mental component score is constructed from the sum of vitality, social functioning, emotional role functioning, and mental health subscales. 48
Data Collection
Patients at our orthopaedic clinic filled out the P-LKS, SF-36, and IKDC-SF questionnaires in the waiting room during their appointment, reflecting their symptoms at that moment. We compared the current P-LKS scores against those from the IKDC-SF and SF-36 to check the criterion validity. Furthermore, to analyze test-retest reliability, the same individuals were requested to answer the questionnaires again 14 days later.
Floor and Ceiling Effects
The presence of floor and ceiling effects was evaluated. These effects were identified when >15% of participants attained the minimum or maximum possible score.6,7,38
Reliability
Reliability indicated how well participants could be differentiated from one another despite the presence of measurement errors. To assess reliability, different aspects, such as internal consistency and test-retest reliability, were examined, along with measurement errors. The Bland-Altman approach was utilized to assess absolute agreement, highlighting the degree of consistency in repeated measurements. 5
Validity
The construct validity of the P-LKS was evaluated by analyzing its correlation with other established questionnaires. According to COSMIN guidelines, 5 predetermined hypotheses were designed regarding the strength of the correlations between the P-LKS, each SF-36 subscale, and the IKDC-SF scale. 21 In the Chinese version of the LKS scale, Wang et al 46 identified a correlation of 0.837 with the IKDC-SF scale. Consequently, the current study anticipated a correlation of 0.7 or higher between the P-LKS and the IKDC-SF scale. As the P-LKS is primarily focused on assessing physical functioning rather than emotional aspects, it was expected to show strong correlations with the physical component of the SF-36. Deviandri et al 17 reported a correlation of 0.66 between the Lysholm score and the physical component of the SF-36. Based on these results, the current study anticipated a correlation of 0.6 or higher between the P-LKS and the physical component of the SF-36. Conversely, lower correlations were expected between the P-LKS and the mental component of the SF-36. Construct validity is considered strong when ≥75% of the predefined hypotheses are approved. 44
Statistical Analysis
The statistical analysis was conducted using SPSS Version 22 (IBM Corp). Categorical variables were summarized using frequencies and percentages, while continuous variables were described by the mean ± SD and median [IQR]. To evaluate the relationship between patient scores on the P-LKS, SF-36, and IKDC-SF scales, both Spearman and Pearson correlation coefficients were applied. Correlations were categorized as poor (0 ≤ r ≤ 0.2), fair (0.2 ≤ 0.4), moderate (0.4 ≤ 0.6), very good (0.6 ≤ 0.8), or excellent (0.8 ≤ 1.0).
47
The intraclass correlation coefficient (ICC) was used to assess test-retest reliability, with values ≥0.9 deemed excellent, 0.75≤ICC<0.9 rated as good, and 0.5 ≤ ICC <0.75 considered moderate.
27
For the P-LKS scale, internal consistency was evaluated by calculating Cronbach alpha (α), with a score ≥0.7 reflecting good internal consistency, according to Terwee et al’s
44
criteria. Measurement errors were determined by calculating the standard error of measurement (SEM) and minimal detectable change (MDC). The SEM was computed by multiplying the pooled standard deviation by the square root of 1 − ICC.
15
The formula 1.96 × SEM ×
To assess absolute reliability, Bland-Altman plots were utilized. No systematic bias was indicated when zero fell within the 95% CI of the mean difference between the first and second administrations of the P-LKS. The 95% CIs were determined using the formula: mean difference ± 1.96 × SDdiff, where SDdiff is the standard deviation of the mean difference between the initial and subsequent administrations of the P-LKS. 5
Results
Cross-cultural Adaptation and Translation Process
For the LKS scale, no notable inconsistencies were identified during the forward and backward translation processes. In the pre-evaluation phase with 20 patients, none reported difficulty in understanding the terms. Nonetheless, the expert committee refined the explanations to ensure they were as clear and straightforward as possible in Persian. The final translation of the P-LKS can be found in the Supplemental Material, available separately.
Patient Characteristics
A total of 100 patients with ACL tear who were admitted to our hospital between July 2022 and August 2023 were asked to participate in our study. The mean age of the participants was 35 ± 13 years (91 male and 9 female). Table 1 provides the overall and sex-specific characteristics of the patients. No participants were excluded because of missing data or changes in functional status when completing the questionnaires for the second time. Thus, the data from all 100 patients were utilized for analyses of validity, internal consistency, and test-retest reliability.
Patients Characteristics a

Values are presented as mean ± SD or n (%). BMI, body mass index.
Professional athletes have either competed at a national level or have previously participated in international competitions. On the other hand, recreational athletes engage in consistent participation in a nonorganized sport solely for personal enjoyment.
Feasibility
There were no notable instances of missing answers or language challenges for specific items in the questionnaire. On average, the P-LKS took patients 3 minutes to complete, with a time range of 2 to 5 minutes. Overall, patients found the questionnaire items pertinent to their physical activities and knee condition.
Floor and Ceiling Effects
The overall P-LKS exhibited acceptable floor and ceiling effects (≤15% of individuals affected). 44 While some patients achieved the maximum possible scores on each P-LKS item, this is inherent to single-question items, reflecting the patient's highest level of functionality. Table 2 illustrates the distribution of floor and ceiling effects for each domain of each questionnaire.
Score Distribution and Floor and Ceiling Effects of the P-LKS, SF-36, and IKDC-SF Questionnaires a

IKDC-SF, International Knee Documentation Committee Subjective Form; P-LKS, Persian Lysholm Knee Score; SF-36, 36-Item Short Form Health Survey.
These values have been converted to a scale of 0-100.
Internal Consistency
The Cronbach alpha for the P-LKS at the initial evaluation (α = 0.88) and during the test-retest (α = 0.85) demonstrated excellent internal consistency (Table 3).
Internal Consistency of P-LKS (Cronbach values) a

P-LKS, Persian Lysholm Knee Score.
Validity
Following analysis and evaluation by the knee surgeons, the questionnaire was deemed to have good content validity. The information obtained was sufficient to assess the functional state of ACL injury patients.
Four of the 5 predefined hypotheses concerning the correlation between the P-LKS and either the IKDC-SF scale or the SF-36 were confirmed (Table 4). There was a strong correlation between the overall P-LKS and the overall IKDC-SF score (r = 0.92), as well as with the subscales of the IKDC-SF score (r = 0.79-0.90). Among IKDC-SF domains, P-LKS showed the highest correlation with the symptoms domain. Additionally, the physical component of the SF-36 questionnaire (r = 0.85) and its physical-related domains, excluding physical health, showed excellent correlation with the overall P-LKS (r = 0.71-0.83). However, the mental component and other subscales exhibited moderate to very good correlation (Table 5).
Predefined Hypothesized and Actual Correlation Between Questionnaires a

IKDC-SF, International Knee Documentation Committee Subjective Form; P-LKS, Persian Lysholm Knee Score; SF-36, 36-Item Short Form Health Survey.
Hypothesis confirmed.
Construct Validity of P-LKS a

r shows correlation coefficient, P shows p-value, IKDC-SF, International Knee Documentation Committee Subjective Form; P-LKS, Persian Lysholm Knee Score; SF-36, 36-Item Short Form Health Survey.
Reliability
The ICC values for test-retest reliability are presented in Table 6. The P-LKS demonstrated high test-retest reliability (ICC = 0.97). Additionally, each item of the P-LKS exhibited excellent reliability (ICC = 0.82-0.99).
Reliability of P-LKS a

ICC, intraclass correlation coefficient; P-LKS, Persian Lysholm Knee Score.
Measurement Error
The values for the SEM, MDCind, and MDCgrp for the P-LKS were determined to be 1.04, 2.88, and 0.288, respectively. The Bland-Altman analysis revealed a mean difference of −0.98 between the 2 P-LKS assessments, with the 95% CI ranging from −12.6 to 10.6 (Figure 1). Because the 0 value fell within the 95% CI of the mean difference between the initial and follow-up scores, it was confirmed that there was no systematic bias, thus underscoring the robust test-retest reliability of the P-LKS.

Bland-Altman plot of the Persian Lysholm Knee Score (P-LKS) with the 2 solid lines representing the 95% CI and the dashed line representing the mean difference.
Discussion
The major findings of our study demonstrate that the construct validity was strong, with >80% of the predetermined hypotheses about the relationships between the P-LKS and other metrics being confirmed. The P-LKS showed a strong correlation with the Persian IKDC-SF (r = 0.92) and the physical aspect of the Persian SF-36 (r = 0.85). Reliability of the test-retest and the internal consistency of the P-LKS were excellent, with an ICC of 0.97 and a Cronbach alpha of .88. The floor and ceiling effects for the P-LKS total score were minimal, at 0% and 2%, respectively. Our study showed that the P-LKS has adequate psychometric properties regarding both validity and reliability. The obtained scores indicated satisfactory psychometric performance for most Iranian patients suffering from ACL tears. There were no issues encountered in the cross-cultural adaptation and translation of the questionnaires, and the back-translations matched the original English versions accurately.
The LKS is a frequently utilized self-reported assessment tool aimed at measuring outcomes for patients experiencing knee problems. This tool has undergone translation, validation, and cultural adaptation in multiple languages, showing strong internal consistency, test-retest reliability, and external validity †† (Supplemental Material; Table A1). Most studies have used the SF-36 questionnaire to assess the validity of the translated LKS.2,10,17,19,42,46
To assess the criterion validity of the translated questionnaires, the P-LKS was compared with the Persian versions of the IKDC-SF and SF-36. Previous cultural adaptation studies have similarly employed the IKDC-SF19,35,46 and SF-3610,17,46 for validation purposes. The P-LKS demonstrated a high correlation with the Persian IKDC-SF (r = 0.92) and physical component of SF-36 (r = 0.85), reflecting excellent validity. These validities are comparable with the previously translated versions in Thai, 25 Chinese, 46 and Dutch 19 languages, which showed that the correlation of LKS with IKDC-SF ranges from r = 0.83 to 0.89. The correlation of the LKS scale with SF-36 and IKDC-SF in various languages is depicted in Figure 2. ‡‡

Correlation of the Lysholm scale with (A) International Knee Documentation Committee (IKDC) and (B) 36-Item Short Form Health Survey (SF-36) in various languages.
The P-LKS exhibited acceptable levels of floor and ceiling effects. Notably, significant ceiling effects were observed in 7 out of the 8 items of the P-LKS. This occurrence is inherent to single-question items, which are designed to permit the highest possible scores, indicative of maximal functionality. The prevalence of ceiling effects across multiple items indicates that the total LKS score should be utilized instead of relying on scores of individual subscales. 19
The lowest ceiling effect was reported in the pain and instability domains, which shows the most common patient complaints. The high prevalence of pain among our population might be explained by the relatively high prevalence of associated meniscal injuries. There was a significant association between meniscal tears and level of pain, though the LKS is not meniscus specific (P = .03). The highest ceiling effect was encountered in the support domain, which was predictable because only patients with single-ligament ACL tears were included in the study.
The P-LKS demonstrated excellent test-retest reliability, with an ICC of 0.97. This ICC value for the P-LKS was higher than those reported in studies on some language versions, such as the Turkish (ICC = 0.82) 10 and Arabic (ICC = 0.80) 1 versions, which showed good reliability. However, similarly, excellent reliability was observed in Indonesian (ICC = 0.99), 17 Italian (ICC = 0.96), 11 and Greek (ICC = 0.95) 35 versions. The variability in ICC values may be attributed to the differing time intervals between the 2 assessments of the LKS scale. The interval between the test and retest should be sufficiently long to avoid recall bias, yet short enough to ensure there are no changes in patient characteristics relevant to the construct being measured, according to COSMIN guidelines 30 (Figure 3). §§ The ICC intervals for various studies are described in the Supplemental Material (Table A1).

Reliability of Lysholm scale in various languages (ICC score). ICC, intraclass correlation coefficient.
Our results revealed that the P-LKS exhibited satisfactory internal consistency with a Cronbach alpha value of .88. This value is comparable with previous studies, which ranged from .68 to .93,1,2,10,17,25 which indicates a good overall homogeneity of the scores. The translated versions in Turkish, 10 Arabic, 1 Greek, 35 and Thai 25 included participants with various knee disorders and demonstrated internal consistency values (α = .68-.90) similar to those found in the Persian, Chinese, 46 Dutch, 19 and Indonesian, 17 which specifically assessed patients with ACL injuries (α = .73-.88). These findings suggest that the diversity of the study population may not compromise the homogeneity of the scores (Figure 4).
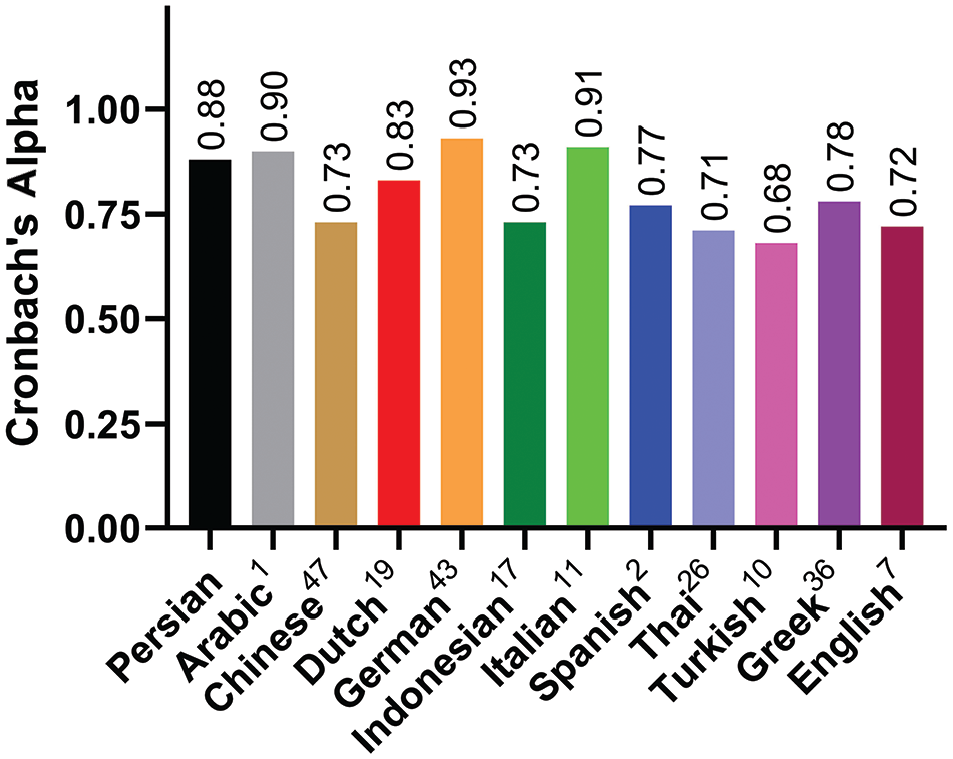
Internal consistency of Lysholm scale in various languages (Cronbach alpha).
The P-LKS indicated adequate sensitivity for group comparisons, as minimal values are needed to identify changes. The SEM of the P-LKS was 1.04, the MDCind was 2.88, and the MDCgrp was 0.29. These statistics are in line with those found in the Dutch version (SEM = 3.2; MDC = 8.9) 19 and German (SEM = 7.84; MDC = 21.72) 42 versions. Only differences exceeding the SEM can be considered beyond measurement error, indicating that to detect a statistically significant change in P-LKS scores, the difference must surpass the SEM. To differentiate from measurement error and confirm a real change, the difference between 2 measurements for individual patients should exceed the MDCind value of 2.88. The MDCind value equals 2.88, which makes it a suitable option for tracking individual patients’ progress over time. 17
Culturally adapted measures enable reliable multicenter studies and meta-analyses across diverse populations. The LKS scale has undergone cultural adaptation, translation, and validation in multiple languages. These investigations involving roughly 1000 patients have generally demonstrated the LKS’s acceptable validity and reliability. ‖‖ These findings corroborate the results of our study.
Limitations
There are several limitations to this study that should be acknowledged. First, this study only included patients with an ACL tear. Therefore, further studies are needed to use this questionnaire for various knee complaints. Second, this study was conducted solely in Tehran, the capital of Iran, a country with a diverse population. Additionally, it is worth mentioning that our study included a limited number of female participants. Finally, it's important to note that various minority groups speak different languages, which could affect the application of the questionnaires. We believe that the P-LKS can be effectively used for Persian-speaking patients with various knee pathologies, similar to its original version.
Conclusion
Our study demonstrated that the P-LKS successfully preserved the attributes of the original version. It can be regarded as a reliable tool for Persian-speaking patients with complete ACL tear.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671251327682 – Supplemental material for Psychometric Validation of the Persian Version of the Lysholm Score
Supplemental material, sj-pdf-1-ojs-10.1177_23259671251327682 for Psychometric Validation of the Persian Version of the Lysholm Score by Fardis Vosoughi, Iman Menbari Oskouie, Mir Saeed Yekaninejad, Yelverton Tegner, Arash Sherafat Vaziri, Sohrab Keyhani and Mehran Soleymanha in Orthopaedic Journal of Sports Medicine
Supplemental Material
sj-pdf-2-ojs-10.1177_23259671251327682 – Supplemental material for Psychometric Validation of the Persian Version of the Lysholm Score
Supplemental material, sj-pdf-2-ojs-10.1177_23259671251327682 for Psychometric Validation of the Persian Version of the Lysholm Score by Fardis Vosoughi, Iman Menbari Oskouie, Mir Saeed Yekaninejad, Yelverton Tegner, Arash Sherafat Vaziri, Sohrab Keyhani and Mehran Soleymanha in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted November 9, 2024; accepted November 20, 2024.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Tehran University of Medical Sciences (IR.TUMS.SHARIATI.REC.1403.068).
Data Accessibility Statement
The data sets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.